Full Length Research Paper
ABSTRACT
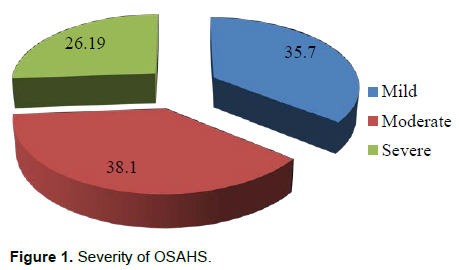
Obstructive sleep apnea hypopnea syndrome (OSAHS) is characterized by recurrent episodes of interruption of ventilation responsible for hypoxemia, hypercapnia and hyper activation of the autonomic nervous system. Hypoxemia followed by re-oxygenation promotes the formation of free radicals, oxidative stress and vascular inflammation, leading to endothelial dysfunction. The objective of this cross-sectional study conducted at the laboratory of Physiology of Gaston Berger University of Saint-Louis was to assess endothelial function during sleep apnea hypopnea syndrome. The endothelial function was explored non-invasively by Endopat 2000. Free and informed consent was required. Data analysis was carried out on Epi Info 7, uni-varied and bi-varied analyzes performed with a significance threshold p <5%. The study involved 42 patients including 69% women and 31% men. The average age was 52.11±8.31 years with a predominance of the (40-50yrs and 50-60yrs). The most frequently medical disorder was hypertension with 71.43%. Over 75% of the subjects were obese or overweight. OSAHS was mild in 35.71% of cases, moderate 38.1% and severe 26.19%. Endothelial dysfunction was found in 27.5% of the subjects. It was most noted in subjects with severe OSAHS, with no statistical significant difference. No significant association was found between endothelial dysfunction, gender, age and body weight. Endothelial function is often impaired during OSAHS. Studies on a larger sample should be done for more conclusive results.
Key words: Endothelial function, sleep apnea hypopnea syndrom, endopat.
INTRODUCTION
Obstructive sleep apnea hypopnea syndrome (OSAHS) is common and underdiagnosed, both in Africa and in the Western countries. In the adult population, the prevalence has been estimated between 3 and 7% for men and 2 to 5% for women in developed and developing countries (Escourrou and Roisman, 2010). The severity of the syndrom is based on apnea hypopnea index AHI measured by polysomnography and daytime sleepiness, excluding another cause of sleepiness. Thus, 3 stages are noted : light if 5 < AHI < 15 per hour, moderate if AHI between 15 and 30 per hour, severe if AHI > 30 per hour.
Various nonspecific clinical manifestations are reported, resulting from complete or partial obstruction of the upper airways responsible for sleep fragmentation, intermittent hypoxia, arousals and hypercapnie. Hypoxemia causes a decrease in oxygen supply to tissues, especially the myocardium. Changes in pressure increase the activity of the autonomic nervous system Hypoxemia followed by re-oxygenation promotes the formation of free radicals which cause oxidative stress and inflammation of the tissues, especially vascular cells. Oxidative stress and inflammation induce endothelial dysfunction. Metabolic and cardiovascular disorders are often associated with OSAHS including high blood pressure, coronary heart disease, stroke, atherosclerosis, myocardial ischemia, insulin resistance and metabolic syndrome, among others (Senaratna et al., 2017). Plasma adiponectin level decrease in OSAHS patients. The reduction of the secretion of adiponectin resulted from the activation of the sympathetic system. Adiponectin can exert multiple biological functions such as anti-inflammatory and anti-atherosclerosis activities, increase in sensitivity to insulin, decrease in insulinresistance and son (Zhang et al., 2006). Chronic intermittent hypoxia may result in pathological changes in cholesterol and triglyceride metabolism resulting in increased lipolysis and lipid biosynthesis (Celikhisar and Ilkhan, 2020).
High blood pressure causes functional alterations with enlarged smooth muscle cells and decreased endothelial function. This endothelial dysfunction results in an inhibition of nitric oxide production leading to less vasodilation during elevated vascular flow and increased vasoconstriction. Even in the absence of known cardiovascular disease, subjects with OSAHS would have increased arterial stiffness, impaired endothelial function and a high risk of cardiovascular disease.
In sub-Saharan Africa, the challenges in the diagnosis and management of OSAHS are important due to the ignorance of the syndrome, lack of polysomnography equipment, cost of sleep recordings and continuous positive pressure (Kashongwe et al., 2019). According to our knowledge, in Senegal, few studies related to obstructive sleep apnea-hypopnea syndrome OSAHS have been done. The objective of this study was to assess endothelial function in subjects with OSAHS.
