Full Length Research Paper

ABSTRACT
In this review, we addressed risk factors for the spread of COVID-19 in the perspective of developing countries, and necessary measures to be undertaken to minimize or control its consequential crisis. Databases such as MEDLINE, PubMed, EMBASE, CINAHL, Web of Science, Scopus and websites of WHO, CDC, and ECDC were searched for relevant information and a narrative analysis approach was followed. As of April 10, 2020, there were a total of 1,674,967 cases and 101,483 deaths from COVID-19 in 210 countries, territories and two international conveyances around the world. During the same period Ethiopia has reported 64 confirmed cases, three deaths and four recoveries. Despite efforts being made to reduce most destinations, international flight especially to and from COVID-19 most hit countries were potential source of virus to the country. Large family size, low prevalence of the soap-based hand-washing practice, poor living conditions and social gatherings are among the main possible risk factors. On the other hand, limited health systems’ capacity in terms of trained workforce, medical supplies, diagnostic facilities, and intensive care units are possible challenges to control the pandemic. The current meagre testing capacity in the country that focuses only on suspected symptomatic cases while the virus is reportedly transmits from asymptomatic cases may result in a catastrophe due to its hidden spread in the community. For countries with weak economies, focusing their efforts on preventive measures is the best and yet cost-effective strategy. Some preventive efforts should focus on community health education about physical distancing, hand hygiene, use of personal protective equipment, self-isolation and quarantine in the context of the local situation. It is crucial to enhance self-reporting and community-based family level care to the symptomatic cases and their contacts. Additional care needs to be in place during burial ceremonies of the unavoidably dead bodies to prevent further contamination. The socio-psychological consequences of COVID-19 need to be given appropriate consideration to avoid unnecessary discrimination, stigma and social destructions. Finally, coordinated efforts to increase contact tracing, isolation, testing and treating needs to be strengthened through national and international collaborations.
Key words: Coronavirus Disease, COVID-19, SARS-COV-2, Corona risks, developing
Abbreviation: CDC, Center for Disease Control; COVID-19, Corona Virus Disease of 2019; EPHI, Ethiopian Public Health Institute; ECDC, European Center for Disease Control; IQR, Interquartile Range; MERS, Middle East Respiratory Syndrome; USA, United States of America; WHO, World Health Organization.
INTRODUCTION
On 31 December 2019, global attention was taken by a cluster of pneumonia-like respiratory cases of unknow origin in China (Huang et al., 2020), which was later identified as a novel beta coronavirus, and so provisionally named as 2019-nCOVCOVID-19 (Duarte et al., 2020; Zhu et al., 2020). The outbreak has spread swiftly in many countries, with the number of new cases infected and death from the infection increasing on an everyday basis (Habibzadeh and Stoneman, 2020). The high contagious potential of the virus via multiple routes and unspecified intermediate hosts seemed to pose a challenge in controlling efforts (ECDC, 2020; WHO, 2020a). On the 30th World Health Organization (WHO) Emergency Committee Meeting, it was agreed that the outbreak has met the criteria for a public health emergency of international concern (WHO, 2020b) and on March 11, 2020, it was officially designated COVID-19 and as a pandemic. In most cases, the risk of death from COVID-19 is linked to being increased in elderly and individuals with underlying chronic infection like diabetes, respiratory infection and diseases, cardiovascular and other disorders (Worldometer, 2020). As of April 10, 2020, in Africa, there were 11,774 confirmed cases and 610 deaths in 52 countries (Comoros and Lesotho don’t have reported cases of COVID-19) (Worldometer, 2020).
The trend so far indicates that most cases and deaths were being reported in developed countries where there is better access stronger health care and infection control systems in comparison to the developing countries (Worldometer, 2020). One can imagine what a crisis would be if the current infection would have happened and transmitted in settings where infection control systems are weak and public awareness is poor. Therefore, it is timely and urgent to highlight the possible challenges and looming crisis from the perspective of developing countries like Ethiopia. Here, we addressed the existing possibilities and scenarios that potentially can facilitate a rapid spread of the coronavirus in the country, given that the country has a population of over 112 million, the second highly populated country in Africa (World Population Review, 2020).
