Full Length Research Paper

ABSTRACT
The effects of oral intake of capsaicin oleoresin (CO) on arterial blood pressure was examined in male spontaneously hypertensive (SHR) rats. Animals were randomized into control (C), capsaicin oleoresin (CO), capsaicin oleoresin-irbesartan (COI) and capsaicin oleoresin-amlodipine besylate (COAB) fed groups. The experimental groups received 50 mg of Capsaicin Oleoresin only, CO with 25 mg of Irbesartan, and CO with 2.5 mg of Amlodipine per kilogram of body weight every other day for 4 weeks. Blood pressure was measured weekly by tail-cuff for 4 weeks. Biological samples were obtained at baseline, day 18, and day 34 (terminal) for aldosterone, arginine vasopressin (AVP), renin, 6-Keto-PGF-1α, Prostaglandin E2, catecholamines, adrenocorticotropic hormone (ACTH) levels, and serum minerals. Statistical significance was set at p≤0.05. The results trended towards decreasing (p=0.190) systolic blood pressure (SBP) in the COAB and CO compared to the COI and control groups. However, significance among group differences were observed for urine aldosterone and AVP, and serum sodium, calcium, magnesium, potassium, and catecholamine (p≤0.05), but not for ACTH, renin, and 6-Keto-PGF-1α levels. Capsaicin treatment was non-significantly associated with decreased SBP in SHR. These findings suggested that the effects of Capsaicin on SPB may involve aldosterone and arteriolar vascular tone.
Key words: Capsaicin oleoresin, amlodipine besylate, irbesartan, arginine vasopressin, spontaneously hypertensive rats.
INTRODUCTION
Not only are the morbidity and mortality rates of hypertension high in many countries in the world, hypertension also affects people of every culture, gender, race, and socio-economic class. According to the Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure, hypertension is defined as an increase in the diastolic blood pressure (DBP) above 90 mm Hg and/or in systolic blood pressure (SBP) above 140 mm Hg. In addition, taking antihypertensive agents may satisfy the definition for hypertension (Chobanian et al., 2003). Physiological stress, heredity, nutrition, and hormonal imbalances are some of the factors that have been identified as contributing to hypertension (Lim et al., 2012; Syed et al., 2012; Kotchen, 2011). The roles of nutrition and hormonal imbalances in hypertension are widely known, and the research findings have resulted in the successful development of drugs to ameliorate the disorder.
Whereas, some common food constituents, such as sodium chloride (NaCl), have been found to exacerbate hypertension, others such as quercetin, have ameliorating effects (Sanchez et al., 2006). Capsaicin is the active ingredient in the genus Capsicum, commonly called chili. Their fruits, chili peppers, are consumed all over the world in different shapes and sizes and vary in the extent of the sensory heat produced by the irritation of mucus membranes (Okeahialam et al., 1998). Notably, these fruits have been used in the pharmaceutical industry as topical pain remedies and for drug development.
This study sought to test the hypothesis that Capsaicin has an arterial blood pressure (BP)-reducing effect that is amplified when combined with antihypertensive drugs, such as irbesartan (AT-1 angiotensin II receptor blocker (ARB) and amlodipine besylate (a slow calcium ion channel blocker) (CCB). When this study was conceived, the use of ARB’s and CCB’s was on the rise in West Africa, where Capsaicin was widely consumed based on non-scientific survey data (Salako et al., 1998).
There is now evidence that Capsaicin, acting through transient potential vanilloid receptor1 (TRPV1) channels, may facilitate the release of nitric oxide from vascular endothelial cells (Yang et al., 2010), thereby leading to vasorelaxation, and a decrease in blood pressure (BP). However, the extent to which capsaicin singularly reduces arterial BP and the possible benefit of the expected additive arterial BP reducing effect when combined with widely used antihypertensive drugs such as amlodipine besylate and irbesartan remain unknown. If indeed capsaicin reduced arterial blood pressure, it was also of interest to elucidate potential additional physiologic mechanisms mediating its effects.
