Full Length Research Paper

ABSTRACT
The Covid-19 pandemic, which originated from Wuhan, Hubei province, China, and quickly spread to the rest of the globe is caused by SARS-CoV-2 coronavirus. Preliminary data suggest a relationship between the BCG vaccine and the prevalence of Covid-19. The vaccine is used in the prevention of tuberculosis, a disease that is most prevalent in developing countries. To determine the potential protective role of Bacillus Calmette-Guérin (BCG) vaccination, this study investigated the occurrence of Covid-19 and the relationship between the spread of Covid-19 in countries that offer BCG vaccination and those that do not. To determine if some SARS-CoV-2 strains were more prevalent than others, the study also performed a phylogenetic analysis of the strains from the representative countries. To achieve the objectives, the study utilized publicly available data on population size, vaccination coverage and Covid-19 cases. The study revealed a significant negative trend between countries that offer the BCG vaccine to the general population and the reported cases of Covid-19. The study proposes future molecular and immunological analyses to determine the potential role of BCG vaccination in protection against Covid-19. This will determine if BCG vaccine has antiviral properties, with the possibility of recommending it for widespread use if supported by scientific data.
Key words: Bacillus Calmette-Guérin (BCG) vaccine, Covid-19, pandemic, phylogeographic analysis, vaccination.
INTRODUCTION
Over the last century, mankind has faced a few pandemics associated with the emergence of new microorganisms, the latest being the Covid-19 pandemic caused by severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) (Andersen et al., 2020). As of 30th April 2020, this virus was present in 212 countries and territories (Kang et al., 2020). Pandemics occur when novel microorganisms, usually viruses emerge as a result of mutations capable of coding for new potentiator biomolecules such as the spike glycoprotein by SARS-CoV-2 (Giovanetti et al., 2020). Consequently, the new machinery may enable the pathogen to jump between hosts, for instance from bats to pangolins and then from the intermediate host to humans (Andersen et al., 2020). Prompt data collection of the novel organisms is critical to understanding behavioral and infectious trends of these pathogens, and in disease mitigation by generating relevant antimicrobial agents (AMA) and vaccines. Efforts to generate effective AMA for novel organisms are challenged by limited understanding of the infectious agent, and hence monitoring basic trends becomes crucial. Following the spread of Covid-19, there have been mixed and unprecedented trends, and varying findings are still accumulating. Interestingly, for instance, countries that immensely practice BCG vaccination against tuberculosis (TB), caused by a bacterium (Mycobacterium tuberculosis) that has a deleterious respiratory effect (Curtis et al., 2020), have generally reported low infection and fatality rates (Miyasaka, 2020). This has led to suggestions that BCG vaccination could be slowing or helping in the protection against Covid-19 (Curtis et al., 2020). While this is likely, in part, a consequence of under-funded health systems, it is vital to investigate the observation. Previous studies have demonstrated that the BCG vaccine has non-specific beneficial effects (Curtis et al., 2020)(Uthayakumar et al., 2018), including increased protection from a variety of respiratory infectious diseases (Prentice et al., 2015). Some of these studies have revealed possible epigenetic changes that subsequently regulate cytokine production (Uthayakumar et al., 2018)(Arts et al., 2018). Coincidentally, most Covid-19 victims die due to unregulated cytokine production.