In general, there is a huge public health concern with the fact that most factors for transmission are readily available; the health systems to contain COVID-19 cases are weak and even not fully accessible to all citizens as that of developed countries. There are social practices that can facilitate transmission of the coronavirus disease such as greeting by handshaking, cheek kissing and hugging across the society, and it is also common to share the dining plates, water glasses, beds and bed sheets among large-sized families. Developing countries like Ethiopia, are in an economic, financial and resource constraints to control the already existing life-threatening infectious diseases. Moreover, the current modalities of case detection, diagnosis and quarantine for coronavirus are resource demanding, which adds direct and indirect economic burden to the countries with weak economic background. In addition to this, the call for political commitment, which has already been observed for the control of prevalent infectious diseases like TB, HIV, and malaria, adds massive public health concerns and thus attention in this regard is needed for the current pandemic (Ren, 2019; Vitoria et al., 2009). Therefore, there is a need to address the issue of COVID-19 in the light of mobilizing all the concerning bodies to maximize their efforts towards preventing, which comparably is the best and cheapest strategy. Thus, the current narrative synthesis aims to provide an overview on the major risk factors for the spread of COVID-19 in Ethiopia, along with the opportunities that exist to mitigate these risks.
METHODS
Information sources and searching strategies
Such as MEDLINE, PubMed, EMBASE, CINAHL, Web of Science and Scopus were searched to capture recent and updated evidences: In addition, unpublished and grey literatures were retrieved from Google Scholar, WHO, CDC, ECDC and other relevant sources. We used MeSH and search terms to construct a search string for each database including terms like ‘coronavirus disease’ or ‘COVID-2019’, and ‘risk factors’. For example, the following search strategy was used on PubMed: ("COVID-19"[All Fields] OR "COVID-2019"[All Fields] OR "severe acute respiratory syndrome coronavirus 2"[Supplementary Concept] OR "severe acute respiratory syndrome coronavirus 2"[All Fields] OR "2019-nCoV"[All Fields] OR "SARS-CoV-2"[All Fields] OR "2019nCoV"[All Fields] OR (("Wuhan"[All Fields] AND ("coronavirus"[MeSH Terms] OR "coronavirus"[All Fields])) AND (2019/12[PDAT] OR 2020[PDAT]))) AND ("risk factors"[MeSH Terms] OR ("risk"[All Fields] AND "factors"[All Fields]) OR "risk factors"[All Fields]) AND "humans"[MeSH Terms] AND ("humans"[MeSH Terms] AND English [lang]).
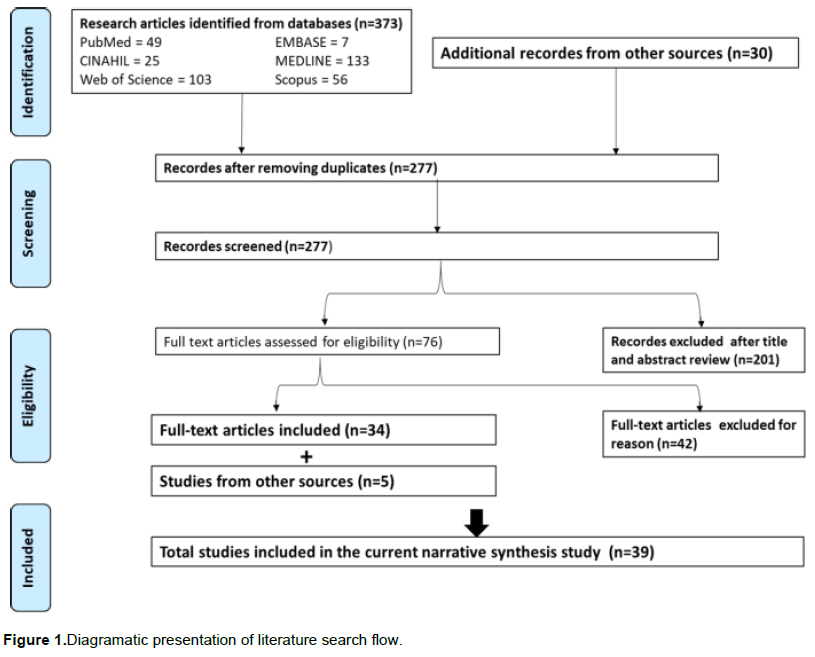
After the searches, duplicate studies were removed, and further screened for inclusion using the title and abstract. Included studies were then reviewed in full text by two authors. Any differences in evaluation of studies were resolved by consensus including the third author. Media briefings from Ethiopian public health institute and the ministry of health were used as a major source for local data. The PRISMA flow diagram (Stewart et al., 2015) is shown in Figure 1.
Review question: What are the possible risk factors for COVID-19 spread in Ethiopia with respect to current global and local conditions and what possible recommendations can be forward to halt the spread of coronavirus disease?
The synthesis: We followed narrative approach to synthesize the evidences from the included studies and other data sources.