To the authors’ knowledge, we are unaware of published data on the effect of orally administered capsaicin on blood pressure in combination with the anti-hypertensive agents, amlodipine besylate and irbesartan. Therefore, the purposes of the study were to determine the effects of orally administered capsaicin oleoresin on arterial blood pressure of spontaneously hypertensive rats (SHR), and to assess the interactive effects of capsaicin oleoresin with irbesartan (IRB) and amlodipine besylate on blood pressure.
METHODS
Research design
In this study, 40 12-week-old spontaneously hypertensive male rats (Harland Sprague Dawley, Indianapolis, IN) were used. The animals were randomly assigned to 4 groups of 10 rats each (3 treatment and one control groups): Capsaicin oleoresin - treated (CO); Capsaicin oleoresin and irbesartan - treated (COI); Capsaicin and amlodipine besylate - treated (COAB); and Control (C).
Animals and treatment
This study was approved by the Howard University Institutional Animal Care and Use Committee (IACUC). All procedures were conducted in accordance with the IACUC regulations. The rats were received from Harlan Laboratories at approximately 8 weeks of age, singly housed in wire mesh cages and quarantined for one week. Additional housing condition included controlled temperature (22 to 24°C), humidity (45 to 55%), and twelve-hour light (7:00 am to 7:00 pm) maintained with an automatic control system. The animals were habituated to the holding container and the tail-cuff blood pressure measurement occurred randomly twice per week for three weeks prior to baseline measurements. The animals were weighed on day one of the experimental period, and then weekly thereafter with an electronic balance (model 800, Whiteman Lab Sales, Inc., Hillsborough, OR). Indirect tail-cuff systolic blood pressure readings were measured with a non-invasive blood pressure and data acquisition system (Kent Scientific Corporation, Torrington, CT 06790 and DASYTEC USA Incorporated, Amherst, NH 03031, respectively) and recorded every week starting at baseline on day one. Blood and urine samples were collected for analyses at baseline and on days 18 and 34. Approximately 1 ml of blood sample was obtained by jugular venipuncture from each rat, and 12-hour urine samples were collected via metabolic cages at baseline and on days 18 and 34 of treatment. Following venipuncture, each rat received intracutaneously an amount of normal saline equivalent to the extracted blood volume.
The animals were fed the Teklad Global 2018 diet per the breeder’s recommendation, while water and food were permitted ad libitum prior to and during the study period. Net food intakes by weight were recorded every other day after subtracting net spillage. The control received only the basal diet and corn oil as a placebo based on average milligram per kg of body weight published data. The treatment groups COAB, COI, and COI received 50 mg of Capsaicin Oleoresin in separate feedings every other day for 4 weeks. In addition, the COI group received 25 mg of Irbesartan while the COAB received 2.5 mg of Amlodipine besylate within half an hour of receiving capsaicin oleoresin every other day in separate feedings. The irbesartan, amlodipine, and Capsaicin oleoresin were dissolved in 1 ml of corn oil, and each solution was delivered to the rats with a gavage needle and syringe, while the received 1 ml of corn oil as a placebo. Separate feedings were delivered via 20-gauge disposable gavage needles with syringes into the stomach. At the terminal stage, under anesthesia, the thoracic cavity of each rat was surgically accessed to obtain terminal blood samples
Biochemical analyses
Serum albumin levels were measured with ready to use reagents from Sigma Diagnostics, (St. Louis, MO). Plasma adrenocorticotrophic hormone (ACTH), 6-Keto-prostaglandine-F1α, and plasma renin were measured using immune-radiometric assay (IRMA) kits from Diagnostic Systems Laboratories Inc., (Webster, Texas). Urine Catecholamine and Prostaglandine-E2 kits from Amersham Pharmacia Biotech Inc., (Piscataway, NY); urine aldosterone and arginine vasopressin were measured with enzyme immunoassay (EIA) kits from Diagnostic Systems Laboratories Inc., (Webster, Texas). Serum sodium and potassium were determined by atomic emission spectroscopy, and magnesium and calcium were determined by atomic absorption spectroscopy (Perkin Elmer Model 500, Flame Atomic Absorption Spectrometer)
Statistical analysis
The Statistical Analysis System software 9.3and Statistical Analysis and Graphics were used to analyze the data. All p-values were two-tailed and significance (p) level for this study and was set at 5% (p ≤0.05) and confidence intervals (CI) computed at the 95% level. Statistical significance of the difference between physiological measure group means was analyzed by the non-parametric Kruskal-Wallis test for comparisons of non-normal continuously distributed data, equivalent to the parametric one-way analysis of variance (ANOVA). Scheffe’s multiple-range tests were performed when the group means of the physiological measures were significant.
