Full Length Research Paper

ABSTRACT
Globally, malnutrition among adolescents is a major public health concern. Despite the emergence of a number of advancements in areas of health and nutrition services in developing countries including Ethiopia, nutritional status of adolescents is not yet commonly included in health and nutrition surveys and an up-to-date overview of their nutritional status across the world is not available. Even the existing studies conducted on nutritional status of adolescents in Ethiopia and other parts of the world overlooked the pastoral and agro-pastoral area contexts. Thus, the objective of this study was to assess nutritional status and associated factors among adolescents of pastoral and agro-pastoral communities. Comparative cross-sectional study was conducted at Mieso Woreda on 655 primary school adolescents selected by multistage random sampling. Data were collected by face-to-face interview using pre-tested structured questionnaire and anthropometric measurements. Bivariate and multivariate binary logistic regressions were conducted to identify independent predictors of stunting and thinness (wasting). The overall magnitude of stunting and thinness were 11.5 and 22.9%. The magnitude of stunting was higher in agro-pastoral (14.5%; 95%CI: 10.7-18.3%) than pastoral (8.3%; 95%CI: 5.3-11.3%) communities. Meanwhile the magnitude of thinness was higher in pastoral (26.2%; 95%CI: 21.4-31.0%) than agro-pastoral (19.6%; 95%CI: 15.3-23.9%) community. Stunting was significantly associated with place of residence, sex, age, family size, source of drinking water, wealth tertiles and child food insecurity. Meanwhile thinness was significantly associated with family size, the source of drinking water, availability of latrine, household wealth tertiles, washing hands with soap after toilet, diarrheal illness and child food insecurity. The study revealed significantly higher magnitude of stunting in agro-pastoral communities and higher magnitude of thinness in pastoral communities though not significant. Interventions should focus on factors identified in this study to reduce magnitude of malnutrition among adolescents.
Key words: Stunting, wasting, school adolescents, pastoralist, agro-pastoralist, Somali.
INTRODUCTION
As defined by WHO, adolescents are individuals between the ages of 10 and 19 years, which make up approximately 20% of the world’s population. Adolescence is a time of intense growth, second only to infancy (Cordeiro et al., 2005; WHO, 2006). During adolescence, individuals can gain 15% of their ultimate adult height and 50% of their adult weight. This rapid growth is accompanied by an increase in nutrient demand (Cordeiro et al., 2005).
Nutrition is a basic human need that remains unmet for vast numbers of adolescents, who are thus unable to achieve their full genetic developmental potential (Cordeiro et al., 2005). Adolescents are the future generation of any country and their nutritional needs are critical for the wellbeing of society. Good nutrition during adolescence is critical to cover the deficits suffered during childhood. If adolescents are well nourished, they can make optimal use of their skills, talents and energies today, as well as be healthy and responsible citizens and parents of healthy babies tomorrow (WHO, 2006).
Adolescents are vulnerable groups for malnutrition and its consequences, because it is the dynamic period of physical growth and mental development. Globally, malnutrition among school age adolescents is a major public health concern. Nutritional status has powerful influence on an adolescent’s learning and how well the adolescent performs in school. Literatures show that there is strong link between nutrition and academic performance of adolescents. Both acute and chronic malnutrition (under nutrition) impairs children’s ability to perform effectively at school (The Partnership for Child Development, 1997). According to many researchers, poor nutritional status in primary school-age adolescents is among the most common causes of low school enrollment, high absenteeism, early dropout and unsatisfactory classroom performance (Andrews, 2013; The Partnership for Child Development, 1999; Walker et al., 2007). In Ethiopian context, focusing on school age adolescents is particularly pertinent as this age group represent more than 30% of the total population (Demographics of Ethiopia, 2014).
Although adolescence is a time of enormous physiological, cognitive, and psychosocial change, they remain “a neglected, difficult-to-measure and hard-to-reach population”. Most studies of malnutrition in developing countries have concentrated on young children or on the pregnancy period, thus neglecting adolescents (Cordeiro et al., 2005).
The concept of nutrition and its manifestation as malnutrition, involves complex processes at multiple levels, from the individual to the household, community, national and international levels. Besides poverty, there are other factors that directly or indirectly affect the nutritional status of adolescents (Cordeiro et al., 2005). Conditions such as food security, clean water, safe sanitation facilities, hygiene practices, maternal care practices and access to health services can have impact on overall nutrition status of adolescents (Benson, 2005). However, the relative importance of these factors may vary from area to area. In Ethiopia, these may include cultural and environmental factors as the country has a habits and practices are highly diversified (Abera, 2016). The livelihood of societies is also another factor that affects nutritional status of their members. There is severe poverty level in pastoralist than agro-pastoral societies (Adugna and Sileshi, 2013) because pastoralists are dependent only on herding and agro-pastoralists practice both herding and land cultivation. Thus, we hypothesized that there may be a difference in nutritional status of school adolescents between pastoral and agro-pastoral communities.