RESULTS AND DISCUSSION
Current epidemiological status of COVID-19
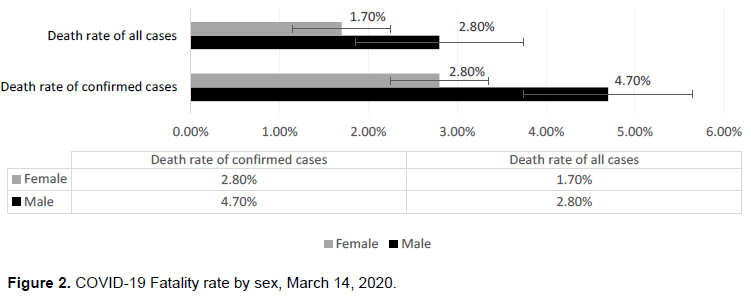
The median age of laboratory-confirmed cases was 51 years (range two days to100 years; IQR 39-63 years) with the majority of cases (77.8%) aged between 30–69 years and 51.1% are males. The virus was transmitting via droplets and fomites during close unprotected contact between an infector and an infectee, with the majority of cases occurring within the households (78-85%) or families (WHO, 2020). In Europe, Spain, Italy, Germany and France were reported case numbers above 120,000 whereas USA is approaching half a million. In Italy and USA, the death toll jumped to 18,000 while in Spain and France 15,970 and 13,197 deaths respectively, were recorded until April 10, 2020 (Worldometer, 2020). The death rate was higher in males (4.7%) than females (2.8%) (Figure 2).
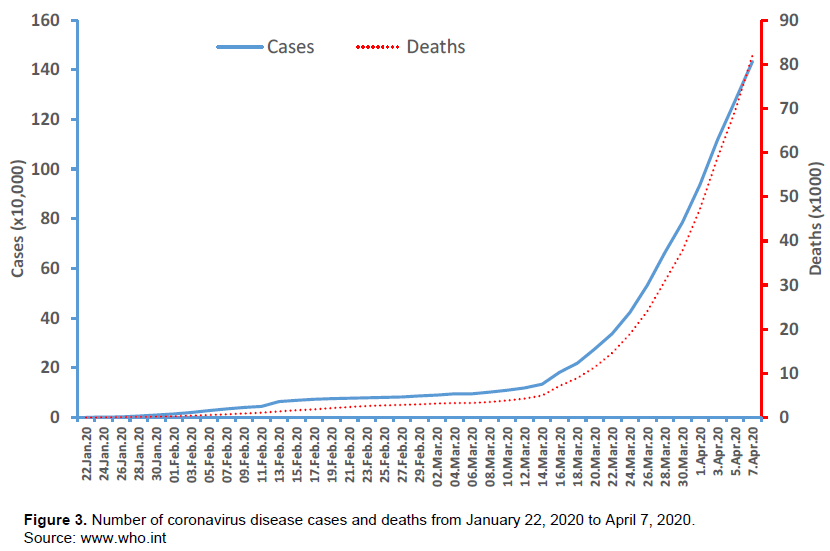
As of April 10, 2020, the coronavirus outbreak had sickened more than 1,674,967 people, and at least 101,483 people had died, and 371,866 were recovered in 210 countries and territories and two international conveyances around the world. Globally, there are a total of 215 cases per million and 13 death per million population were registered (Worldometer, 2020) (Figure 3).
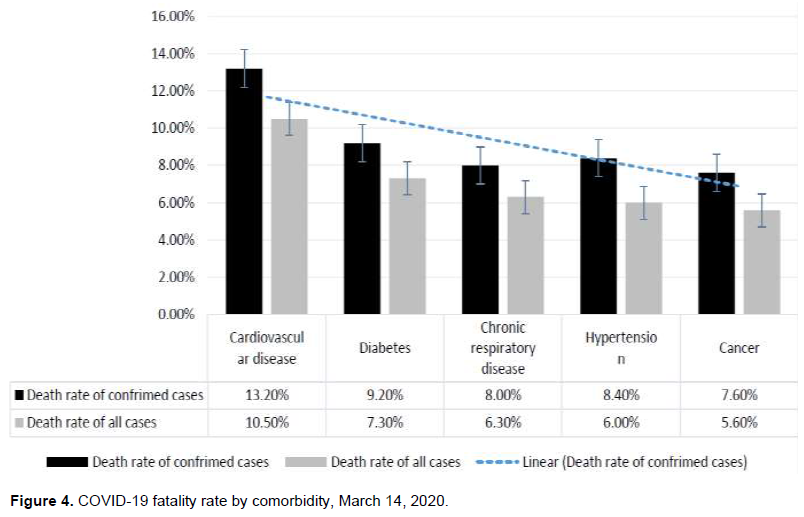
It was majorly affecting individuals with cardiovascular diseases (10.5%), diabetes (7.3%), chronic respiratory diseases (6.3%), hypertension (6.0%) and cancer (5.6%). Its mortality rate was low (0.9%) among no pre-existing diseases and none among children below 9 years (Worldometer, 2020) (Figure 4).