RESULTS
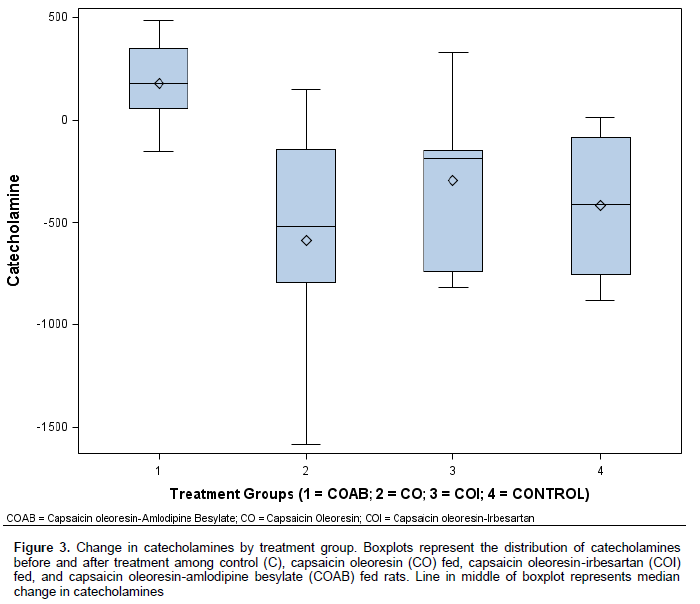
The mean changes from baseline in systolic blood pressure, diastolic blood pressure, and heart rate were compared statistically among the groups. A non-significant difference towards reduction in systolic blood pressure from baseline values was observed among the groups during the course of treatment (p=0.086) (Table 1). Mean changes in diastolic blood pressure and heart rates were not significantly different among the groups (p=0.888 and p=0.460 respectively). However, the COI group had an insignificant mean increase in DBP during the treatment period compared to baseline. The mean difference in the urine aldosterone output levels of the treatment groups were significantly lower than that of the control group (p=0.0001) (Table 2). The COAB group had the lowest change in urine aldosterone level, followed by the CO, and COI groups respectively (Figure 2).
.png)
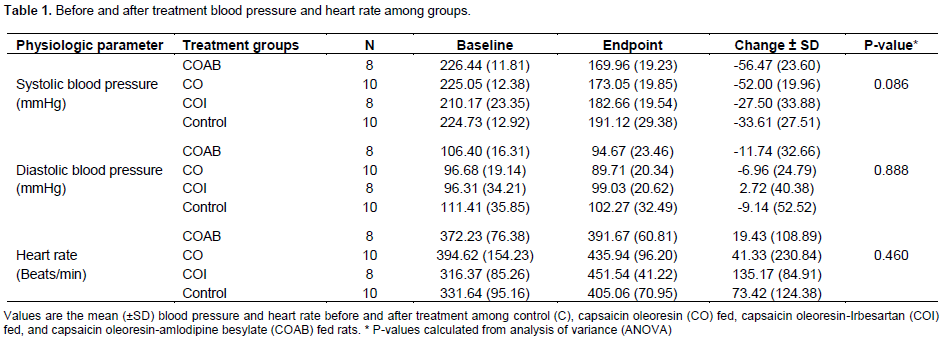
The urine AVP output of the COI group and the control decreased significantly (p=0.003) from baseline compared to that of the CO and COAB groups (Figures 1).