Despite the emergence of a number of advancements in areas of health and nutrition services in developing countries including Ethiopia, nutritional status of adolescents is not yet commonly included in health and nutrition surveys and an up-to-date overview of their nutritional status across the world is not available (Uauy et al., 2008; Walker et al., 2007). They were not included in Ethiopian Demographic and Health Surveys (EDHS) which provide nutritional status data of children under five-years-old at national and regional levels (Black et al., 2008). The existing studies conducted on nutritional status of adolescents in Ethiopia and other parts of the world also overlooked the pastoral and agro-pastoral area contexts (Assefa et al., 2013; Cordeiro et al., 2005; Dambhare et al., 2010; Gebreyohannes et al., 2014; Mulugeta et al., 2009; WHO, 2006; Wolde et al., 2014). Therefore, taking this into account, the aim of the present study was to assess nutritional status and identify associated factors among primary school adolescents of pastoral and agro-pastoral communities of Mieso Woreda, Somali Region, Ethiopia, to focus the attention of policy makers towards this group.
MATERIALS AND METHODS
Study design, area and period
Comparative cross-sectional study was conducted from March 10 to April 11, 2014 at Mieso Woreda, Shinele Zone, Somali Region. The woreda (administrative district) is located at a distance of 327 and 312 km from the capital of the region, Jigjiga town, and the capital of the country, Addis Ababa city (Figure 1). The woreda is typically rural and organized into 10 administrative kebeles. It is characterized by pastoral and agro-pastoral livelihood of the society. Ecologically agricultural, the Mieso Woreda is divided in to dry mid-highland, semi-arid and arid zones. Information is not available on the land area and rainfall of Mieso Woreda. The woreda had an estimated total population of 85,570 (47,589 males and 37,981 females) in 2013 which was projected from 2007 population census. The woreda had a total of 11 primary schools (6 serving grades 1-6 and 5 full cycle primary schools; that is, grades 1-8) and 1 general and upper secondary school (grade 9-12 ) in 2013 to serve an estimated 20,218 (11,243 males and 8,974 females) school age children. There were 3 health centers and 10 health posts in the woreda though the facilities were not equipped with necessary medical supplies, equipments, pharmaceuticals and even some were nonfunctional. The woreda had seasonal roads because of its topographical features.

Participants and sampling procedures
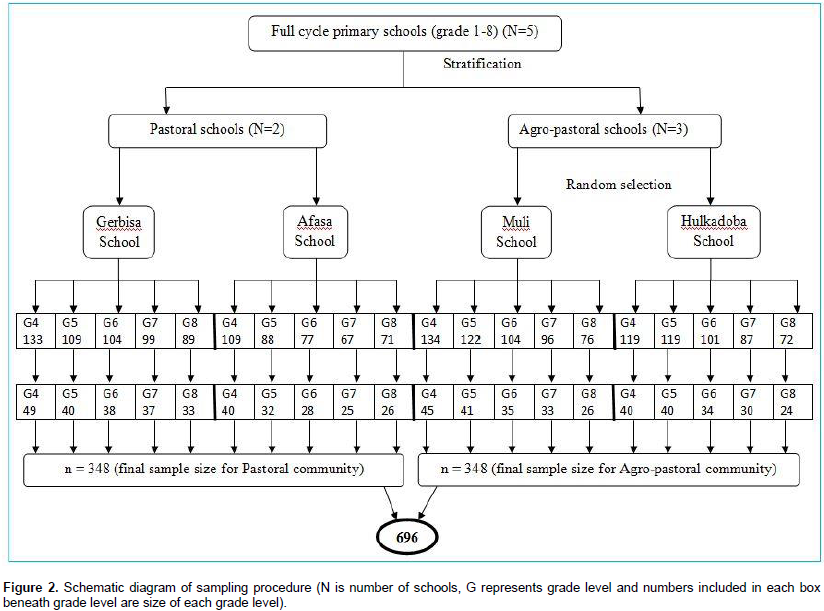
Study participants were sampled 10-19 years old students attending grades 4 to 8 at full cycle primary schools mentioned previously and who had no physical deformity or chronic illness. Sample size was determined by double population proportion formula using EpiInfo Software. 23.1% prevalence of wasting were assumed (Hall et al., 2008) among school children of agro-pastoral community, 10% difference in prevalence of wasting between the two communities which gave 33.1% prevalence of wasting among school children of pastoral community, 5% type I error (a), 80% power, 10% non-response rate and equal sample size as the two communities had nearly equal size of school children population. Thus, the final sample size was 348 for each community.
Participants were selected by multistage random sampling from each community. First, two schools were randomly selected from each community. Then, study participants were randomly selected, proportional to the size of each grade level (Figure 2). Selected participants were classified as pastoral or agro-pastoral within same school by asking them the livelihood of their family.
