Short Communication

ABSTRACT
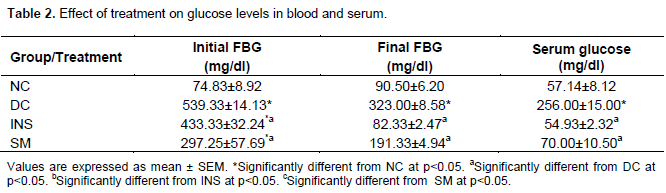
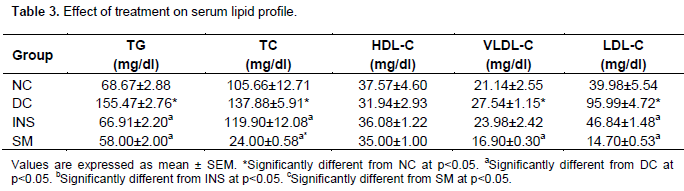
Lipid profile status of streptozotocin induced diabetic rats treated with ethanolic leaf extract of Solenostemon monostachyus was assessed. A total of 24 rats were used for the experiments and were divided into four groups (that is, Diabetic Control (DC), Normal Control (NC), Insulin Treated (INS) and S. monostachyus (SM) treated groups), with 6 rats each. The extract, 250 mg/kg body weight, was administered twice daily for 21 days. The serum glucose level in mg/dl was 70.00±10.50 for SM treated groups, 256.00±15.00 for DC. There was significant decrease at p>0.05 in blood glucose of rats administered with the extract. The lipid profile values for SM were triacylglycerol (TG, 58.00±2.00), total cholesterol (TC, 35.00±1.00), high density lipoprotein cholesterol (HDL-c, 35.00±1.00), very low density lipoprotein cholesterol (VLDL-c, 16.90±0.30), low density lipoprotein cholesterol (LDL-c, 14.70±0.53) and for DC were TG (155.47±2.76), TC (137.88±5.91), HDL-c (31.94±2.93), VLDL-c (27.54±1.15), LDL-c (95.99±4.72). The result for the lipid profile of SM treated groups showed significant decrease (P>0.05), when compared with DC groups. Based on the results obtained from this study, it may be concluded that the ethanolic leaf extract of SM has hypoglycaemic properties and was able to alleviate elevations in lipid profile and oxidative stress induced by streptozotocin in Wistar albino rats.
Key words: Solenostemon monostachyus, hypoglycaemic, oxidative stress.
INTRODUCTION
Origin of medicinal plant
According to medicinal history, Hippocratus was the first Greek to regard medicine as a science and was also called father of medicine. His “Material Medica” consisted essentially of herbal recipes, some of the medicinal plants described by Hippocratus, included opium, mint, etc., various preparations of aromatic roots and flowers in treating many ailments (Farnsworth and Morris, 1976). Galen in his middle ages was considered to be the most distinguished physician of antiquity after Hippocratus. He treated disease essentially by the use of herbs and those who followed his method eventually developed the sect known as “Electics” who employed herbs as well as mineral substances in treating the sick.
According to Treasure (2002), allopathic as well as homeopathic systems of medicine today are based on the doctrines expatiated by Galen. Historically, plants provide a source of inspiration for novel drug compounds. Medicinal plants have made large contributions to human health and wellbeing. Their role is in two fold in the development of new drugs: (1) they may become the base for the development of new drugs; (2) phyto-medicinal for the treatment of disease.
There are numerous examples of plant derived drugs. Some selected examples are isoquinolines, alkaloid, emetine obtained from the underground part of cephaclisipecacuanta and related species. Plant parts have been used for many years as amobicidal drugs as well as for the treatment of abscesses. Another important drug of plant origin with a long history of use is quinine, which is an alkaloid that occurs naturally in the bark of Ginchona tree. Apart from its continued usefulness in the treatment of malaria, it can also be used to relieve nocturnal leg cramps; Nelson (2002) found that higher plants have made important contribution in areas, such as cancer therapies.