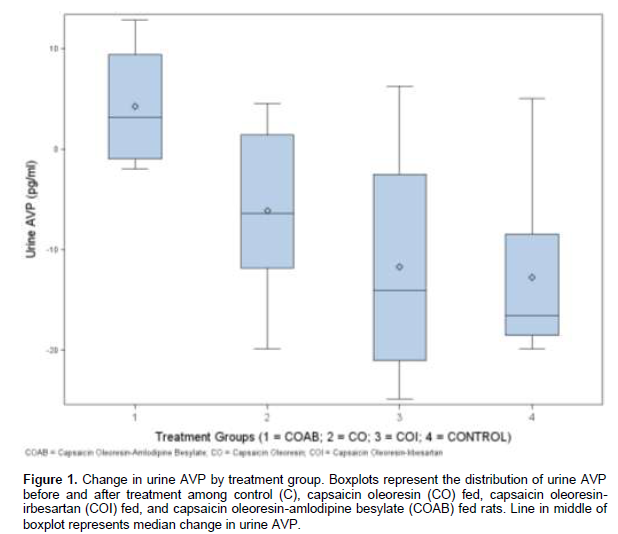

Urine output of catecholamine was significantly higher in the COAB group compared to the other treatment groups and the controls (p = 0.001). The CO, COI and the control group dropped from baseline. Plasma renin levels were not significantly different (p=0.273) among the groups (Table 2). Although the mean change in the plasma ACTH levels were similar among the groups (p=0.402) the mean difference in the plasma ACTH levels of the COI and control groups increased compared to those of the CO and the COAB groups. The urine output of both PGE2 and 6-Keto-PG1α increased from baseline. The upward trends were not however significant: PGE2 (p = 0.102) and 6-Keto-PG1α (p = 0.550.) (Figure 3).
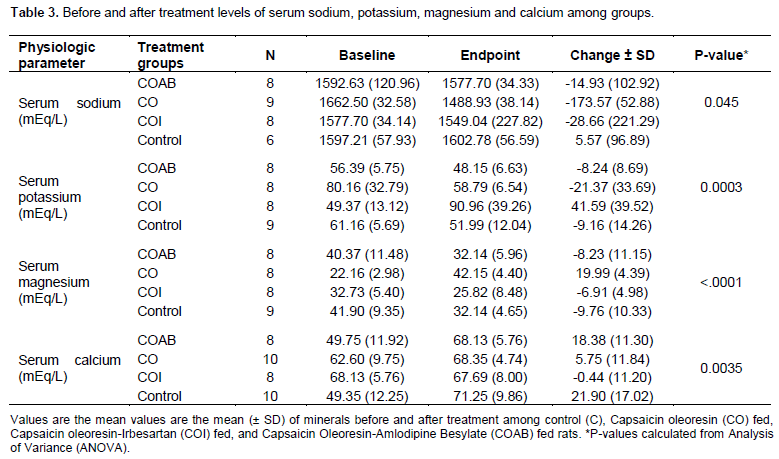
The change in the serum sodium level of the CO group was significantly different from those of the control, and the other treatment groups (p=0.045) (Table 3, Figures 4 and 5). The mean difference in the serum potassium level of the COI group was significantly different (p = 0.003) from those of the control, CO, and the COAB groups.
.png)

The change in the serum level of magnesium in the CO group was significantly different (p = 0.0001) from those of the control and other treatment groups. The serum level changes in calcium in the COI group was significantly different (p= 0.0004) from those of the other treatment groups and the controls. Serum calcium levels decreased in the COI group but increased in the control and among the other experimental groups (CO and COAB) (Figures 6 and 7).


DISCUSSION
In this study, the oral intake of capsaicin oleoresin alone and capsaicin oleoresin with amlodipine besylate non-significantly reduced systolic blood pressure of SHR compared to those of capsaicin with irbesartan and controls. The noted decrease in SBP is in accordance with the observation that the measured urine output of arterial pressor factors, such as AVP and its metabolites, decreased during treatment, except in the COAB group (Table 2, Figure 1). This observation is supported by evidence from the literature confirming that oral dietary capsaicin had SBP reducing effects, and in particular, that endothelial nitric oxide may mechanistically explain these effects (Yang et al., 2010).
The observed decrease in urine output of AVP in the CO, COI and controls, compared to increase in the COAB group, may suggest either a decreased AVP secretory activity in the CO, COI, and the control groups or decreased clearance of the circulating AVP. Interestingly, the pair with the greatest decrease in urine AVP output also had the smallest change in SBP from baseline, suggesting that the AVP axis may mechanistically explain the induction of hypertension in SHR rats (Paczwa et al., 1997; Bankir et al., 2005).