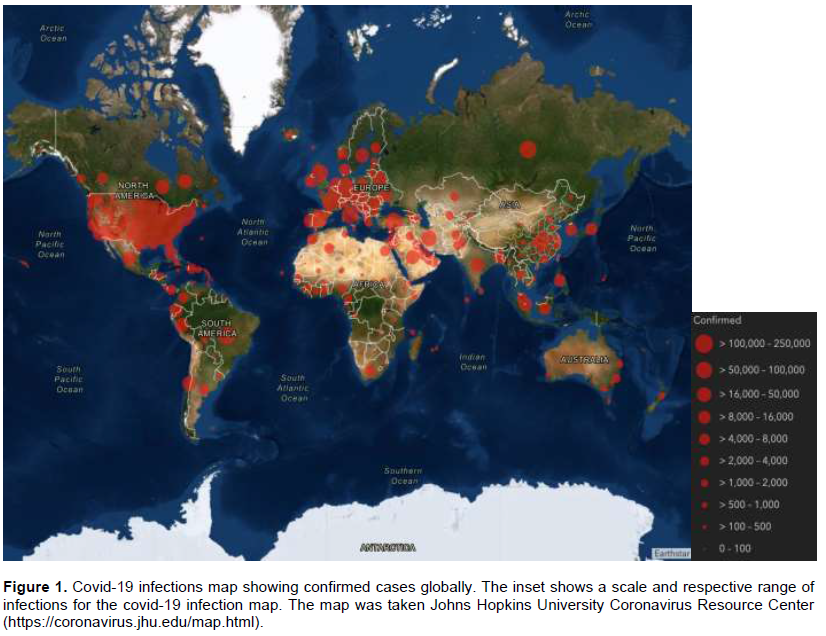
The study sought to find a correlation between BCG vaccination coverage and Covid-19 virus cases to determine if indeed that pattern arises. It has also been argued that because of variation in geographical positioning and comorbidities of the affected people (Guan et al., 2020), pandemics tend to cluster and generally impact different parts of the world to varying extents (https://coronavirus.jhu.edu/). As such, the novel Covid-19 virus is no exception with early data showing variation in distribution to different regions of the world (Ensheng et al., 2020). Herein, how the impact and the behavioral trend of the Novel Covid-19 virus might have been influenced by geographical positioning and immunization of the populace especially against TB was discussed. The current study aimed to evaluate the relationship between BCG vaccination and coronavirus isolated strains, thus the prevalence of Covid-19.
METHODOLOGY
BCG vaccination vs Covid-19 infected population
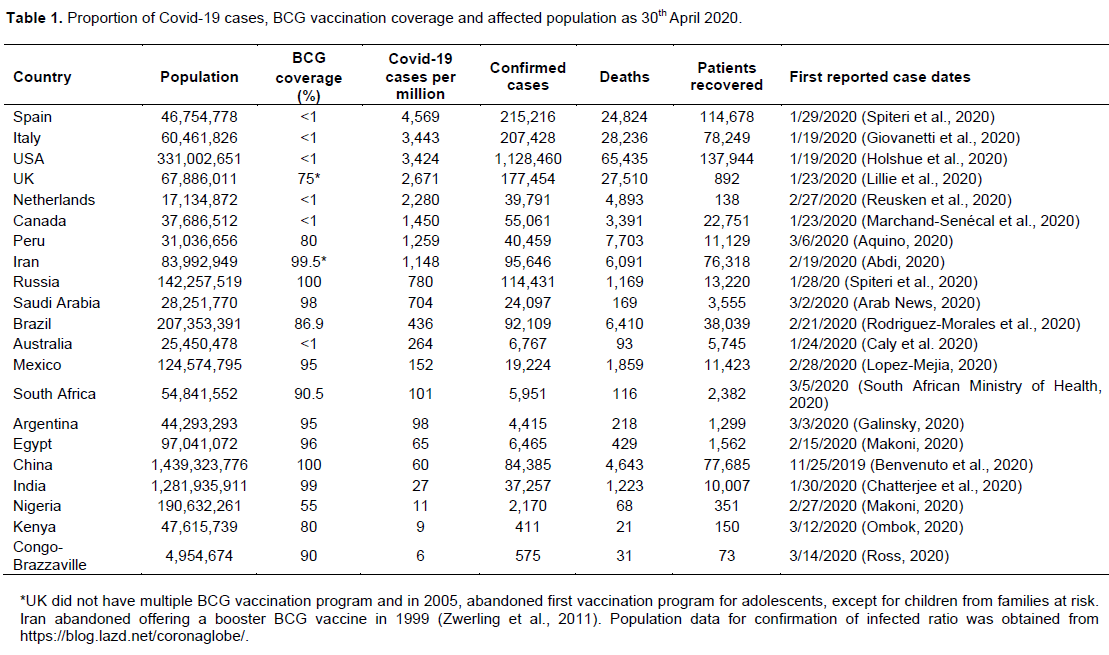
To establish if there was a correlation between Covid-19 infections and the BCG vaccination, representative countries across the globe were selected and data collected from publicly available data bases. The model countries were diversely selected to represent all the continents of the world as follows; North America (Canada, USA and Mexico), South America (Peru, Brazil and Argentina), Europe (Spain, Italy, United Kingdom and Netherlands), Africa (South Africa, Egypt, Nigeria, Kenya and Congo-Brazzaville), Asia (Russia, India, China, Saudi Arabia and Iran) and Australia. While data on Covid-19 infections was obtained from The Johns Hopkins Coronavirus Resource Center (https://coronavirus.jhu.edu/) and Google News (https://news.google.com/covid19), BCG vaccination data was acquired from BCG Atlas (http://www.bcgatlas.org/). Population data for confirmation of infected ratio was obtained from https://blog.lazd.net/coronaglobe/. Correlation analysis and graphing were performed using GraphPad Prism version 8 (https://www.graphpad.com/scientific-software/prism/).