Variables, data collection procedure and measurement
Outcome variable was malnutrition (Stunting assessed by Height-For-Age and Wasting/Thinness assessed by BMI-For-Age) whereas independent variables included socio demographic/economic characteristics (age and sex of the child, parents’ educational level and occupation, head of the household, family size, type of family, number of siblings, religion, ethnicity, wealth and place of residence), health status (sickness in the last 2 weeks and type of illness (diarrhea, fever, cough and others)), feeding practice (breakfast intake, meal frequency per day, adolescent food insecurity), environmental factors (source of drinking water, availability of latrine at home, hand washing practice at critical times).
Data were collected by face-to-face interview using a structured questionnaire which was developed after reviewing different literatures of similar studies. The questionnaire was prepared in English, translated to Somali language and back translated to English to check consistency. Questionnaire was pre-tested on 5% of the sample in both communities and necessary corrections were made accordingly. Eight BSc Nurses who speak Somali were data collectors and there were also two BSc Health Officers supervising the data collection. Two days training was given for the data collectors and supervisors. Overall process of data collection was supervised by principal investigator.
Data were collected from adolescent students. To reduce the possible recall bias on age of the school adolescents, school age records were used and cross-checked with parents’ response. Weight was measured using a well calibrated Seca digital scale to the nearest 0.1 kg and height was measured using measuring board with a moveable headboard to the nearest 0.1 cm. Height measurement was taken while the participant was barefoot.
Adolescent’s food insecurity was measured using a four item index adopted from household food security questionnaires used in developing countries (Frongillo and Nanama, 2006). Adolescents were asked four food security questions. These were whether in the last three months adolescent (1) had ever worried about having enough food, (2) had to reduce food intake because of shortages of food or money to buy food, (3) had to go without having eaten because of shortage of food or money to buy food and (4) had to ask outside the home for food because of shortage of food or money to buy food. A “Yes” response to food security question was labeled to have score of “1” and “No” was labeled to have score of “0”.
The values were summed to produce a food insecurity index. The index of food insecurity is defined as the number of items with a positive answer. The index was dichotomized as “food insecure” for adolescents having a value of 1 and above and “food secure” for those who had a value of 0. The index has high internal consistency (Cronbach’s Alpha=0.82) which is above the cut off point for reliability (Nunnally, 1978).
Household wealth was assessed by the adolescent’s reporting of ownership of asset items consisting of animal assets (Goat, Cattle, Camel, Donkey, Ox), ownership of house, and ownership of farming land; all commonly used as an indication of wealth status in the study area.
Data processing and analysis
Data were entered into EpiData 3.4, exported to SPSS 20, cleaned, explored and recoded before analysis. BMI was calculated by dividing weight in kilogram by square of height in meters. Anthropometric indices (Height-For-Age and BMI-For-Age) were calculated by WHO AnthroPlus software 1.0.4 using WHO child growth references.
Principal component analysis was done and the results were converted into tertiles and categorized into “higher”, “medium” and “lower” tertiles within each community. Chi-square test was conducted to check adequacy of cells. Bivariate binary logistic regression was done for variables that fulfill chi-square test criteria to examine their association with the outcome variables. After checking multicollinearity among predictor variables in linear regression, variables with p-value less than 0.05 in bivariate analysis were entered into multivariable binary logistic regression using backward stepwise method.
Finally, variables with p-value less than 0.05 in multivariable analyses were considered as having statistically significant association with outcome variables. Adjusted odds ratio (AOR) with 95% CI was used to show the strength of association.
Ethical consideration
Ethical clearance was obtained from the Institutional Review Board (IRB) of College of Health Sciences, Jimma University. IRB has specifically approved this study and provided a letter of confirmation. Support letter was obtained from the department of Epidemiology and submitted to Somali Regional Health Bureau and Mieso Woreda administrative body, woreda health office, education office and respective schools. Written informed consent and verbal informed assent were obtained from parents/guardians and children respectively. Privacy of student was kept during anthropometric measurements. Confidentiality of collected information was also ensured.
Operational definitions
Community: A region, within which most people tend to follow the same patterns.
Pastoralist community: Community that practices herding as primary source of their family income.
Agro-pastoralist community: Community that practices both crops production and herding as primary source of their family income.
Woreda: It is the third level administrative district next to region/state and zone in Ethiopia.
Body Mass Index (BMI): It is weight in kilograms divided by the square of height in meters
Nutritional status: In this study, this term refers to either under nutrition (stunting or wasting/thinness) or not under nutrition.
Chronic malnutrition (stunting): It refers to height-for-age (HAZ) < -2 SD of median value of the NCHS/WHO international growth reference (WHO, 2009).
Acute malnutrition (wasting/thinness): It refers to BMI-for-age (BAZ) < -2 SD of the median value of the NCHS/WHO international growth reference (WHO, 2009).