Early examples include the anti-leukaemia alkaloids vinblatine and Vincristine which are both obtained from the Madagascan periwinkle plant. Solenostemon monostachyus could serve as a good supplement because of its hydrogen peroxide scavenging potential. Erythrocytes are the most abundant cells in vertebrates. Their unique morphology and physiological nature are exploited in drug delivery and targeting. Because of the preponderance of polyunsaturated fatty acids in the erythrocyte membranes, they are highly susceptible to oxidative damage whose consequences are lipid per-oxidation and haemolysis. This has been a mechanism for erythrocyte cell injury and death (Miki et al., 1987).
Erythrocyte haemolysis can be caused by some haemoglobinopathies, oxidative drugs and redox active metals (Ko et al., 1997). S. monostachyus is a prime candidate that could reverse the oxidative damages. The following compounds have been isolated from the leaves of S. monostachyus. They are the terpenoids β- pinene, oct- 1- en – 3-ol, β- caryophyllene, octan-3-ol, and E, E-α-farnesene (Eyele Mve et al., 2006). Dietary polyphenols, carotenoids and terpenes have also exhibited significant medicinal potentials (Wang et al., 2008).
Diabetes mellitus
Diabetes is a group of metabolic diseases in which a person has high blood sugar, because the pancreas does not produce enough insulin (WHO, 2006). This high blood sugar produces the classical symptoms of polyuria (frequent urination), polydipsia (increased thirst) and polyphagia (increased hunger).
Types of diabetes
There are three main types of diabetes mellitus (DM).
(1) Type 1 DM results from the body's failure to produce insulin, and presently requires the person to inject insulin or wear an insulin pump. This form was previously referred to as "insulin-dependent diabetes mellitus" (IDDM) or "juvenile diabetes".
(2) Type 2 DM results from insulin resistance, a condition in which cells fail to use insulin properly, sometimes combined with an absolute insulin deficiency. This form was previously referred to as non-insulin-dependent diabetes mellitus (NIDDM) or "adult-onset diabetes".
(3) The third main form, gestational diabetes occurs when pregnant women without a previous diagnosis of diabetes develop a high blood glucose level. It may precede development of type 2 DM.
Other forms of diabetes mellitus include congenital diabetes, which is due to genetic defects of insulin secre-tion, cystic fibrosis-related diabetes, steroid diabetes induced by high doses of glucocorticoids, and several forms of monogenic diabetes. All forms of diabetes have been treatable since insulin became available in 1921, and type 2 diabetes may be controlled with medications. Both types 1 and 2 are chronic conditions that cannot be cured. Pancreas transplants have been tried with limited success in type 1 DM; gastric bypass surgery has been successful in many with morbid obesity and type 2 DM. Gestational diabetes usually resolves after delivery. Diabetes without proper treatments can cause many complications. Acute complications include hypoglycaemia, diabetic ketoacidosis, or nonketotic hyperosmolar coma. Serious long-term complications include cardiovascular disease (CVD), chronic renal failure, and diabetic retinopathy (retinal damage). Adequate treatment of diabetes is thus important, as well as blood pressure control and lifestyle factors such as smoking cessation and maintaining a healthy body weight.
MATERIALS AND METHODS
Identification and preparation of plant
Fresh leaves of S. monostachyus were collected from Botanical garden at the University of Calabar, Calabar, Nigeria. The sample of the plant specimen was identified and authenticated by a Botanist from the botanical garden, and the voucher specimen was deposited in the herbarium of the same university. The leaves were sorted to eliminate any dead matter and other unwanted particles. The leaves were air-dried for 2 weeks and the leaves were blended with a manual hand blender and 150 g of the plant was weighed and soaked in 700 ml of ethanol. The mixture was then placed in a water bath at about 60 to 80°C for 10 min for thorough extraction of the plant active components and allowed to cool. The extract was then filtered with a chess material and later a Whatman no. 1 filter paper to obtain a homogenous filtrate. The filtrate was then concentrated in vacuo at low temperature of 37 to 40°C. The concentrate was then allowed open in a water bath for complete dryness. The extract was refrigerated at 2 to 5°C until when used. Appropriate concentration of the extract was subsequently made by dilution with distilled water into 250 mg/kg body weight and administered to the animals.