MATERIALS AND METHODS
Study design
This study was conducted at the Physiology Laboratory of the Health Sciences Research and Formation Unit at Gaston Berger University, Saint-Louis, Senegal. This is a descriptive and cross-sectional study that took place over the period from January 15 to February 20, 2020. The protocol was established in accordance with the recommendations of the Helsinki declaration and approved by the Ethics Committee of the Faculty of Health Sciences of Cheikh Anta Diop University of Dakar, under the reference 0417/2019/CER/UCAD. All subjects had agreed to volontarily participate in the study by signing a free and informed consent form.
Study population
Forty two Senegalese patients participated in this study. They were recruited among the general population. The diagnosis of OSAHS was confirmed by polygraphy (CID-LXe, CIDELEC) for all patients, after a screening with the Berlin questionnaire (Netzer et al., 1999) and the Epworth sleepiness scale (Johns, 1991). The CID-LXe has 8 electrophysiological channels (3 electroencephalography EEG leads, one electrooculography EOG right and left eye lead, 2 anterior tibial electromyography EMG lead, one chin EMG lead and one electrocardiography ECG lead) and all of the airways (tracheal sound sensor and suprasternal pressure, oximeter sensor, thoraco-abdominal straps, a position sensor associated with an actimeter, and a nasal pressure measurement by a telescope) for a complete recording of sleep. It is equipped with the latest evolution of PNEAVOX technology (tracheal sound sensor) with a pneumotachograph option. Patients with pregnancy, mental health disorders or under psychotrope drugs were excluded.
Biochemical parameters and body composition
The biochemical parameters (fasting blood sugar, total cholesterol, HDL, triglycerides, serum iron, calcium levels, magnesemia, serum creatinine and azotemia) were quantified using the Cyan brand spectophotometer, Cyan Smart model. The LDL cholesterol level was calculated using Friedwald's formula:
LDL = total cholesterol - HDL - Triglycerides / 5 (in g/L).
A Tanita DC-360 impedance meter was used to determine the body composition, according to the required conditions.
Exploration of endothelial function
The exploration of endothelial function was done non-invasively by Endopat 2000 (Axtell et al., 2010). Patients were accommodated in a quiet, spacious, air-conditioned office with a comfortable bed. The examination procedure was explained to them with the 3 stages: pre-occlusion, occlusion and post-occlusion. They were told that during the period of occlusion, unwanted sensations such as tingling or heaviness of the limb may occur. They were warned that they should not move their fingers during the entire exam to avoid artifacts and ensure the reliability of the recordings. Jewelry and rings, especially metal, have been removed to avoid possible interference. Then they were placed in the supine position and asked to relax as much as possible.
Systolic and diastolic blood pressures were mesured manually using a validated sphygmomanometer (Omron) respecting the required conditions and the values mentioned on the patient sheet of the software. The inflatable cuff was positioned on the non-dominant arm, near the crease of the elbow. The Endopat biosensors were placed on the index fingers of both arms after checking the condition of the skin and the size of the nails. The test was easy and lasted 15 min. After recording the baseline for 5 min corresponding to the pre-occlusion phase, a 5-min vascular occlusion was performed by inflating the pneumatic cuff. After deflation, recording has been prolonged for 5 min.
The post-occlusive reaction was expected to manifest as endothelium-dependent dilatation, resulting in an increase in the amplitude of the PAT signal. A post-occlusion / pre-occlusion ratio was calculated by the Endopat software. The normal values of reactive hyperemia index (RHI) and its logarithm Ln were respectively 1.67 to 2 and 0.51 to 0.70. RHI and LnRHI values below 1.67 and 0.51, respectively, indicated endothelial dysfunction.
Statistical analysis
The statistical analysis were carried out using Excel and Epi Info version 7 software. The data were expressed as percentages and averages. For quantitative variables, means and the extremes were calculated. Univariate and bivariate analyses were performed, significance threshold was set at p<0.05, a p-value of less than 0.05.