Among the groups, DBP decreased non-significantly, except for a marginal increase in the COI group, compared to baseline. These changes may be related to an intrinsic DBP reducing mechanism in the strain of SHR used in the study, or, alternatively, to drug combination effects or other unknown mechanisms. Interestingly, the COAB groups had a higher mean DBP than the COI, control and CO groups, perhaps because of amlodipine besylate’s known moderating effect on myocardial depolarization, and consequent reduced DBP and heart rate (Lexi-Comp, 2013).
In all the groups heart rate increased, but the mean between group differences were not statistically significant. Because increased sympathetic nervous system activity is a leading cause of increased heart rate and hypertension, this, in addition to reflex tachycardia, may explain our findings from this study (da Silva et al., 2009; Tsioufis et al., 2011; Santos and Carvalho, 2013).
The COAB group showed a significant increase in urine catecholamine output during treatment compared to the control and other treatment groups. The age-related decrease in urine outputs among the other groups suggest decreased systemic catalysis or decreased production within the adrenal medulla. Also, the COAB group had increased AVP excretion, a potent vaso-pressor. Epinephrine is a known vasoactive compound, and through its alpha and beta receptor activities can causes elevated SBP, increased ventricular contraction, and increased heart rate (Grassi et al., 2010;Toal et al., 2012). Also, epinephrine dilates the peripheral arteriolar vascular bed. This evidence suggests an intrinsic decline in the clearance of circulating catecholamine, or decrease in the production of catecholamine by the adrenal medulla. The later may partly explain the observed changes in SBP. In the COAB group, the converse would be the case but the exact mechanism is uncertain.
While the mechanisms are not completely understood, the observed urine aldosterone level in our study suggests a relationship between Capsaicin treatment and the stabilization of urine aldosterone output. The observed reduction among the experimental groups was stable within the margin of error compared to the sevenfold reduction demonstrated in the controls. Capsaicin treatment potentially resulted in the blunting of aldosterone release and activities, thus accounting for the reduction in urine aldosterone and its metabolites in the treatment group (Figures 2 and 3). Reduction in aldosterone catabolism results in volume retention, leading to an increase in SBP. A similar pattern is also seen with AVP urine out, thus confirming volume retention as a likely inducer of hypertension in SHR (Mironova, et al., 2015). Collectively, the observations are consistent with studies showing that the activation of adrenal afferent nerves in vivo attenuated aldosterone steroidogenesis, and that high levels of ACTH prevented this phenomenon (Ulrich-Lai et al., 2001).
The plasma renin levels of all the groups trended downward from baseline, and may point to an essential SBP control mechanism in SHR instead of a treatment effect (Volpe et al., 2012). Circulating levels of renin are directly related to the plasma angiotensin I level (Reid, 1998). In principle, SBP status is coupled to angiotensin II and III activity. Interestingly, irbesartan’s mechanism of action involves blocking angiotensin II activities receptors, which in turn regulates aldosterone.
The serum potassium level is regulated by aldosterone activity (Ikeda et al., 1994). The rise in serum potassium in the COI group may be partially related to the reduction of the angiotensin II potassium-regulating activity by irbesartan, leading to decreased potassium secretion in the renal collecting duct system. It is also possible that serum potassium derangement is part of a physiological mechanism of inducing hypertension in the SHR because the control group effectively demonstrated lower serum potassium. In support of the later observation, Hu et al. (2013), Kanbay et al. (2013) and Van Crombruggen et al. (2011) reported restoring normal SBP by re-establishing a normal potassium status in potassium-depleted rats. Additionally, limiting plasma renin activity and sensitization of the arteriolar vascular bed to catecholamines have been proposed as potassium-controlling mechanisms (Mulrow, 1999; Hu et al., 2013). These reports support observations from our experiment.