Handling and treatment of animals
A total of 24 adult male albino rats weighing between 150 and 250 g obtained from the disease free stock of the animal house, Biochemistry Department, College of Medical Sciences University of Calabar, Calabar, Nigeria, were used for the study. The rats were divided into four groups with six rats each, as follows: Group A (normal control group receiving distilled water as placebo), Group B (diabetic control group receiving distilled water as placebo), Group C (insulin group receiving 5 unit/kg body weight of insulin) and Group D (diabetic test group l received oral dose of S. monostachyus leaves extract juice). Table 1 The dose employed during administration was based on the predetermined LD50 values obtained from preliminary studies.

Induction of experimental diabetes
Prior to diabetes induction, the rats were subjected to 12 h fast, and then diabetes was induced by intraperitoneal injection of 40 mg/kg body weight with streptozotocin (STZ) (sigma St. Louis, Mo, U.S.A) using sodium citrate buffer (0.5M) reconstituted in dimethyl sulfoxide (DMSO). The normal control animals received DMSO only, three days after STZ treatment, diabetes was confirmed in STZ treated rats with a fasting blood sugar (FBS) concentration ≥ 200 mg/dl. This was estimated using One Touch Glucometer (Lifescan, Inc. 1996 Milpas, California, U.S.A) with blood obtained from the tail vein of the rats.
The rats were acclimatized in the experimental animal house for one week before the commencement of the experiment. The animals, housed in stainless steel cages under standard conditions (ambient temperature 28.0±2.0°C and humidity 46%, with a 12 h light/dark cycle), were fed with the normal rat pellets. All the rats in both test and control groups were allowed free access to food and water ad libitum, throughout the experimental period. Good hygiene was maintained by constant cleaning and removal of faeces and spilled feed from cages daily. The animals in test group III received insulin 5 unit/kg body weight and group IV received oral daily doses of aqueous extract of S. monostachyus leaves, respectively, using orogastric tubes and syringes. This lasted for a period of 21 days and the experiments were conducted between the hours of 7.00 am and 7.00 pm daily. Rats in the control groups I were administered, by oral gavage, with 5 ml of distilled water (placebo). All the animal experiments were carried out in accordance with the guidelines of the Institution’s Animal Ethical Committee (Table 2).
Collection and analysis of blood
All the animals were anaesthetized with chloroform vapour, twenty-four (24 h) after last day of extract administration, and dissected for blood collection. Blood samples were collected by cardiac puncture into a set of plain and fluoride oxalate sample bottles. The determi-nation of LD50/Acute toxicity tests was done orally using albino mice.
Biochemical tests were carried out, which include: liver enzymes-alanine aminotransferase and aspartate aminotransferase accor-ding to the method described by Reithman and Frankel (1957). Serum alkaline phosphatase was done using Randox test kits. Lipoprotein profile-total cholesterol was done using HDL-C, TG, serum electrolytes, urea and creatinine.
Statistical analyses
The results obtained from this study were analyzed by one-way analysis of variance (ANOVA), followed by Student’s t-test to evaluate the significance of the difference between the mean value of the measured parameters in the respective test and control groups using SPSS windows. A significant change was considered acceptable at P>0.05.
Changes in blood glucose of diabetic and non-diabetic test animals
Daily changes in blood glucose were monitored following daily treatment with extract and insulin in diabetic and non-diabetic rats. The blood glucose levels ranged between 60 and 108 mg/dl in the normal control rats (NC) that were not given any extract. Fasting blood glucose of other treatment groups varied differently. The treatment groups tended toward lowering the blood glucose levels when compared with the diabetic control (DC), but the S. monostachyus (SM) group was closely related to the insulin treated group. The diabetic control group range was between 601 and 295 mg/dl. Differences in DC showed sustained elevations in blood glucose level of untreated diabetic rats.