Phylogeographic analysis
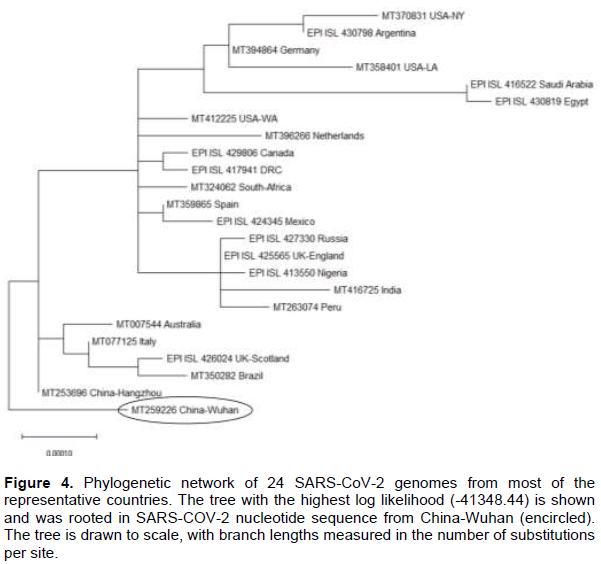
A phylogeographic analysis was performed to understand the historical and contemporary evolutionary changes of SARS-CoV-2 as it spread across the world relative to the origin, Wuhan China. The genomic data used was mined from publicly available genomic databases; Global Initiative on Sharing All Influenza Data (GISAID) (https://www.gisaid.org/ ) (Elbe and Buckland-Merrett, 2017) and https://www.ncbi.nlm.nih.gov/. The accession numbers for the two databases starts with EPI_ISL_ and MT, respectively. The nucleotide sequences utilized includes the following: MT412225 (USA-WA), MT370831 (USA-NY), MT358401 (USA-LA), EPI_ISL_429806 (Canada), EPI_ISL_424345 (Mexico), EPI_ISL_430798 (Argentina), MT350282 (Brazil), MT263074 (Peru), EPI_ISL_425565 (England), EPI_ISL_426024 (UK-Scotland), MT394864 (Germany), MT396266 (Netherlands), MT359865 (Spain), MT077125 (Italy), EPI_ISL_417941 (DRC), EPI_ISL_430819 (Egypt), EPI_ISL_413550 (Nigeria), MT324062 (South-Africa), EPI_ISL_427330 (Russia), EPI_ISL_416522 (Saudi-Arabia), MT416725 (India), MT259226 (China-Wuhan), MT253696 (China-Hangzhou) and MT007544 (Australia). In some countries such as USA and United Kingdom, several genomic data were selected for different geographical locations. In the USA for instance, genome from Washington (USA-WA), New York (USA-NY) and Louisiana (USA-LA) were identified and utilized, representing West Coast, East Coast and Southern states of USA, respectively.