Knowledge gaps on COVID-19 pandemic
Regarding susceptibility, the WHO report showed that no known pre-existing immunity or factors that can increase the coronavirus susceptibility of human infection (WHO, 2020). Researchers need to answer the level of individual susceptibility in comparison to the pre-existing health problems like malaria, tuberculosis, HIV/AIDS, and other viral and poverty-related diseases as well as exposure to their treatment and vaccines with particular attention to sub-Saharan Africa. And if the recent hypothesis regarding the antimalarial drugs (Chloroquine and hydro-chloroquine) and BCG vaccines are effective against COVID-19, its severity may not be as worse as in Western countries.
The routes of transmission are also not explicitly understood. There were preliminary reports indicating the potential airborne spread of COVID-19 that is awaiting further investigation for confirmation (Yuan Liu et al., 2020). A potential fecal-oral transmission from fecal shedding of the virus has been demonstrated from some patients, and the viable virus has been identified in a limited number of reported cases (WHO, 2020).This poses additional risk for the developing countries where feco-orally transmitting infections are prevalent due to poor hygiene and inadequate infection control practices (UNICEF, 2018).
With the current virus being novel at infecting human being, multitudes of possible infection risk prevention measures need to be considered. In a clinical settings, the virus could remain in or on medical equipment such as stethoscope, sphygmomanometer, and other instruments and this may contribute as a common conduit of transmission. The uptake of cashless transactions in Ethiopia is lower compared to developed countries and thus a large proportion of commercial activities are by involving handling of coins or money notes. Notably, the coronavirus could remain on money notes for days, and people could get infected while buying and selling (The Telegraph, 2020).
Variability in the incubation period has also been reported in different countries and thus 14 days should not be considered as an absolute length of incubation for COVID-19. COVID-19 cases with an incubation period of 27 days (Reuters, 2020), 19 days (Bai et al., 2020), and 24 days (Guan et al., 2020) were reported in China. A report from Germany showed that individuals could shade the virus before the clinical manifestation of the disease (Sebastian et al., 2020), and they had the potential to infect others. Therefore, tracing and testing all contacts of the index case are important. However, tracing all contacts is not an easy task in a country with low technological advancement; so every community members should be cooperative and maintain their own health by reporting any contacts with confirmed or suspected cases.
Mounting of the host immunity following post-infection is becoming vague after 14% of recovered coronavirus patients tested positive with an unknown degree of infectivity (Li et al., 2020). Therefore, isolating and careful follow-up of all previously treated and recovered cases for several days after discharging is needed as non-negligible number of false negative cases were reported by RT-PCR (Yafang et al., 2020). In this case, there might be a need to revise the existing treatment guidelines for the COVID-19 that states patients can be considered recovered and released from the hospital when their throat or nose swabs show up contrary in two consecutive tests, with a CT scan indicating no lung lesions, and when they have no apparent symptoms such as fever (Li et al., 2020).
COVID-19 risk factors in Ethiopia and similar settings
Family structure and environmental characteristics
In China, human-to-human transmission of the SARS-COV-2 virus is mainly occurring within families (78-85%), with the estimated secondary attack rate in households' ranging from three to 10% (WHO, 2020). According to the 2016 estimate, in Ethiopia, the average household size was 4.6 persons, with nearly half of them under the age of 15 years (47%), while 4% were above age 65 (Chen et al., 2019). In the country, there is an extended family structure such that married sons and daughters may continue living together with their families. In some cases, unmarried aunts, uncles, cousins, and even close family friends could continue to live together with the nuclear family (Ethiopian Public Health Institute, 2020). Therefore, in such cases, if the infection starts to happen within large-sized families the condition most likely turns to be complex and complicates the control efforts.
One of the recommended hygiene measures is regular hand washing with soap and water, which is believed to play a critical role in preventing the COVID-19 transmission. Unfortunately, the prevalence of hand washing with soap and water in Ethiopia was as low as 28% in urban households and 7% in rural households (Central Statistical Agency, 2017). This could mainly be due to about 35% of the population having no access to improved water source and only 6.3% of households have access to improved sanitation. This is already proved to lead to around 60 to 80% of communicable diseases that attributed to limited access to safe water and inadequate sanitation and hygiene services (UNICEF, 2018). Given the large family size with inadequate hygiene and sanitation practices, the authors believe that coronavirus related messaging should mainly target families and therefore, effective strategies and models designed to outreach efficiently at the family level would help reducing the spread of disease.
Social structures and socioeconomic phenomenon
Ethiopia can be considered as a high-risk country based on the societal structure and socioeconomic basis. There are strong social ties and attachments with frequent physical interactions that have been developed for centuries as a beneficial means of integrity, which are now considered to be risk factors for COVID-19 transmission. In urban cities such as Addis Ababa, institutions that provide public services are inadequate, such that crowding is common in hotels, cafes, restaurants, public transportation, market places, hospitals, and other social institutions. These may find it difficult to maintain physical/social distancing as means of infection prevention strategy, thus may facilitate swift spread of coronavirus disease.