Effect of treatment on serum lipid profile
Changes in serum lipids concentration following treatment, in this investigation is as shown in Table 3. From the result, serum high density lipoprotein cholesterol (HDL-c) concentration in diabetic control rats which decreased non-significantly when compared with the non-diabetic control (NC) was increased in all diabetic treatment groups including the insulin group (INS). These increases were however non-significant (P>0.05). Serum concentrations of total cholesterol (TC) (155.47±2.76), triacylglycerol (TG) (137.88±5.91), very low density lipoprotein cholesterol (VLDL-c) (27.54±1.15) were significantly increased (P<0.05) in DC group when compared with the NC. Treatments with extracts of SM showed a significant decrease (P<0.05) in TG (58.00±2.00), TC (35.00±1.00), VLDL-c (16.90±0.30), low density lipoprotein cholesterol (LDL-c) (14.70±0.53) when compared with DC group.
DISCUSSION
Changes in serum lipids concentration in mg/dl following treatment, in this investigation is as shown in Table 3. From the result, serum high density lipoprotein cholesterol (HDL-c) concentration in diabetic control rats which decreased non-significantly as compared to NC was increased in all diabetic treatment groups including INS. These increase were however non-significant (P>0.05). Serum concentrations of TC (155.47±2.76), TG (137.88±5.91), and VLDL-c (27.54±1.15) were signi-ficantly increased (P<0.05) in DC when compared with the non-diabetic normal control group (NC). Treatments with extracts of SM showed a significant decrease (P<0.05) in TG (58.00±2.00), TC (35.00±1.00), VLDL-c (16.90± 0.30), LDL-c (14.70±0.53) when compared with DC group.
Type 2 diabetes is commonly associated with dyslipidaemia which is a risk factor for the development of CVD (Koffi et al., 2009). This is supported by our present study. From this study, there was a marked increase in the lipid content of serum in streptozotocin induced diabetic rat. This is due to the increased mobilization of free fatty acid (FFA) from peripheral depot (Krishnaveni et al., 2010). Interestingly, most of the studies with different plant extracts in diabetic rats were in agreement with our result (Ladan et al., 2007). The rise in serum TG, TC, VLDL, LDL and low HDL in this study indicate derangement of lipid metabolism and amplified incidence of cardiac dysfunction in diabetic rats. Insulin deficiency or resis-tance may be responsible for dyslipidaemia, because insulin has an inhibitory action on HMG-COA reductase, a key enzyme which is responsible for the metabolism of LDL particles rich in cholesterol. Administration of extracts of S. monostachyus showed significant decrease (p<0.05) in TC, LDL, VLDL, and TG. This alleviation denotes the anti-hyperlipidaemic potential of S. monostachyus.
S. monostachyus in reversing the elevation of LDL-c, TC, VLDL-c, TG and decreased HDL-c in hyperlipidaemic rats agrees with the findings of Adaramoye et al. (2005) for diabetic and hyperlipidaemic rats. The crucial risk factor for CVD includes a low level of HDL-c. The association between a low level of HDL-c and an increased risk of CVD has been well established through epidemiological and clinical studies. LDL-c is a primary target of CVD risk reduction therapy. LDL-c transports cholesterol mainly to the arterial wall. This results in the build-up of insoluble lipid on the wall of the arteries thereby reducing blood flow and increasing the pressure on the arterial wall as well as the heart. The deposition of the cholesterol on the arterial wall results in a condition known as arteriosclerotic plaque which is the major cause of CVD. CVD are the leading cause of death in developing countries (Latunde Dada, 1990). Hyper-cholesterolaemia has been identified as a primary risk factor in the development of CVD. This implies that, pre-venting or reducing the serum levels is associated with reducing risk of CVD. In contrast, HDL plays a direct role in the atherogenic process. Therapeutic intervention by raising HDL-c is widely encouraged. In this study, SM led to a significant increase of HDL-c, indicating its promising protective role against CVD. The protective role has been suggested to occur in various ways, HDL-c exert part of its anti-atherogenic effect by counteracting LDL oxidation. Recent studies also show that HDL promotes the reverse cholesterol transport pathway by inducing an efflux of excess accumulated cellular cholesterol and prevent the generation of an oxidatively modified LDL (Yokozawa et al., 2006). Furthermore, HDL inhibits the oxidation of LDL by transition metal ions, but also prevents 12-lipooxygenase-mediated formation of lipid hydro-peroxides. On the basis of the results of this study, SM may probably play an anti-atherogenic role through the inhibition of lipid oxidation as well as the elevation of HDL-c. People with higher levels of HDL-c seem to have fewer problems with CVD, while those with low HDL-c have increased rate of CVD. Some reports have shown that flavonoids, tannins and coumarin may play some role in antioxidant and hypolipidaemic effect (Ezekwe and Obidoa, 2001). The action of the plant extract in reducing plasma cholesterol concentration could be due to the ability of one or more of the phytochemicals in the plant to activate the functioning enzymes of the rat responsible for cholesterol absorption.