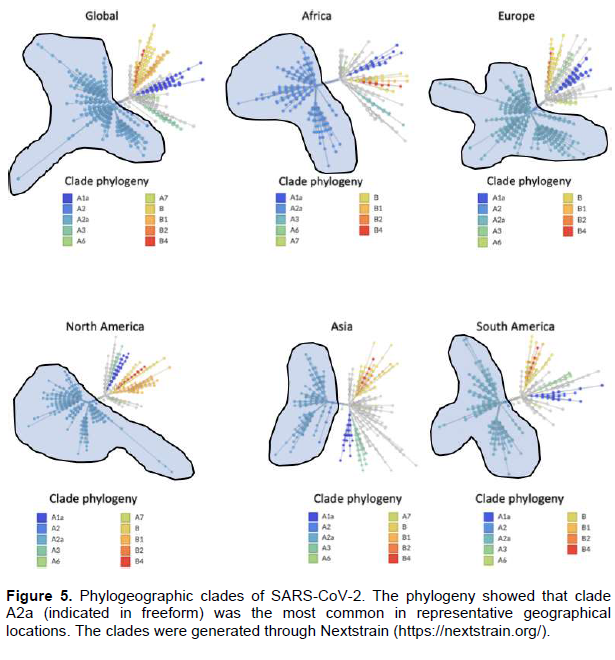
Phylogenetic analysis for clades of SARCoV-2 viruses from the pandemic was performed to determine the geographic spread of different clades. This was to help reveal if there was a more dominant clade, and its distribution across the globe. This was achieved using Nextstrain (https://nextstrain.org/).
RESULTS
BCG vaccination vs Covid-19 infected population
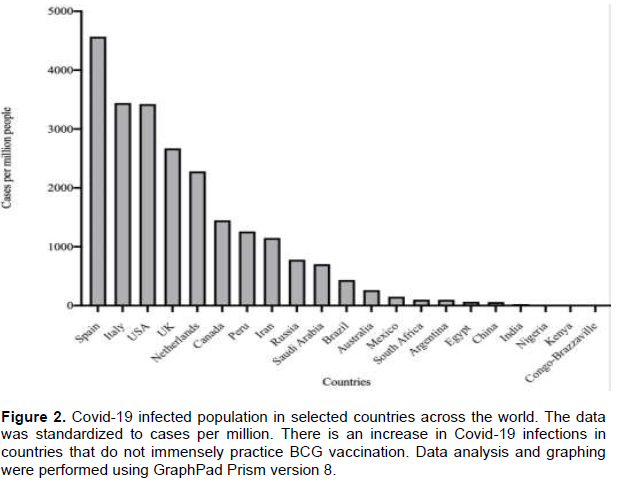
Data obtained from various databases were tabulated factoring in BCG vaccination coverage vs Covid-19 infected population. (Table 1) The details included population of the candidate countries, BCG vaccinations and Covid-19 infections. Further, the Covid-19 infections data was standardized to cases per million comparisons in representative countries and represented graphically (Table 1 and Figure 2). Interestingly, there were high cases of Covid-19 infections in countries that have less BCG vaccination as compared to countries that immensely use BCG vaccine.
Phylogeographic analysis
To further understand the genetic relationship and changes in the representative countries, a phylogeographic analysis was conducted.
Following alignment of the genomic data, a phylogeographic analysis was performed using the Tamura-Nei model on MEGA X (Kumar et al., 2018)as shown in Figure 4. The alignment sequences can be accessed via https://doi.org/10.6084/m9.figshare.12246302.v1. Evolutionary history was inferred by using the Maximum Likelihood method and the Tamura-Nei model. The tree with the highest log likelihood (-41348.44) is shown (Figure 4) and was rooted in SARS-CoV-2 nucleotide sequence from China-Wuhan (encircled). Initial tree(s) for the heuristic search were obtained automatically by applying Neighbor-Join and BioNJ algorithms to a matrix of pairwise distances estimated using the Tamura-Nei model, and then selecting the topology with superior log likelihood value. There were a total of 29911 positions in the final dataset. Phylogenetic analysis of SARCoV-2 viruses revealed that clade A2a was the most common both in all regions.
DISCUSSION
The Covid-19 pandemic has had a global impact (Figure 1) and a high fatality rate. By the end of April 2020, there were 3,303,296 confirmed cases and 235,290 deaths globally. Further emerging in silico predictions reflect even more infections and fatalities. However, European countries and the USA have reported the highest number of cases per one million people (Ensheng et al., 2020). India and the source of the pandemic, China, had lower cases per one million people compared to the USA, Italy, Spain, Netherlands, and UK, even though they are the most populated countries in the world (Table 1). African countries under study had hardly reported high cases of Covid-19 by the date this article was written (end of April, 2020). However, there was an initial fear that due to weaker healthcare systems, Chinese expatriates (about 2 million Chinese nationals live and work in Africa), and the associated increased travel between China and Africa for education, business and leisure, the infection rates could be higher (Kapata et al., 2020).