Social groups with less decisive power in most developing countries like Ethiopia such as children, women/girls, homeless and poor households can be especially vulnerable for violence, risk of abuse and associated psychosocial distress if specific measures could not be considered (The Alliance for Child Protection in Humanitarian Action, 2020). Handling these groups in a caring way possible will contribute a lot to the containment of the virus.
The lockdown and stay-at-home motto, which seems working in most developed countries, might not be effective, and even may worsening the case in economically poor settings. The rural society with limited or no shopping centers whose food supplies are based on weekly markets, will substantially be affected unless strategies to reach out to them is designed ahead. There are individuals whose survival is based on daily labor. If it will be an unavoidable option to apply, there must be a consideration of basic needs like food and shelter for the homeless. Also, there must be coordinated efforts including every member of the society, charity organizations, government and the international community to sustain the life of these groups if the worst scenario happens. If these people are overlooked, successful control of COVID-19 will be elusive at national and international levels.
Transportation, screening and current speed of coronavirus spread
Ethiopia put strict screening at points of entry to airports, and suspected cases are being recorded. Controversially, unlike other airlines, until recently Ethiopian Airlines did not cancel all flights to countries profoundly affected by the coronavirus. Ethiopian Ministry of Health (MOH) and Ethiopian Public Health Institute (EPHI) reported that they are jointly working 24-hrs in Bole International Airport and other major gates to the country (Ethiopian Public Health Institute, 2020) mainly focusing on assessing contact history and clinical evaluation of suspect cases. The authors believe continued flights from Ethiopian Airlines as well as other airlines to Ethiopia will make the population pay unnecessary cost regarding to COVID-19 even though the flights have paramount importance for the country from different angles.
Although the majority of laboratory-confirmed cases in China and elsewhere in the world were clinically symptomatic; there were asymptomatic cases that were confirmed positive by a real-time reverse-transcription–polymerase-chain-reaction (RT-PCR)(Philip, 2004). This case was similar to the diagnosis of asymptomatic cases by RT-PCR assays of throat swabs and sputum in Germany who were shedding potentially infectious virus without fever but only minor signs of infection (Sebastian et al., 2020).Therefore, evaluation and testing of passengers for body temperature alone may not be sufficient to detect COVID-19. As such, a robust public health surveillance system coupled with rapid and reliable diagnostic testing and quarantine are suggested to control COVID-19 and other diseases that has no vaccine or therapy (Anthony and Perlman, 2015).
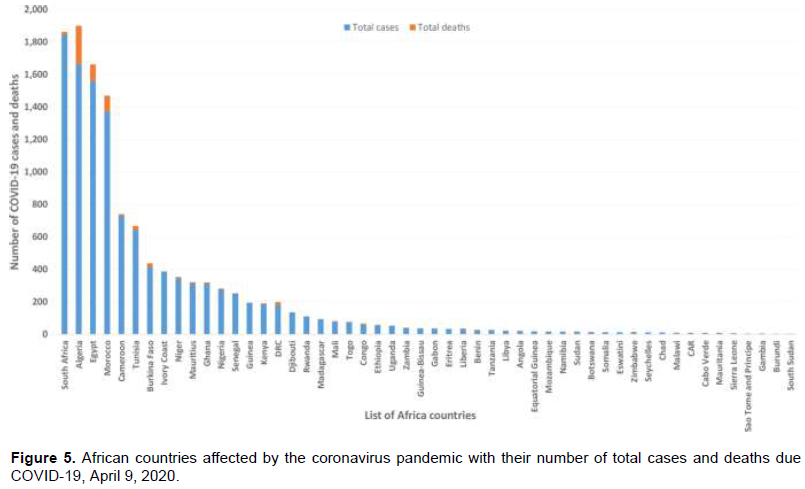
Importantly, strict follow-up around all borders are required as movement around these area may introduce the virus to the pastoralist and agrarian rural communities so that the virus can spread so fast without detection and will be difficult to control. Furthermore, Africa with a population over 1.2 billion, is highlighted by the WHO as an area where the coronavirus could rapidly take off mainly due to a lack of adequate health systems with a priority alerting list of 13 countries, including Ethiopia (Tom, 2020) (Figure 5 and S1 Table).
Shortage of adequate equipment and risk of health care workers
A simultaneous shortage of personal protective equipment (PPE) is endangering health workers worldwide, which was mainly caused by rising demand, panic buying, hoarding, and misuse for unintended purpose (WHO, 2020). There is already existing critical gap in Africa, and WHO has completed its first phase of distribution to 24 countries with confirmed cases, their neighbors, and major regional transport hubs (WHO Regional Office for Africa, 2020).