RESULTS
Characteristics of the population
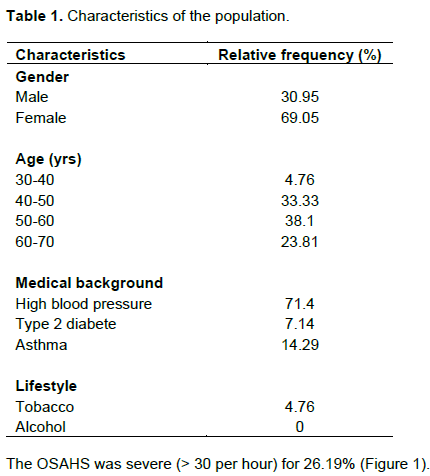
The study population consisted predominantly of women with a sex ratio of 2.23. The mean age was 52.11 ± 8.31 years; the median 53.5; mode 42 with extremes of 36 and 66. The age groups (40-50 and 50-60) were the most represented. The characteristics of the study population have been represented in Table 1.
Biochemical and bio-impedancemetric parameters
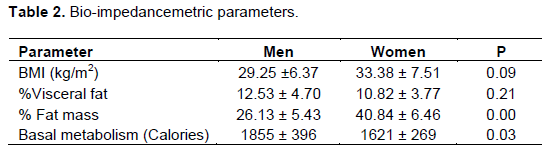
The majority of our subjects were obese. The mean body mass index (BMI) values were 29.25±6.37 kg/m2 and 33.38±7.51 kg/m2, respectively for men and women, without significant difference. The percentage of body fat was significantly higher in women. The bio-impedancemetric data are presented in Table 2.
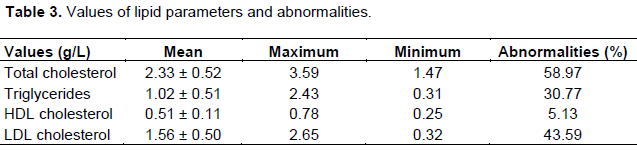
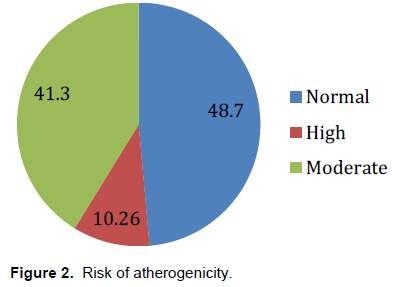
For biochemical parameters, fasting blood sugar was abnormal in 12.8% of cases. Renal function, assessed by serum creatinine and urea, was normal except for two subjects who had elevated serum creatinine. The most frequent ionic disorders were hypocalcemia and hypermagnesemia, in 60 and 25% of cases, respectively. The mean, maximum and minimum values of the lipid parameters are represented in Table 3, as well as the abnormalities observed. These were elevated total, LDL cholesterol, triglycerids and reduced HDL cholesterol. The risk of atherogenicity or the ratio of total cholesterol to HDL cholesterol was respectively elevated in 10.29% and moderated in 48.72% of cases, as shown in Figure 2.
Endothelial function
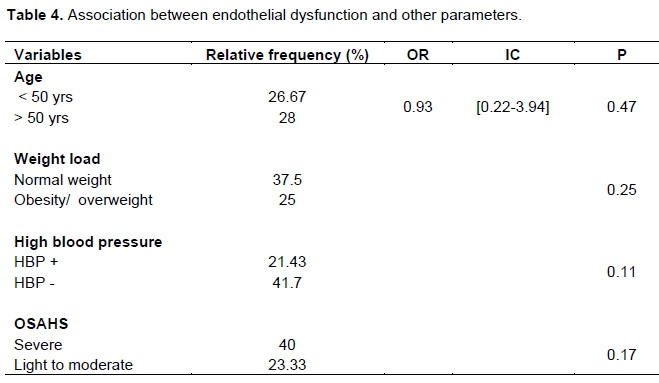
In 27.5% of subjects, an endothelial dysfunction has been observed with a Ln RHI <0.5. The mean of Ln RHI was 0.64±0.25 for women and 0.71±0.24 for men, with no significant difference (p = 0.47). No statistical significant association was noted between endothelial dysfunction and other variables such as age, weight, percentage of visceral fat, severity of OSAHS, presence or absence of hypertension (Table 4).