Past episode of diarrhea: It refers to having three or more loose stools in 24 h in the past two weeks from the date of survey.
Food insecurity: It refers to having food insecurity index (produced from four food security questions) of 1 and above.
RESULTS
Socio-demographic and economic characteristics
A total of 655 (324 from pastoral and 331 from agro-pastoral community) school adolescents were included in the study making response rate of 94.1% (93.1 and 95.1% respectively). Thirty three adolescents were absent during data collection time and eight were excluded from analysis for incompleteness and inconsistency of the information.
“The majority of participants were male, both from the pastoral (54.0%) and the agro-pastoral (52.0%) commu-nities. The mean age was similar in both groups, 12.9 (SD = 1.9) and 12.7 (SD = 2.0) for participants of pastoral and agro-pastoral community respectively. The majority of participants were Somali (97.5% pastoral, 97.3% agro-pastoral) and Muslim (99.1% pastoral, 99.4% agro-pastoral). Almost half (49.4%) of pastoral and majority (55.0%) of agro-pastoral participants live within a family size of greater than five. The majority of households were male headed (98.1% pastoral, 95.8% agro-pastoral) and monogamous (86.4% pastoral, 92.1% agro-pastoral). The majority of both mothers (97.5% pastoral, 95.8% agro-pastoral) and fathers (88.0% pastoral, 81.3% agro-pastoral) were unable to read and write. Majorities (93.2% pastoral, 88.8% agro-pastoral) of the mothers were housewives and majorities (79.9% pastoral, 74.0% agro-pastoral) of the fathers were farmers. Sorghum is the main staple food (38.0% pastoral 44.7% agro-pastoral) for both communities (Table 1).


Magnitude of malnutrition and associated factors
Magnitude of malnutrition
Overall magnitude of stunting was 11.5% (95% CI: 9.1-13.9), with a lower magnitude in the pastoral community [8.3% (95% CI: 5.3-11.3)] than in the agro-pastoral community [14.5% (95% CI: 10.7-18.3)]. This difference was statistically significant. Overall magnitude of wasting/thinness was 22.9% (95% CI: 19.7-26.1), with higher magnitude in the pastoral community [26.2% (95% CI: 21.4-31.0), than in agro-pastoral community [19.6% (95% CI: 15.3-23.9)] though it was not statistically significant.
Factors associated with stunting
Stunting was significantly associated (p < 0.05) with type of community, sex of the adolescent, age of the adolescent, grade level, number of siblings, family size, source of drinking water, household wealth (tertiles), daily meal frequency, cough illness, and adolescent’s food security at bivariate level (Table 2).


The multivariable analysis was performed for variables showed statistically significant association with stunting at bivariate level. Type of community, sex of adolescent, age, family size, source of drinking water, household wealth (tertiles) and adolescent food insecurity were found independently associated with stunting (Table 3). From the table, adolescents of agro-pastoral community were 2.5 times more likely to be stunted than that of pastoral community [AOR: 2.52, 95%CI: (1.36,4.67)]. Female adolescents were 2.4 times more likely to be stunted than males [AOR: 2.36, 95%CI: (1.29,4.33)]. Adolescents in the age range of 15-18 were nearly 11 times more likely to be stunted than those of ages 10 to 14 [AOR: 10.85, 95%CI: (4.82, 24.41)]. Adolescents whose family’s size was greater than 5 were 2 times more likely to be stunted than adolescents whose family’s size was 5 or less [AOR: 1.92, 95%CI: (1.03, 3.57)]. Adolescents whose family’s source of drinking water was unprotected were 3.6 times more likely to be stunted than their counterpart [AOR: 3.59, 95%CI: (1.79, 7.20)]. Adolescents whose household wealth (tertile) was lower were 3.2 times more likely to be stunted than adolescents whose household wealth (tertile) was higher [AOR: 3.19, 95%CI: (1.47-6.94)]. Food insecured adolescents were 2.6 times more likely to be stunted than food secured adolescents [AOR: 2.57, 95%CI: (1.35, 4.88)].