Coincidentally, countries with lower cases per million people had one thing in common: BCG vaccination (Figure 2). Interestingly, Iran, a country that abandoned offering a booster BCG vaccine in 1999 (Zwerling et al., 2011), registered high cases of Covid-19 (Figure 3). It is, however, hard to postulate the impact that may have had on Covid-19 incidences. The low number of cases in China could be due to the underlying effects of BCG vaccination and/or massive efforts by the government to contain the virus. Overall, countries with low TB incidences (mostly western countries) that do not administer the BCG vaccine to the general population had the highest Covid-19 cases per million people. Countries such as England stopped the BCG vaccination in 2005 (Fine, 2005) whereas Australia abandoned its program in the 1980s due to a reduction of tuberculosis incidences (Zwerling et al., 2011). India has an expansive BCG vaccination program (Zwerling et al., 2011). The country registered 27 cases per million people by the end of April 2020. Additionally, India’s reported first case was on 1/30/2020 (Table 1), and by April 5, 2020, the 1.3 billion people in India were put into lockdown. This precaution could have added to the containment of the virus spread. An even more interesting contrast was the low number of Covid-19 cases in the United States’ southern neighbor, Mexico; while Mexico reported 152 cases per million by the end of April 2020, the USA had 3,424 cases per million by the same date. A similar trend was seen between the USA and Argentina, a South American state with high BCG vaccination coverage.
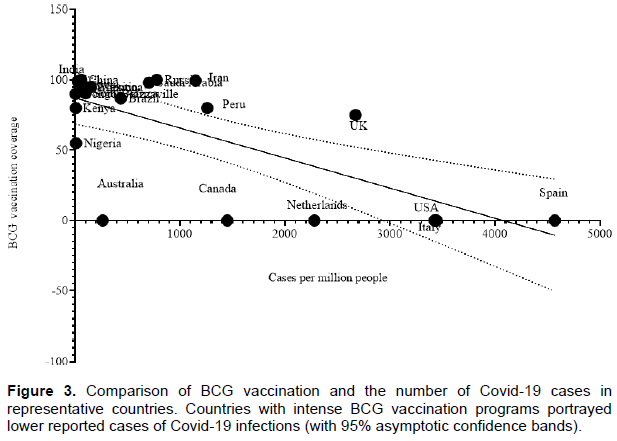
The BCG vaccination coverage had a negative correlation with reported Covid-19 cases (p<0.0001, R2=0.5707). Regression analysis revealed a strong association between low numbers of Covid-19 cases and BCG vaccination (mean value of 75.54%) (Figure 3). However, high numbers of Covid-19 cases cannot be explained by the lack of BCG vaccination alone. There are other risk factors such as comorbidity, age, and socio-economic factors including living conditions (Guan et al., 2020). Phylogenetic analysis using genomic data reveals that some countries that were highly impacted shared strains with the same ancestral nodes with those with less Covid-19 reported cases (Figure 4). This could mean shared strains alone may not determine cases, but BCG vaccine, which is shared among those reporting lower cases could be one factor, among other confounders. Further analysis revealed clade A2a was most common in Africa, North and South America, Europe, and Asia (Figure 5). Clade A2a was curiously the most common in New York City’s most affected areas of Manhattan, Brooklyn, Bronx and Westchester (Gonzalez-Reiche et al., 2020). The populations in New York City boroughs and its neighborhoods are considerably high. But these are not as poorly sanitized regions as slums in developing countries (Corburn and Hildebrand, 2015). Further, overcrowding (such as Kenya’s Kibera slums which has 30,000 persons per square mile) (Njuguna et al., 2013), poor infrastructure, and inadequate social amenities (Kamau and Njiru, 2018), would have led to a catastrophic situation. Further, looking at Saudi Arabia and Egypt (both with >95% BCG vaccine coverage) emphasizes the possible existence of other confounders besides BCG vaccination (Table 1). Countries which have an immense BCG vaccination practice continue to manifest low levels of Covid-19 spread. Although BCG vaccine induced changes have been found to correlate with protection against experimental viral infections (Arts et al., 2018), it is not precisely clear whether there is such protection against coronaviruses. An understanding of the effects of BCG vaccine (Ozdemir et al., 2020)and the mechanism of action will be key in making informed decisions based on evidence (Kumar and Meena, 2020). Phylogeographic analysis indicates initial occurrence in Wuhan, China, in November to December 2019, leading to transmission across the globe. Although clade A2a, isolated early during the pandemic from EU countries in February 2020 is the most common, evolution within this clade has been difficult to resolve (Gonzalez-Reiche et al., 2020). Consequently, it is assumed that other factors such as but not limited to weather, sanitation, comorbidity, the intensity of Covid-19 testing, different regional moments in the spreading of the pandemic, and continuous evolution of the virus are crucial confounders which warrant further individual and/or collective investigation(s).