Adrenocorticotropic hormone (ACTH) levels were increased in all groups but not significantly. The changes in plasma ACTH did not appear to influence urine aldosterone. Another point to consider is the role of brain angiotensin II (Ang II), which is known to increase BP, serum sodium, AVP, and ACTH via the reduction of baroreceptor sensitivity and stimulation of sympathetic output, autonomous the renin-angiotensin-aldosterone system (Kanbay et al., 2013). The latter function explains the observed absence of distinct relationships among urine aldosterone output, plasma ACTH, serum sodium, and potassium (Figure 5).
Finally, the effects of the diurnal release of ACTH may not be fully accounted for in this study, as the blood samples were obtained in the evening to evaluate whether Capsaicin induced a sustained ACTH surge. Further studies to investigate the role of brain angiotensin II role in hypertension in SHR may be necessary.
The serum magnesium level increased significantly in the CO group but decreased in the other treatment groups and in the control group (Table 3). Results from several studies have affirmed the relationship between Mg2+and Ca2+ homeostasis and blood pressure regulation (Adrogue and Madias, 2014; Cunha et al., 2012; Sontia and Touyz, 2007). Since the observed decrease in serum magnesium included the control group, an age-related dysregulation of a native mechanism for magnesium homeostasis is suspected in hypertension induction in SHRs. The significant rise in the CO group’s serum magnesium level is interesting, given the trends among the other treatment groups and the control.
The serum calcium levels were essentially unchanged in the COI group, although they increased in the other treatment groups. Recent evidence implicates significantly low serum calcium level in hypertension (Ungvari and Koller, 2000; Huang et al., 2000). The increase in serum calcium is part of an overall native scheme for SBP control in SHR (Figure 6 and 7).
PGE2, a potent vasodilator, and 6-keto-PG1α, a stable metabolite of prostacyclin, a vasodilator, increased from baseline in all the groups but not significantly. The trend was uniform across the groups including the controls. It is unlikely that the cyclooxygenase pathways are involved significantly in the induction of hypertension of the rat strain used in this study. However, moderation of circulating prostaglandins with vasoconstrictory properties has been shown to mechanistically amelioration SBP in SHR (Ikeda et al., 1994; Huang et al., 2000).
Because no significant differences were found in food intake, body weights, or organ weights among the groups at baseline and after treatment, it appears likely that these factors may not have played a significant role in the outcome of the study.
CONCLUSIONS
Following treatment, we observed non-significant trends towards a reduction in systolic blood pressure (SBP) of the SHR groups that received capsaicin oleoresin (CO) and Capsaicin oleoresin-irbesartan (COI) compared to controls (C). The parameters measured appear to support, in part, the observed trend toward a reduction in systolic blood pressure, a marginal reduction in diastolic blood pressure, and an age-related increase in the heart rate, each of which is likely related to the brain-activated sympathetic system. Finally, it appears that the control of BP in the SHR species used in this study is multi-faceted. Capsaicin oleoresin seems to have both direct and additive effects of trending towards lowering SBP in SHR. Further studies are needed to explore the role of oral capsaicin intake in the induction of nitric oxide synthase activity, and therefore in the modulation of arterial blood pressure.
CONFLICT OF INTEREST
The authors declare that the research was carried out without any commercial or financial relationships that could be interpreted as a conceivable conflict of interest.
ACKNOWLEDGEMENTS
The authors thank Richard F. Gillum, MD, Doris Hughes, PhD, and Enid Knight, PhD of Howard University for their guidance; Dr. Felix Grissom of Howard University College of Medicine; and the USDA, Beltsville Research Center, Minerals Laboratory team, Dr. Kristine Patterson, Daniel Scholfield, and David Paul, for allowing us access to their laboratories for this study. Special thanks to Bristol-Meyers Squibb for donating the drug Irbesartan; to Pfizer Laboratories for donating the drug Amlodipine Besylate; and to Kalsec for donating the drug Capsaicin Oleoresin. Materials for this work were donated by Kalsec, Pfizer laboratories, Bristol-Meyers Squibb, and the USDA Agricultural Research Service.