Factors associated with wasting/thinness
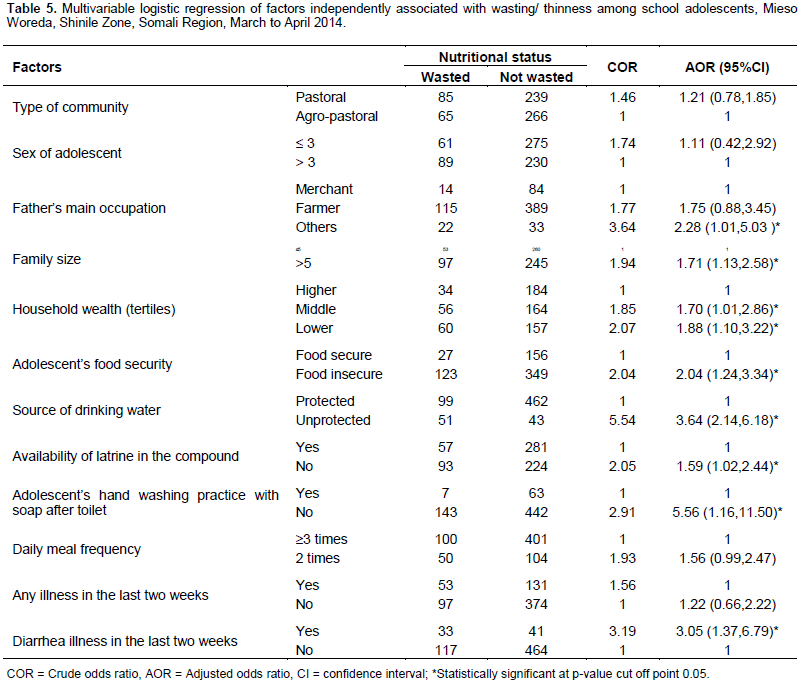
Wasting/thinness was significantly associated (p < 0.05) with type of community, number of siblings, family size, father’s main occupation, source of drinking water, availability of latrine in the compound, household wealth (tertiles), daily meal frequency, adolescent’s hand washing practice with soap after toilet, any illness in the last two weeks, diarrhea illness and adolescent’s food security (Table 4).


The multivariable analysis was performed for variables showed statistically significant association with wasting at bivariate level. Family size, the source of drinking water, availability of latrine in the compound, household wealth (tertiles), adolescent’s hand washing with soap after toilet, diarrhea illness in the last two weeks and adolescent food security were significantly associated with wasting (Table 5). From the table, children whose household family size was greater than 5 were 1.7 times more likely to be wasted than children whose household family size was 5 or less [(AOR: 1.71, 95%CI: (1.13, 2.58)]. Children whose family’s source of drinking water was unprotected were 3.6 times more likely to be wasted than their counterpart [AOR: 3.64, 95%CI: (2.14, 6.18)]. Adolescents whose family did not have latrine at home were 1.6 times higher at risk of being wasted than their counterparts [AOR: 1.59, 95%CI: (1.02, 2.44)]. Adolescents who did not have hand washing practice after toilet were 5.6 times more likely to be wasted than their counterparts [AOR: 5.56, 95%CI: (1.16,11.50)]. Adolescents who had diarrhea illness in the last two weeks were 3 times higher at risk of being wasted than who did not [AOR: 3.05, 95%CI: (1.37, 6.79)]. Adolescents whose household wealth (tertile) was lower and middle were 1.9 and 1.7 times more likely to be wasted respectively than adolescents whose household wealth (tertile) was higher [AOR: 1.88, 95%CI: (1.10, 3.22) and AOR: 1.70, 95%CI: (1.01, 2.86) respectively]. Food insecured adolescents were 2 times more likely to be wasted than food secured ones [AOR: 2.04, 95%CI: (1.24, 3.34)].
DISCUSSION
Comparative cross-sectional study was conducted from March 10 to April 11, 2014 at Mieso Woreda, Somali Region, to assess nutritional status of school adolescents and identify associated factors. The overall prevalence of stunting and wasting were 11.5 and 22.9%. The overall prevalence of stunting was lower than findings from different studies conducted in Northwest Ethiopia where stunting reports range from 15 to 30.7% (Amare et al., 2013, 2012; Mekonnen, 2013) and another study conducted in Ashanti region of Ghana which was 56.7% (Danquah et al., 2013). These differences could be due to the differences in their animal product consumption and food culture.
Prevalence of stunting was found to be higher (14.5%) in agro-pastoral than pastoral (8.3%) community while prevalence of thinness (wasting) was higher (26.2%) in pastoral than agro-pastoral (19.6%) community. These differences in nutritional status among pastoral and agro-pastoral communities were statistically significant and stunting remained significant even after adjusting to other factors. The likelihood of being stunted was 2.5 times more in agro-pastoral than pastoral community. There was scarcity of previous research conducted on children of similar age groups and communities to compare with present findings. However, this finding was in agreement with a study conducted on 6 to 36 months old children in Shinile zone of Somali region, Ethiopia (Save the Children, 2001; 2007). This could be due to the differences in main staple foods in the two communities. It could also be because of historical difference in stunting, that is, in the years past when these adolescents would have been affected, pastoral communities might have been wealthier than the agro-pastoral ones.
The overall prevalence of thinness (22.6%) was much higher than the reports of studies conducted in Adama town, Ethiopia (1.4%) (Belay et al., 2011), Gondar, Ethiopia (8.9%) (Amare et al., 2013), Kenya (4.5%) (Chesire et al., 2009) and Eastern Uganda (10.1%) (Acham et al., 2012). Since wasting reflects acute nutritional deficiency caused by inadequate food intake and/or infections (de Onis et al., 2007), this higher prevalence could be attributed to dry season (March to April) when pasture and water could be a problem and might have led to food shortage and infection during survey period.