CONCLUSION
The results of this study show that the extract of SM can bring down the glucose levels in diabetic rats. Glucose levels of SM treated group decreased significantly when compared with the diabetic control group. The serum lipid profile level also decreased significantly when compared with the diabetic control group. Hence, we have come to the conclusion that this plant will be useful in the fight against diabetes.
ACKNOWLEDGEMENTS
The author’s would like to thank Prof. E. U. Udosen and Dr. F. E. Uboh for their support towards the success of this work.
CONFLICT OF INTEREST
Authors have not declared any conflict of interest.
REFERENCES
|
Adaramoye OA, Nanneri VO, Anyanwu KC (2005). Possible anti-atherogenetic effects of Kolaviron (a Garcinia kola seed extract) in hypercholesterolemia rats. Clin. Exp. Pharmacol. Physiol. 32(1-2):40-6. Crossref |
||||
| Ezekwe CI, Obidoa O (2001). Biochemical effect of Vernonia amygdalina on rat liver microsomes. Niger. J. Biochem. Mol. Biol. 16:1745-1798. | ||||
|
Farnsworth NR, Morris RW (1976) . Higher plants-the sleeping giant of drug development. Am. J. Pharm. Sci. Support Public Health 148(2):46-52. Pubmed |
||||
|
Ko FN, Hsiao G, Kao YH (1997). Protection of oxidative hemolysis by demethydiisoeugenol in normal and beta-thalassemic red blood cells. Free Rad. Biol. Med. 22:215-222. Crossref |
||||
|
Krishnaveni MS, Mirunalini K, Karthishwaran G, Dhamodharan N (2010). Antidiabetic and antihyperlipidermic properties of phyllanthusembicalinn (Euphobiaceae) on sterptozotocin induced diabetic rats. Pak. J. Nutr. 9:43-51. Crossref |
||||
|
Ladan MJ, Umar RA, Hassana SW, Shehu B (2007). Glycemic status and lipid profiles of diabetic in Sokoto, Nigeria. Asia. J. Biochem. 2:183-187. Crossref |
||||
|
Miki M, Tamai H, Mino M, Yamamoto Y, Niki E (1987). Free radical chain oxidation of rat Red blood cells by molecular oxygen and its inhibition by alpha- tocopherol. Arch. Biochem. Biophys. 258(2):373-80. Crossref |
||||
| Nelson KP (2002). Bacteriological and pharmacological studies of Madagascan periwinkle. Am. J. Pharm. 113-297. | ||||
|
Wang YC, Chuang YC, Hsu HW (2008). The flavonoid, carotenoid and pectin content In peels of citrus cultivated in Taiwan. Food Chem. 106:277-284. Crossref |
||||
| World Health Organization (WHO) (2006). Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycaemia. Geneva: WHO, Switzerland. P 646. | ||||
|
Yokozawa T, Cho EJ, Sasaki S (2006). The protective role of Chinese prescription Kangen-Karyu extract on diet – induced hypercholesterolemia in rats. Biol. Pharmacol. 29:760-765. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