CONCLUSION
If there is a correlation between BCG vaccination in representative countries across the world and the number of reported Covid-19 cases was assessed. The study revealed an inverse trend between countries that immensely offer BCG vaccination to the general population and reported cases of Covid-19. Whereas the study establishes a correlation, the contribution of other factors, including but not limited to test capabilities, demographics, and disease burden need to be investigated to further augment these findings. To elucidate direct antiviral effect of BCG vaccination, molecular analysis to determine the role of BCG vaccination and potential protection against coronaviruses should also be investigated. If BCG vaccine is found to have coronavirus protection benefits, the clinical need for a BCG vaccination may need to be re-evaluated in countries that do not predominantly administer it, particularly on vulnerable and easily exposed population groups such as, the elderly, healthcare workers, people with pre-existing conditions and those with other concerning comorbidities. Consequently, evidence of protection against viral respiratory infectious agents should underscore the need for developing countries to continue the administration of BCG vaccination promptly to offer continued beneficial effects on their populations.
ACKNOWLEDGMENTS
The authors gratefully appreciate the authors, originating and submitting laboratories of the sequences from GISAID’s EpiFlu™ and Nextstrain Databases. They also recognize Coronavirus Resource Center at Johns Hopkins University, Google’s COVID-19 news, and BCG atlas for the provision of data to the public. Lastly, they thank Philip Alabi (Brown University, Rhode Island), Rosemary Nyamboya (St George’s University Hospital, London, UK), Courtney Mariita (Troy Prep Charter Schools, New York), Michael Ochieng’ (Pontificia Universidad Comillas, Madrid, Spain) and Jessica Gilpin (Vanderbilt University, Tennessee) for their insights and feedback.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abdi M (2020). Coronavirus disease 2019 (COVID-19) outbreak in Iran: Actions and problems. Infection Control and Hospital Epidemiology pp. 1-2. |
|
|
Andersen KG, Rambaut A, Lipkin WI, Holmes EC, Garry RF (2020). The proximal origin of SARS-CoV-2. Nature Medicine. |
|
|
Aquino M (2020). Peru records first confirmed case of coronavirus, President Vizcarra says. |
|
|
Arab News (2020). Saudi Arabia announces first case of coronavirus. |
|
|
Arts RJ, Moorlag SJ, Novakovic B, Li Y, Wang S-Y, Oosting M, Kumar V, Xavier RJ, Wijmenga C, Joosten LA (2018). BCG vaccination protects against experimental viral infection in humans through the induction of cytokines associated with trained immunity. Cell Host and Microbe 23:89-100. |
|
|
Benvenuto D, Giovanetti M, Salemi M, Prosperi M, De Flora C, Alcantara LC, Angeletti S, Ciccozzi M (2020). The global spread of 2019-nCoV: A molecular evolutionary analysis. Pathogens and Global Health 114:64-67. |
|
|
Caly L, Druce J, Roberts J, Bond K, Tran T, Kostecki R, Yoga Y, Naughton W, Taiaroa G, Seemann T (2020). Isolation and rapid sharing of the 2019 novel coronavirus (SARSâ€CoVâ€2) from the first patient diagnosed with COVIDâ€19 in Australia. Medical Journal of Australia. |
|
|
Chatterjee K, Chatterjee K, Kumar A, Shankar S (2020). Healthcare impact of COVID-19 epidemic in India: A stochastic mathematical model. Medical Journal, Armed Forces India |
|
|