Gender differential in the studies of nutritional status of children in less developed countries has frequently reported that boys were favored in that they were breast-fed longer, received better quality diet, child care time, health treatment and had better nutritional status (Shariff et al., 2000). In Ethiopia, in contrast to boys, girls often face a reduction in freedom and opportunities during puberty. These restrictions are frequently increased in rural parts of Ethiopia, where more than 85% of the girls live and where work burdens for adolescent girls are especially heavy. Puberty is also a time when girls’ bodies prepare for the nutritional demands of pregnancy and lactation required in later life (Berheto et al., 2015). The findings of this study showed significant difference of stunting between sex groups. Females adolescents were 2.4 times more likely to be stunted than males. However, this was not in agreement with reports of studies conducted in Morocco (Hioui et al., 2011) where females were less likely to be stunted than males (AOR: 0.41, CI: 0.94-0.03) and Uganda (Acham et al., 2012) which showed that girls were less vulnerable to malnutrition compared to boys (AOR: 0.96, CI: 0.56-1.66).
This study showed that stunting was significantly associated with age; 15 to 18 years old adolescents had higher odds to be stunted compared with 10 to 14 age groups. This was congruent to the reports of many studies which showed prevalence and severity of stunting has been found to increase with age, with older children diverging further from the reference medians for height until puberty (Acham et al., 2012; Al-Saffa, 2009; 2013; Awoyemi et al., 2012). This might be due to inadequate nutrient intake besides increased requirement during adolescents’ faster growth period or it could be that conditions are improving over time and that those older adolescents were more severely affected by malnutrition as preschoolers than the younger adolescents.
While it was expected that parental occupation appears to be one of the household factors that can influence the nutritional status of children, in this study, however, both parents’ occupational status did not show significant difference on their children’s nutritional status. This may be due to the fact that almost all mothers were housewives and majority of fathers were farmers.
Both stunting and wasting were more likely among larger families and this was in line with finding of studies done in Pakistan (Mian et al., 2002) and Jimma, Ethiopia (Assefa et al., 2013). Adolescents whose household’s wealth tertile were lower were 3.19 times more likely to be stunted than adolescents whose household’s wealth tertile was higher. This is in agreement with a study done in Jimma, Ethiopia (Assefa et al., 2013) where household income was positively associated with Height for Age z-score. Wasting was also more likely among adolescents of households with middle and lower wealth tertile than higher ones. This was in agreement with a study done in Jimma, Ethiopia (Assefa et al., 2013) where household income showed a positive association with BMI for Age z-score though not statistically significant.
This study revealed that food insecured adolescents were nearly 3 times more likely to be stunted than food secured adolescents. This may indicate the presence of chronic adolescent food insecurity in the study area since stunting shows chronic malnutrition. The finding was in line with study done in Jimma, Ethiopia (Central Statistical Agency [Ethiopia], 2014) where food insecurity is negatively associated with the linear growth of adolescents. Wasting is an indicator of acute malnutrition and it is usually the result of acute or short-term insufficient food intake often combined with frequent illness (de Onis et al., 2007). The result of this study supported the above idea as food insecured adolescents were 2 times more likely to be wasted than food secured adolescents.
The findings of this study support the fact that unfavorable environmental and personal conditions such as inadequate and unsafe water, poor sanitation, and poor personal hygiene can increase the probability of infectious diseases and, in turn, cause or aggravate malnutrition. In this study, stunting and wasting were significantly associated with the use of unprotected water source for drinking. Adolescents whose household did not have latrine at home were more likely to be wasted than their counter part. This was in consistent with the study done in Tigray, Northern Ethiopia (Mulugeta et al., 2009). Hand washing with soap after use of toilet also showed a significant association with wasting where adolescents who did not practice hand washing with soap after toilet were more likely to be wasted than those who did.
It is known that infection and under-nutrition are interrelated. The finding of this study showed that the likelihood of being wasted was 3 times higher among individuals who experienced diarrhea in the last two weeks than those who did not.
In general, since the findings of this study might have been affected by method of our data collection where household level information was obtained from adolescents, it should be used with caution.
CONCLUSION
This study revealed that the prevalence of stunting was significantly higher among adolescents of agro-pastoral community while the prevalence of wasting was higher among adolescents of pastoral community. Factors significantly association with stunting were type of community, sex of adolescent, age, family size, source of drinking water, household wealth tertile and adolescent food insecurity. Factors significantly association with wasting were family size, source of drinking water, latrine availability, after toilet hand washing practice, diarrhea illness in the last 2 weeks, household wealth tertile and adolescent food insecurity.