The shortage of PPE at least to the health workers poses risk of getting infection for themselves and spreading it to other patients, colleagues and their families. Without secured supply chains of PPE, the risk to healthcare workers around the world is real, and the statement by the WHO ''We can't stop COVID-19 without protecting health workers first," is valid to be addressed (WHO, 2020). Therefore, industries and governments need to act quickly to boost supply, ease import/export restrictions, and put measures to stop speculations and hoarding.
Lack of equipment and limited trained professionals to diagnose and detect the virus, may lead to inconspicuous hidden spread of infection in the country. A preemptive approach to make available high-level skilled and trained health personnel at the national level would be a timely intervention. The current relatively coronavirus free window, if used wisely to plan and implement public health interventions, will be an excellent opportunity to manage the pandemic in countries with limited resource such as Ethiopia and other similar settings.
Proper communication channel, preventive behaviors, and panic managements
Communication with the public during health emergency events is an essential function of government agencies.
Successful communication helps to control the emergency by aiding the public to rapidly adjust behaviors and perceptions of risk, while unsuccessful policies can promote community outrage, and impede the progress of threat mitigation (Maxwell, 2003). Trusted and verifiable sources of information are critical in communication with the public. For example, during the Middle East Respiratory Syndrome (MERS) outbreak crisis in South Korea, people were using online news, interpersonal networks, and social media to acquire MERS-related information more frequently than the information from public health officials, which was regarded as untrustworthy (Kyungeun and Young Min, 2018). The consequence of such sources may lead the public to inappropriate risk perception and disrupts preventive measures. A clear consistent and timely information from government or public health officials with the most essential and necessary regulations saves from unnecessary panics (Yoo and Park, 2016). Moreover, information on social media may not be accurate enough, and the diffusion of misinformation via these media can have a direct impact on the spread of the disease as it easily influences public behavior to a larger extent (Robert, 2020). In the case of Europe, the ECDC in its communication and data protection section for COVID-19 preparedness made transparent discussion and clear communication lines to allow rapid information to all staffs, patients/visitors, media and the general public (ECDC, 2020). The current efforts of mainstream media are great and should continue updating the public from trusted sources like Ministry of Health, EPHI, WHO, CDC and other credible information sources.
In order to develop preventive behaviors and control of panics at different levels, effective communication is highly important. The Ethiopian MOH, EPHI, and other government stakeholders need to plan jointly, and disseminate real-time information to the public through reliable and traditional media outlets.
Willingness of the people to expose themselves
Individuals with signs and symptoms or suspected to have coronavirus disease may hide in the community because of the fear of stigma, discrimination, and social and economic isolation (Jefferson, March 2, 2020). In such cases, individuals need to be encouraged to expose themselves when they have sign and symptoms or spot of contact with known or suspected cases. This can only be achieved if the community reaches a conscious consensus about the extent of risk and impending crisis of the infection at individual, family, community, national and international levels. Community need to be supportive and act at its maximum humanitarian level possible to avoid early fear, stigma and negative attitudes that can result in disruption of the socio-economic and mental status of the survivors.
In different rural parts of Ethiopia, especially among older people, there is a widespread belief that illnesses are being caused by supernatural forces, not by micro-organisms, and tend to use culturally prescribed treatment rather than seeking modern health care (Hodes and Teferedegne, 1996; Workneh et al., 2018). This type of belief can have negative effect on acceptance and implementation of preventive measures such as social/physical distancing, hand hygiene and voluntariness to be quarantined and following up of the treatment. Therefore, health education that targets rural and older people designed in the local context should be provided.
Behaviors that act as either barriers or promoters for self-isolation, self-reporting and status disclosure need to be studied and implemented based on expertise recommendation.
Responsibility of regional governments
In Ethiopia, a national committee consisting of six ministries has been set up to monitor COVID-19 pandemic. From the reports of EPHI, major preparedness suspected cases screening are taking place mainly in Addis Ababa, the capital city activities such as health personnel training and (Ethiopian Public Health Institute and Ministry of Health, 2020). Given the heterogeneous nature of regional health offices in terms of capacity and resources to manage and control such a serious pandemic in the country, efforts to harmonize response capabilities across the country are critically sought. Based on the Italy experience, incorrect management of a single case could lead to an overwhelmed health system crisis and loss of several lives unnecessarily (Fabrizio, 2020). Therefore, the regional governments need to be alert in designing strategies pertinent to their settings in addition to the national regulations. Based on the existing evidences on socioeconomic status of households, food security for those who cannot survive without aid need to be given attention.