DISCUSSION
We noted in patients with OSAHS endothelial dysfunction, especially in those with severe OSAHS. Several studies have reported an alteration of endothelial function during OSAHS (Budhiraja et al., 2007; Hoyos et al., 2015). Endothelial dysfunction contributes substantially to the pathogenesis of cardiovascular disorders (Wang et al., 2015). It is a predictive marker of cardiovascular events and atherosclerosis. The association between endothelial dysfunction and OSAHS results from intermittent hypoxia with re-oxygenation, leading to reduced NO bioavailability, increased oxidative stress, systemic inflammation, and sympathetic activity. The secretion of reactive oxygen species (ROS) due to repeated re- oxygenations hypoxia explains endothelial dysfunction and associated micro-vascular disorders.
In addition, a study carried out in type 2 diabetics with OSAHS did not show correlation between endothelial dysfunction and the severity of OSAHS (Bironneau et al., 2017). In a randomized controlled trial which included 150 patients with severe OSAHS, without associated cardiovascular disease and with 5% type 2 diabetes, the mean RHI value was 2.15. The RHI value obtained was slightly lower, but without significant difference between the different apnea hypopnea index (AHI) groups (Bironneau et al., 2017). Another study showed the lack of association between OSAHS and endothelial function assessed by RHI in obese subjects (Araujo, 2015). Studies have suggested an improvement in endothelial dysfunction in patients with severe OSAHS, after 3 months, under continuous positive pressure (Azuma et al., 2015).
In one study, severe OSAHS was reported to be associated with endothelial dysfunction independently of obesity and serum adiponectin level. It would be interesting to perform serum assays for endothelial dysfunction markers such as endocan, a proteoglycan secreted by the vascular endothelium and involved in endothelial dysfunction and inflammatory processes (Kanbay et al., 2018). We observed disturbances in lipid metabolism in our study. Numerous disturbances in lipid metabolism have been reported in patients with OSAHS, including increased total cholesterol, LDL - cholesterol and triglycerides, decreased HDL - cholesterol, impaired oxidative capacity of HDL - cholesterol and increased lipid peroxidation (Bosshard and Sériès, 2008; Nadeem et al., 2014). Chronic intermittent hypoxia is the main factor behind dyslipidemia, systemic inflammation, oxidative stress, endothelial dysfunction and atherosclerosis (Adedayo et al., 2014).
In our study, hypermagnesemia was the main ionic disorder observed. Data were contradictory. In OSAHS, oxidative stress and inflammation may be followed by alteration of trace elements and heavy metals. Levels of cadmium, cobalt, iron, manganese, lead, magnesium and zinc were significantly higher in affected subjects (Asker et al., 2015). An other study had shown lower level of magnesium in patients with OSAHS (Karamanli et al., 2017).
Our study had some limitations. It was not possible to conclude formally that there was no significant correlation between the severity of OSAHS and endothelial dysfunction due to the small sample. In addition, it was difficult for these patients with associated cardiovascular risk factors such as obesity, hypertension, diabetes or dyslipidemia to distinguish between what would come under the apnea syndrome or these comorbidities.
CONCLUSION
Our study shows that endothelial dysfunction has been observed in patients with OSAHS. This endothelial dysfunction could increase the occurrence of cardiovascular complications in these subjects. Further, larger-scale research is needed to confirm early vascular alterations in OSAHS.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
The authors appreciate the "L'Oréal-UNESCO for Women in Science" Sub-Saharan Africa Program, the Ousmane Ngom health district in Saint-Louis and the Health Sciences Department of Gaston Berger University.