Recommendation
Based on our findings, scientific literature and current practice of the National Nutrition Program (NNP), the following nutrition specific and nutrition sensitive interventions are suggested for the NNP and other stakeholders to improve the nutrition condition of school children in the study area:
1. The Somali Regional State Health Bureau and Mieso Woreda Health Office should design interventions which targets adolescents’ malnutrition specific to pastoralist and agro-pastoral livelihood systems.
2. Mieso Woreda Education Office and Health Office should provide health education on personal hygiene integrating with regular educational activities in the school.
3. The Woreda Health Office should strengthen community education on family planning and environmental sanitation through health extension workers (HEWs).
4. The Woreda Water Service Office should strongly work to improve sources of drinking water.
5. Mieso Woreda Agriculture Office should strongly work and co-operate with other sectors and NGO’s to improve household economy and ensure adolescents’ food security through broadened microfinance institutions or other development and income generating activities.
6. Finally, other community based studies with different and stronger study designs, and improved source of information (e.g. parents) are encouraged to better understand adolescent malnutrition.
CONFLICTS OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENT
The authors would like to express their gratitude to Jimma University for financial support in conducting this study. They are also grateful to all bodies that gave permission and cooperation to conduct this study. Their special thanks go to participants of this study and their parents, without whose active participation, this study would not have been completed successfully. Last but not the least, their thanks go to data collectors, supervisors and others who contributed to the success of this study.
REFERENCES
|
Abera H (2016). Factors Influencing Children's Nutritional Status In Adami-Tulu Woreda (Thesis). AAU, 1996. |
|
|
Acham H, Kikafunda JK, Tylleskar T, Malde MK (2012). Nutritional and health status primary schoolchildren in rural Uganda. Afr. J. Food Agric. Nutr. Dev. 12 (2):5862-5880. |
|
|
Adugna E, Sileshi M (2013). Determinants of poverty in (agro-) pastoral societies of Southern Ethiopia. Livestock Res. Rural Dev. 25(20). |
|
|
Al-Saffa AJ (2009). Stunting among primary-school children: a sample from Baghdad, Iraq. East. Mediterr. Health J. Rev. 15(2):322-329. |
|
|
Amare B, Ali J, Moges B, Yismaw G, Belyhun Y, Gebretsadik S, Woldeyohannes D, Tafess K, Abate E, Endris M, Tegabu D, Mulu A, Ota F, Fantahun B, Kassu A (2013). Nutritional status, intestinal parasite infection and allergy among school children in Northwest Ethiopia. BMC Pediatr. 13:7. |
|
|
Amare B, Moges B, Fantahun B, Tafess K, Woldeyohannes D, Yismaw G, Ayane T, Yabutani T, Mulu A, Ota F, Kassu A (2012). Micronutrient levels and nutritional status of school children living in Northwest Ethiopia. Nutr. J. 11:108. |
|
|
Andrews T (2013). Reasons Why Students' Academic Performance May Be Impacted [WWW Document]. Artic. Artic. Dir. |
|
|
Assefa H, Belachew T, Negash L, Assefa H, Belachew T, Negash L (2013). Socioeconomic Factors Associated with Underweight and Stunting among Adolescents of Jimma Zone, South West Ethiopia: A Cross-Sectional Study. Int. Sch. Res. Not. 2013 (2013):e238546. |
|
|
Awoyemi TT, Odozi JC, Ogunniyi AA (2012). Environmental and Socioeconomic Correlates of Child Malnutrition in Iseyin Area of Oyo State, Nigeria. Food Publ. Health 2(4):92-98. |
|
|
Belay G, Reji P, Erko B, Legesse M, Belay M (2011). Intestinal parasitic infections and malnutrition amongst first-cycle primary schoolchildren in Adama, Ethiopia. Afr. J. Prim. Health Care Fam. Med. 3(1):5. |
|
|
Benson T (2005). An assessment of the causes of malnutrition in Ethiopia: a contribution to the formulation of a National Nutrition Strategy for Ethiopia [WWW Document]. Int. Food Policy Res. Inst. IFPRI. URL View (accessed 9.21.16). |
|
|
Berheto TM, Mikitie WK, Argaw A (2015). Urban-rural disparities in the nutritional status of school adolescent girls in the Mizan district, south-western Ethiopia. Rural Remote Health 15(3):3012. |
|
|
Black RE, Allen LH, Bhutta ZA, Caulfield LE, de Onis M, Ezzati M, Mathers C, Rivera J (2008). Maternal and child undernutrition: global and regional exposures and health consequences. Lancet 371(9608):243-260. |