International community
In the era of globalization where the world is being considered as a single home for all humankind and global population as a single family, countries with better economy need to stand in solidarity with developing countries. Countries with strong pharmaceutical companies and industries need to take this opportunity to establish a strong bond partnership to provide wide range of humanitarian support for those that needs it most.
Capacity building of health care workers in terms of case detection, diagnosis, and case management can save more lives. Provision of testing supplies either by donation or affordable prices need to be put at top priority. Everyone across the globe should consider COVID-19 as a common enemy of all humankind and stand together to fight against it with all capacity.
LIMITATIONS OF THE STUDY
This study has some limitations such as dynamically changing nature of number of corona virus infected cases hindering us from providing solid quantitative data on the number of cases and deaths from COVID-19. Some of the recommendations are already being applied in some developing countries but not in others, and this does not underestimate the importance of the current study. Nevertheless, the recommendations and concerns contained in this review are valid, contribute to the ongoing efforts, and can potentially save more lives.
CONCLUSION AND RECOMMENDATIONS
Corona virus is spreading globally at a swift pace and there are few reported cases in Ethiopia. In such a pandemic situation, for countries with a weak economy such as Ethiopia and most of the African countries, preventive efforts should be considered as the best and cost-effective measures. Failure to prevent will lead to a more costly approach of controlling and case management, which is resource-intensive and unaffordable. Therefore, the following risk mitigation approaches are strongly recommended: banning of close contacts like handshaking and kissing for greetings that are common practices in Ethiopia and other countries. Community health education focusing on the causes, prevention and the possible consequences should be cascaded as fast as possible to the lowest administrative units of every household. The WHO standard recommendations on infection prevention strategies like regular hand washing, covering mouth and nose while coughing and sneezing, and cooking meat, eggs and other animal products need to be adhered strictly. Future interventions should target family units to break infection chains and prevent further spread of the virus. The socio-psychological consequences of COVID-19 need to be given appropriate consideration to avoid unnecessary discrimination, stigma and deterioration of social health. International community need to stand with developing countries and build capacity of case detection, diagnosis and case management. The need to increase testing capacity should be emphasized as without it all the efforts may not bring satisfactory outcomes.
ETHICS APPROVAL AND CONSENT TO PARTICIPATE
The authors of primary study are acknowledged
CONFLICT OF INTERESTS
The authors declare that there is no conflict of interest
REFERENCES
|
Anthony RF, Perlman S (2015). Coronaviruses: An Overview of Their Replication and Pathogenesis Methods in Molecular Biology, 1282. |
|
|
Bai Y, Yao L, Wei T, Tian F, Jin DY, Chen L, Wang M (2020). Presumed Asymptomatic Carrier Transmission of COVID-19. JAMA. |
|
|
Central Statistical Agency (2017). Ethiopian Demographic and Health Survey, 2016. |
|
|
Chen F, Knutson TP, Rossow S, Saif LJ, Marthaler DG (2019). Decline of transmissible gastroenteritis virus and its complex evolutionary relationship with porcine respiratory coronavirus in the United States. Science Reports 9(1):3953. |
|
|
Duarte R, Furtado I, Sousa L, CFA C (2020). The 2019 Novel Coronavirus (2019-nCoV): Novel Virus, Old Challenges.Acta Medica Portuguesa |
|
|
ECDC (2020). Case definition for EU surveillance of COVID-19. . |
|
|
ECDC (February 2020). European Centre for Disease Prevention and Control. Check list for hospitals preparing for the reception and care of coronavirus 2019 (COVID-19) patients. ECDC: Stockholm; 2020. . |
|
|
Ethiopian Public Health Institute. (March 2020). The Ethiopian Public Health Institute's (EPHI) Press Statement on Coronavirus Disease (COVID-19) |
|
|
Ethiopian Public Health Institute, & Ministry of Health. (March 03, 2020). Urgent Press Release on Coronavirus Disease in Ethiopia. |
|
|
Fabrizio C (2020). Covid-19: preparedness, decentralization, and the hunt for patient zero. Lessons from the Italian outbreak. BMJ, 368. |
|
|