REFERENCES
|
Adedayo AM, Olafiranye O, Smith D, Hill A, Zizi F, Brown C, Girardin JL (2014). Obstructive sleep apnea and dyslipidemia: evidence and underlying mechanism. Sleep breath 18(1):13-18.? |
|
|
Araujo Lda S, Fernandez JF, Klein MR, Sanjuliani AF (2015). Obstructive sleep apnea is independently associated with inflammation and insulin resistance, but not with blood pressure, plasma catecholamines and endothelial function in obese subjects. Nutrition 31(11-12):1351-7. |
|
|
Asker S, Asker M, Yeltekin AC, Aslan M, Demir H (2015). Serum levels of trace minerals and heavy metals in severe obstructive sleep apnea patients: correlates and clinical implications. Sleep breath 19(2):547-52. |
|
|
Axtell Al, Gomari FA, Cooke JP (2010). Assessing endothelial vasodilator function with the Endo-PAT 2000.?Journal of visualized experiments: JoVE (44).. |
|
|
Azuma M, Chihara Y, Yoshimura C, Murase K, Hamada S, Tachikawa R, Matsumoto T, Inouchi M, Tanizawa K, Handa T, Oga T, Mishima M, Chin K (2015). Association between endothelial function (assessed on reactive hyperemia peripheral arterial tonometry) and obstructive sleep apnea, visceral fat accumulation and serum adiponectin. Circulation Journal 79(6):1381-9. |
|
|
Bironneau V, Goupil F, Ducluzeau, P. H., Le Vaillant, M., Abraham, P., Henni S, Gagnadoux, F (2017). Association between obstructive sleep apnea severity and endothelial dysfunction in patients with type 2 diabetes. Cardiovascular diabetology 16(1) :1-10. |
|
|
Bosshard V, Sériès F (2008). Syndrome d'apnée hypopnée obstructive du sommeil : facteur de risque pour le développement d'un syndrome métabolique? Médecine des maladies métaboliques 2(2):104-109. Doi : MMM-03-2008-2-2-ENCOURS-101019-200802623. |
|
|
Budhiraja R, Parthasarathy S, Quan SF (2007). Endothelial dysfunction in obstructive sleep apnea. Journal of Clinical Sleep Medicine, 3(4) : 409-415.?PMID: 17694731. |
|
|
Celikhisar H, Ilkhan GD (2020). Alterations in serum adropin, adiponectin and pro inflammatory cytokine levels in OSAS. Canadian Respiratory Journal 2020:2571283. Doi : 10.1155/2020/2571283. PMID : 32454912. |
|
|
Escourrou P, Roisman GL (2010). Epidémiologie du syndrome d'apnées hypopnées obstructives du sommeil de l'adulte et de ses complications. Médecine du sommeil 7(4) :119-128.? |
|
|
Hoyos CM, Melehan KL, Liu PY, Grunstein RR, Philipps CL (2015). Does obstructive sleep apnea cause?endothelial dysfunction? A critical review of the literature. Sleep medicine reviews, 20, 15-26.. |
|
|
Johns MW (1991). A new method for measuring daytime sleepiness : the Epworth Sleepiness Scale Sleep. Sleep 14:540-5. |
|
|
Kanbay A, Ceylan E, Köseoglu HI, Caliskan M, Takir M, Tulu S, Cakili OT, Köstek O, Erek A, Afsar B (2018). Endocan : a novel predictor of endothelial dysfunction in obstructive sleep apnea syndrome. Clin Respir J 12(1):84-90. |
|
|
Karamanli H, Kizilirmak D, Akgedik R, Bilgi M (2017). Serum levels of magnesium and their relationship with CRP in patients with OSA. Sleep breath 21(2):549-556. PMID: 27600660. |
|
|
Kashongwe IM, Kayembe JMN, Kashongwe M, Tete BO, Adambounou S, Adjoh S, Neino MA, Agodokpessi G, Ouédraogo M, Sumaili EK (2019). Syndrome d'apnées obstructives du sommeil (SAOS) en Afrique subsaharienne: revue de la littérature, état des lieux et perspectives. Ann Afr Med 12(2):e3257-3261.? |
|
|
Nadeem R, Singh M, Nida M, Waheed I, Khan A, Ahmed S, Naseem J, Champeau D (2014). Effect of obstructive sleep apnea hypopnea syndrome on lipid profile: a meta-regression analysis. Journal of Clinical Sleep Medicine, 10(5):475-489. PMID : 24910548. |
|
|
Netzer NC, Stoohs RA, Netzer CM, Clark K, Strohl KP (1999). Using the Berlin questionnaire to identify patients at risk for the sleep apnea syndrom. Annals of internal medicine 131(7):485-491. |
|
|
Senaratna CV, Perret JL, Lodge CJ, Lowe AJ, Campbell BE, Matheson MC, Hamilton GS, Dharmage SC (2017). Prevalence of obstructive sleep apnea in the general population: a systematic review. Sleep medicine reviews, 34:70-81. PMID: 27568340. |
|
|
Wang J, Yu W, Gao M, Zhang F, Gu C, Yu Y, Wei Y (2015). Impact of obstructive sleep apnea syndrome on endothelial function, arterial stiffening and serum inflammatory markers: au updated meta-analysis and?metaregression of 18 studies Journal of the American heart association, 4(11) :e002454.. PMID: 26567373. |
|
|
Zhang XL, Yin KS, Wang H, Su S (2006). Serum adiponectin levels in adult male patients with obstructive sleep apnea hypopnea syndrome. Respiration 73(1):73-77. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