REFERENCES
|
Adrogue HJ, Madias NE (2014). Sodium surfeit and potassium deficit: keys to the pathogenesis of hypertension. J. Am. Soc. Hypertens. 8(3):203-213. |
|
|
Bankir L, Fernandes S, Bardoux P, Bouby N, Bichet DG (2005) Vasopressin-V2 receptor stimulation reduces sodium excretion in healthy humans. J. Am. Soc. Nephrol. 16:1920-1928. |
|
|
Cunhan AR, Umbelino B, Correia LM, Fritsch M (2012). Magnesium and vascular changes in Hypertension Int. J. Hypertens. 754250. |
|
|
Chobanian AV, Bakris GL, Black HR (2003). The 7th Report of the Joint National Committee on the Prevention, Detection, Evaluation, and Treatment of High Blood Pressure (2003). U.S. Health and Human Services, National Institutes of Health, National Heart, Lung, and Blood Institute, National High Blood Pressure Education Program 2003 JAMA 289(19):2560-2571. |
|
|
da Silva A, doCarmi J, Dubinion J, Hall JE (2009). Role of sympathetic nervous system in obesity related hypertension. Curr. Hypertens. Rep. 11:206. |
|
|
Grassi G, Seravalle G, Quarti-Trevano F. The "neuroadrenergic hypothesis" in hypertension: current evidence (2010). Exp. Physiol. 95:581-6. |
|
|
Hu G, Xu X, Liang X, Yang X, Zhang J, Simayi Z, Chen Y (2013). Associations of plasma atrial natriuretic peptide and electrolyte levels with essential hypertension. Exp. Ther. Med. 5(5):1439-1443. |
|
|
Huang A, Sun D, Koller A (2000). Shear stress-induced release of prostaglandin H2 in the arterioles of hypertensive rats. Hypertension 35:925-30. |
|
|
Ikeda T, Gomi T, Sasaki Y (1994). Effects of swim training on blood pressure, catecholamines and prostaglandins in spontaneously hypertensive rats. Jpn. Heart J. 35:205-11. |
|
|
Kanbay M, Bayram Y, Solak Y, Sanders PW (2013). Dietary potassium: a key mediator of the cardiovascular response to dietary sodium chloride. J. Am. Soc. Hypertens. 7:395-400. |
|
|
Kotchen TA (2011). Hypertensive vascular disease Harrison's Principle of Internal Medicine, 18th edn. McGraw-Hill, New York. Drug Information Handbook: A Comprehensive Resource for Clinicians and Healthcare Professionals (2013.) 22nd edn. Lexi-Comp, Hudson, OH. |
|
|
Lim SS, Vos T, Flaxman AD (2012). A comparative risk assessment of burden of disease and injury attributed to 67 risk factors and risk factor clusters in 21 regions, 19902013: a systemic analysis for the Global Burden of Disease Study. Lancet 380:2224-60. |
|
|
Mironova E, Chen Y, Pao AC, Roos KP, Kohan DE, Bugaj V, Stockand JD (2015). Activation of ENaC by AVP contributes to the urinary concentrating mechanism and dilution of plasma. Am. J. Physiol. Renal Physiol. 308(3):F237-F243. |
|
|
Mulrow PJ (1999). Angiotensin II and aldosterone regulation Regul. Pept. 80:27-30. |
|
|
Okeahialam BN, Isamade EL, Ibrahim TM, Anjoorin FI (1998). The effect of lacidipine on patients with mild to moderate hypertension and the effect of a combination of lacidipine and hydrochlorothiazide in the treatment of hypertension uncontrolled after four weeks of lacidipine treatment: an open study. West Afr. J. Med. 17:42-46. |
|
|
Paczwa P, Budzikowski AS, Szczepanska-Sadowska E (1997). Enhancement of central pressor effect of AVP in SHR and WKY rats by intracranial N (G)-nitro-L-arginine. Brain Res. 748(1-2):51-61. |
|
|
Reid IA (1998). The renin-angiotensin system: physiology, pathophysiology, and pharmacology. Adv. Physiol. Educ. 20:S237-45. |
|
|
Salako BL, Kadiri S, Walker O, Fehintola FA (1998). Evaluation of lacidipine (a calcium blocker) in the treatment of hypertension in black African people: a double-blind comparison with hydrochlorothiazide. Afr. J. Med. Med. Sci. 27(1-2):73-75. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