Guan WJ, Ni ZY, Hu Y, Liang WH, Ou CQ, He JX, Zhong NS (2020). Clinical characteristics of 2019 novel coronavirus disease in China. med R xiv, 2020.2002.2006.20020974. |
|
|
Habibzadeh P, Stoneman EK (2020). The Novel Coronavirus: A Bird's Eye View. International Journal of Occup Environiment Medicine 11(2):65-71. |
|
|
Hodes RM, Teferedegne B (1996). Traditional beliefs and disease practices of Ethiopian Jews. Israel Journal of Medical Sciences, 32(7):561-567. |
|
|
Huang C, Wang Y, Li X, Ren L, Zhao J, Hu Y, Gu X (2020). Clinical features of patients infected with 2019 novel coronavirus in Wuhan, China. Lancet. |
|
|
Jefferson T (March 2, 2020). Covid 19-many questions, no clear answers. BMJ Opinion. |
|
|
Kyungeun J, Young MB (2018). When Information fromPublic Health Officials is Untrustworthy: The Use of Online News, Interpersonal |
|
|
Networks,and Social Media during the MERS Outbreak in South Korea, Health Communication. |
|
|
Li Liuqian, Huang Shulun, Wei, H. (Feb 26, 2020 ). 14% of recovered coronavirus patients in China's Guangdong tested positive again: CAIXIN GLOBAL. |
|
|
Maxwell TA (2003). The public needs to know: emergencies, government organizations, and public information policies. Government Information Quarterly20(3):233-258. |
|
|
Philip S (2004). Diseases ofpoverty and the10/90 Gap. |
|
|
Ren M (2019). Greater political commitment needed to eliminate malaria. Infectious Distance Poverty 8(1):28. |
|
|
Reuters. (Feb. 22, 2020). Coronavirus incubation could be as long as 27 days, Chinese provincial government says. |
|
|
Robert P (Feb 21, 2020). The covid-19 outbreak has shown we need strategies to manage panic during epidemics. thebmjopinion. |
|
|
Sebastian Hoehl, Annemarie Berger, Marhild Kortenbusch, Jindrich Cinatl, Denisa Bojkova, Holger Rabenau. (February 18, 2020). Evidence of SARS-CoV-2 Infection in Returning Travelers from Wuhan, China: Correspondence. New England Journal of Medicine |
|
|
Stewart LA, Clarke M, Rovers M, Riley RD, Simmonds M, Stewart G, JF T (2015). Preferred reporting items for systematic review and meta-analyses of individual participant data: the PRISMA-IPD statement. . JAMA 313(16):1657-1665. |
|
|
The Alliance for Child Protection in Humanitarian Action. (2020). Technical Note: Protection of Children during the Coronavirus Pandemic (v.1). |
|
|
The Telegraph (2020). Cash could be spreading the coronavirus, warns the World Health Organization. |
|
|
Tom Flanagan. (March 5, 2020). The 13 countries that could be the next coronavirus centres. |
|
|
UNICEF (2018). Water, sanitation and hygiene (WASH). |
|
|
Vitoria M, Granich R, Gilks CF, Gunneberg C, Hosseini M, Were W, De Cock KM (2009). The global fight against HIV/AIDS, tuberculosis, and malaria: current status and future perspectives. American Journal Clinical Pathology 131(6):844-848. |
|
|
WHO. (2020a). WHO: Novel Coronavirus - China Geneva 2020 |
|
|
WHO Regional Office for Africa. (March 13, 2020). More than 15 countries in Africa report COVID-19 cases. |
|
|
WHO (2020b). Statement on the second meeting of the International Health Regulations (2005) Emergency Committee regarding the outbreak of novel coronavirus (2019-nCoV). |
|
|
WHO (2020, March 03, 2020). Shortage of personal protective equipment endangering health workers worldwide. |
|
|
WHO (February 2020). Report of the WHO-China Joint Mission on Coronavirus Disease 2019 (COVID-19). |
|
|
Workneh T, Emirie G, Kaba M, Mekonnen Y, Kloos H (2018). Perceptions of health and illness among the Konso people of southwestern Ethiopia: persistence and change. Journal of Ethnobiology and Ethnomedicine14(1):18. |
|
|
World Population Review (2020). Total Population by Country 2020. |
|
|
Worldometer. (April 10, 2020, March 07, 2020). COVID-19 Coronavirus Outbreak. . |
|
|
Yafang Li, Lin Yao, Jiawei Li, Lei Chen, Yiyan Song, Zhifang Cai, Chunhua Yang (2020). Stability Issues of RT-PCR Testing of SARS-CoV-2 for Hospitalized Patients Clinically Diagnosed with COVID-19 |
|
|
Yoo W, Choi DH, Park K (2016). The effects of SNS communication: How expressing and receiving information predict MERS-preventive behavioral intentions in South Korea. Computers in Human Behavior 62:34-43. |
|
|
Yuan Liu, Zhi Ning, Yu Chen, Ming Guo, Yingle Liu, Nirmal Kumar Gali, Qingyan Fu KL (2020). Aerodynamic Characteristics and RNA Concentration of SARS-CoV-2 Aerosol in Wuhan Hospitals during COVID-19 Outbreak. bioRxiv, Preprint. |
|
|
Zhu N, Zhang D, Wang W, Li X, Yang B, Song J, RL (2020). A Novel Coronavirus from Patients with Pneumonia in China. New England Journal of Medicine, 2019. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