Corburn J, Hildebrand C (2015). Slum Sanitation and the Social Determinants of Women's Health in Nairobi, Kenya. Journal of Environmental and Public Health 209505-209505. |
|
|
Curtis N, Sparrow A, Ghebreyesus TA, Netea MG (2020). Considering BCG vaccination to reduce the impact of COVID-19. The Lancet. |
|
|
Ensheng D, Hongru D, Lauren G (2020). An interactive web-based dashboard to track COVID-19 in real time. The Lancet Infectious Diseases. |
|
|
Galinsky P (2020). Confirmaron el primer caso de coronavirus en Argentina: trasladaron el paciente a otra cliÌnica |
|
|
Giovanetti M, Benvenuto D, Angeletti S, Ciccozzi M (2020). The first two cases of 2019-nCoV in Italy: Where they come from? Journal of Medical Virology 92:518-521. |
|
|
Gonzalez-Reiche AS, Hernandez MM, Sullivan M, Ciferri B, Alshammary H, Obla A, Fabre S, Kleiner G, Polanco J, Khan Z, Alburquerque B, Guchte A, Dutta J, Francoeur N, Melo BS, Oussenko I, Deikus G, Soto J, Sridhar SH, Wang Y-C, Twyman K, Kasarskis A, Altman DR, Smith M, Sebra R, Aberg J, Krammer F, Garcia-Sarstre A, Luksza M, Patel G, Paniz-Mondolfi A, Gitman M, Sordillo EM, Simon V, Bakel H (2020). Introductions and early spread of SARS-CoV-2 in the New York City area. |
|
|
Guan W, Liang W, Zhao Y, Liang H, Chen Z, Li Y, Liu X, Chen R, Tang C, Wang T (2020). Comorbidity and its impact on 1590 patients with Covid-19 in China: A Nationwide Analysis. European Respiratory Journal 55(5). |
|
|
Holshue ML, DeBolt C, Lindquist S, Lofy KH, Wiesman J, Bruce H, Spitters C, Ericson K, Wilkerson S, Tural A, Diaz G, Cohn A, Fox L, Patel A, Gerber SI, Kim L, Tong S, Lu X, Lindstrom S, Pallansch MA, Weldon WC, Biggs HM, Uyeki TM, Pillai SK, Washington State 2019-nCoV Case Investigation Team (2020). First Case of 2019 Novel Coronavirus in the United States. The New England Journal of Medicine 382:929-936. |
|
|
Kang S, Peng W, Zhu Y, Lu S, Zhou M, Lin W, Wu W, Huang S, Jiang L, Luo X, Deng M (2020). Recent progress in understanding 2019 novel coronavirus (SARS-CoV-2) associated with human respiratory disease: detection, mechanisms and treatment. International Journal of Antimicrobial Agents 55(5):105950. |
|
|
Kapata N, Ihekweazu C, Ntoumi F, Raji T, Chanda-Kapata P, Mwaba P, Mukonka V, Bates M, Tembo J, Corman V, Mfinanga S, Asogun D, Elton L, Arruda LB, Thomason MJ, Mboera L, Yavlinsky A, Haider N, Simons D, Hollmann L, Lule SA, Veas F, Abdel Hamid MM, Dar O, Edwards S, Vairo F, McHugh TD, Drosten C, Kock R, Ippolito G and Zumla A (2020). Is Africa prepared for tackling the COVID-19 (SARS-CoV-2) epidemic. Lessons from past outbreaks, ongoing pan-African public health efforts, and implications for the future. International Journal of Infectious Diseases 93:233-236. |
|
|
Kumar J, Meena J (2020). Demystifying BCG Vaccine and COVID-19 Relationship. Indian Pediatrics. |
|
|
Kumar S, Stecher G, Li M, Knyaz C, Tamura K (2018). MEGA X: molecular evolutionary genetics analysis across computing platforms. Molecular Biology and Evolution 35(6):1547-1549. |
|
|
Lillie PJ, Samson A, Li A, Adams K, Capstick R, Barlow GD, Easom N, Hamilton E, Moss PJ, Evans A, Ivan M, Phe Incident Team, Taha Y, Duncan CJA, Schmid ML, The Airborne Hcid Network (2020). Novel coronavirus disease (Covid-19): The first two patients in the UK with person to person transmission. The Journal of Infection 80(5):578-606. |
|
|
Lopez-Mejia M (2020). Mexico confirms first coronavirus cases in two men returned from Italy. |
|
|