|
|
Central Statistical Agency (CSA) [Ethiopia] (2014). Ethiopia Mini Demographic and Health Survey 2014. Addis Ababa, Ethiopia. |
|
|
Chesire E, Orago A, Oteba L, Echoka E (2009). Determinants of Under Nutrition among School Age Children in a Nairobi Peri-Urban Slum. East Afr. Med. J. 85(10). |
|
|
Cordeiro L, Lamstein S, Mahmud Z, Levinson FJ (2005). Adolescent Malnutrition in Developing Countries: A Close Look at the Problem and at Two National Experiences. United Nations SCN News. 31. Available at: |
|
|
Dambhare DG, Bharambe MS, Mehendale AM, Garg BS (2010). Nutritional Status and Morbidity among School going Adolescents in Wardha, a Peri-Urban area. Online J. Health Allied Sci. 9(2). |
|
|
Danquah AO, Amoah AN, Opare-Obisaw C (2013). Nutritional Status of Upper Primary School Pupils in a Rural Setting in Ghana. Int. J. Nutr. Food Sci. 2(6):320. |
|
|
de Onis M, Onyango AW, Borghi E, Siyam A, Nishida C, Siekmann J (2007). Development of a WHO growth reference for school-aged children and adolescents. Bull. World Health Organ. 85(9):660-667. |
|
|
Demographics of Ethiopia (2014). Wikipedia Free Encycl. Available at: |
|
|
Frongillo EA, Nanama S (2006). Development and validation of an experience-based measure of household food insecurity within and across seasons in northern Burkina Faso. J. Nutr. 136(5):1409S-1419S. |
|
|
Gebreyohannes Y, Shiferaw S, Demtsu B, Bugssa G (2014). Nutritional Status of Adolescents in Selected Government and Private Secondary Schools of Addis Ababa, Ethiopia. Int. J. Nutr. Food Sci. 3(6):504. |
|
|
Hall A, Kassa T, Demissie T, Degefie T, Lee S (2008). National survey of the health and nutrition of schoolchildren in Ethiopia. Trop. Med. Int. Health 13(12):1518-1526. |
|
|
Hioui ME, Azzaoui F-Z, Ahami AOT, Aboussaleh Y (2011). Nutritional Status and School Achievements in a Rural Area of Anti-Atlas, Morocco. Food Nutr. Sci. 2(8):878-883. |
|
|
Mekonnen H (2013). Malnutrition and its Correlates among Rural Primary School Children of Fogera District, Northwest Ethiopia. J. Nutr. Disord. Ther. 3(2). |
|
|
Mian RMA, Ali M, Ferroni PA, Underwood P (2002). The Nutritional Status of School-Aged Children in an Urban Squatter Settlement in Pakistan. Pak. J. Nutr. 1(3):121-123 |
|
|
Mulugeta A, Hagos F, Stoecker B, Kruseman G, Linderhof V, Abraha Z, Yohannes M, Samuel G (2009). Nutritional Status of Adolescent Girls from Rural Communities of Tigray, Northern Ethiopia. Ethiop. J. Health Dev. 23(1). |
|
|
Nunnally JC (1978). Psychometric theory. McGraw-Hill. 730. ISBN: 978-0-07-047465-9 |
|
|
Save the Children (2007). The causes of malnutrition in children under 3 in the Somali Region of Ethiopia related to household caring practices: Report on research findings from Somali Caring Practices research project in Shinile and Dambal districts of Shinile zone, Somali region, Ethiopia (Preliminary Report). Ethiopia. |
|
|
Save the Children (2001). Shinile Agropastoral Livelihood Zone (Sorghum, Cattle and Shoats). |
|
|
Shariff ZM, Bond J, Johson N (2000). Nutritional status of primary school children from low income households in kuala lumpur. Malays. J. Nutr. 6(1):17-32. |
|
|
The Partnership for Child Development (1999). Short stature and the age of enrolment in Primary School: studies in two African countries. Soc. Sci. Med. 48(5):675-682. |
|
|
The Partnership for Child Development (1997). Better health, nutrition and education for the school-aged child. Transact. Royal Soc. Trop. Med. Hyg. 91(1):1-2. |
|
|
Uauy R, Kain J, Mericq V, Rojas J, Corvalán C (2008). Nutrition, child growth, and chronic disease prevention. Ann. Med. 40(1):11-20. |
|
|
Walker SP, Chang SM, Powell CA, Simonoff E, Grantham-McGregor SM (2007). Early childhood stunting is associated with poor psychological functioning in late adolescence and effects are reduced by psychosocial stimulation. J. Nutr. 137(11):2464-2469. |
|
|
World Health Organization (WHO) (2009). Anthroplus for personal computers manual: Software for assessing growth of the world's children and adolescents. Department of Nutrition for Health and Development. Geneva. |
|
|
World Health Organization (WHO) (2006). Adolescent Nutrition: A Review of the Situation in Selected South-East Asian Countries. WHO Regional Office for South-East Asia, New Delhi. |
|
|
Wolde T, Amanu W, Mekonnin D, Yitayin F, Abu F, Dufera F, Birhanu T, Ejeta E (2014). Nu |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