Makoni M (2020). Keeping COVID-19 at bay in Africa. The Lancet Respiratory Medicine. |
|
|
Marchand-Senécal X, Kozak R, Mubareka S, Salt N, Gubbay JB, Eshaghi A, Allen V, Li Y, Bastien N, Gilmour M, Ozaldin O, Leis JA (2020). Diagnosis and Management of First Case of COVID-19 in Canada: Lessons applied from SARS. Clinical infectious diseases: An official publication of the Infectious Diseases Society of America, ciaa227. |
|
|
Miyasaka M (2020). Is BCG vaccination causally related to reduced COVID-19 mortality? EMBO Molecular Medicine 12(6):12661. |
|
|
Njuguna HN, Cosmas L, Williamson J, Nyachieo D, Olack B, Ochieng JB, Wamola N, Oundo JO, Feikin DR, Mintz ED, Breiman RF (2013). Use of population-based surveillance to define the high incidence of shigellosis in an urban slum in Nairobi, Kenya [published correction appears in PLoS One. 2014;9(8):e105031]. PLoS ONE. 2013;8(3):e58437. |
|
|
Ombok E (2020). Kenya Reports First Case of Coronavirus. |
|
|
Ozdemir C, Kucuksezer UC, Tamay ZU (2020). Is BCG vaccination effecting the spread and severity of COVIDâ€19? Allergy. |
|
|
Prentice S, Webb EL, Dockrell HM, Kaleebu P, Elliott AM, Cose S (2015). Investigating the non-specific effects of BCG vaccination on the innate immune system in Ugandan neonates: Study protocol for a randomised controlled trial. Trials 16(1):149. |
|
|
Reusken CB, Buiting A, Bleeker-Rovers C, Diederen B, Hooiveld M, Friesema I, Koopmans M, Kortbeek T, Lutgens SP, Meijer A, Murk J-L, Overdevest I, Trienekens T, Timen A, Bijllaardt W, Dissel J, Gageldonk-Lafeber A, Vegt D, Wever PC, Hoek W, Kluytmans J (2020). Rapid assessment of regional SARS-CoV-2 community transmission through a convenience sample of healthcare workers, the Netherlands, March 2020. Eurosurveillance 25(12):2000334 |
|
|
Rodriguez-Morales AJ, Gallego V, Escalera-Antezana JP, Méndez CA, Zambrano LI, Franco-Paredes C, Suárez JA, Rodriguez-Enciso HD, Balbin-Ramon GJ, Savio-Larriera E, Risquez A, Cimerman S (2020). COVID-19 in Latin America: The implications of the first confirmed case in Brazil. Travel Medicine and Infectious Disease 101613-101613. |
|
|
Ross A (2020). Congo Republic confirms first coronavirus case -government. |
|
|
South African Ministry of Health (2020). Minister Zweli Mkhize reports first case of Coronavirus Covid-19. |
|
|
Spiteri G, Fielding J, Diercke M, Campese C, Enouf V, Gaymard A, Bella A, Sognamiglio P, Sierra Moros MJ, Riutort AN, Demina YV, Mahieu R, Broas M, Bengnér M, Buda S, Schilling J, Filleul L, Lepoutre A, Saura C, Mailles A, Levy-Bruhl D, Coignard B, Bernard-Stoecklin S, Behillil S, Werf S, Valette M, Lina B, Riccardo F, Nicastri E, Casas I, Larrauri A, Salom Castell M, Pozo F, Maksyutov RA, Martin C, Van Ranst M, Bossuyt N, Siira L, Sane J, Tegmark-Wisell K, Palmérus M, Broberg EK, Beauté J, Jorgensen P, Bundle N, Pereyaslov D, Adlhoch C, Pukkila J, Pebody R, Olsen S, Ciancio BC (2020). First cases of coronavirus disease 2019 (COVID-19) in the WHO European Region, 24 January to 21 February 2020. Eurosurveillance 25(9):2000178. |
|
|
Uthayakumar D, Paris S, Chapat L, Freyburger L, Poulet H, Luca K (2018). Non-specific Effects of Vaccines Illustrated Through the BCG Example: From Observations to Demonstrations. Frontiers in Immunology 9:2869-2869. |
|
|
Zwerling A, Behr MA, Verma A, Brewer TF, Menzies D, Pai M (2011). The BCG World Atlas: A database of global BCG vaccination policies and practices. PLoS Medicine 8(3):e1001012. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


