Full Length Research Paper

ABSTRACT
Demographic and health surveys provide household level data on population dynamics and health-related issues. Findings from a well characterized community can be used by relevant stakeholders to plan appropriate and acceptable health interventions for the benefit of the citizens. This project aimed to characterize Ijede community in Ikorodu LGA of Lagos State, Nigeria in preparation for a more appropriate Demographic and Health Surveillance System (DHSS) in the community. The study carried out a cross-sectional study in Ijede community in Lagos State. Buildings and structures in the community were mapped, a census of the community taken, socio-demographic details of household heads obtained, availability of water, sanitation and hygiene, and other facilities assessed. Descriptive statistics were used for analysis of data. The population of the community was 8,208 persons in 2,171 households with a male-female ratio of 1:1. About half of the populations (47.4%) were aged less than 20 years. Majority of household heads were males (72.4%), aged 40-59 years (43.0%), retail traders (25.8%), and married (68.8%). Multifarious tenement buildings constituted majority of buildings. The major source of water supply is the borehole (59.6%) and the water is not purified in 60.0% of cases. The flush toilet constitutes majority of toilet facilities but 15.4% are still uncovered pit latrines. Ijede community has been characterized, with a population of 8,208 and key demographic parameters obtained, thus providing required baseline for the establishment of a DHSS in this community.
Key words: Mapping, demographic, surveillance, health, population.
INTRODUCTION
Demographic and health surveys systematically collect information, which not only provides knowledge about the prevailing health characteristics or indices in a particular community but also serves as a veritable resource for effective health planning. Government and other stakeholders utilize survey results to plan and monitor health interventions in any community, irrespective of size, taking into cognizance the demographic changes that occur over time (Fisher and Way, 1988). The United States Agency for International Development (USAID), working in collaboration with various partners has helped over 90 countries including Nigeria carry out about 320 nationally representative demographic and health surveys since 1984 when the programme was first established (Fisher & Way, 1988). Many developing countries in sub-Saharan Africa and Asia have been beneficiaries of the programme (El-Zanaty and Way, 2000; ICF Macro, 2009; Corsi et al., 2012; Gambia Bureau of Statistics, 2014).
National demographic and health surveys (NDHS) usually collect relevant data on the health and social indices of people and their health systems. Information collected includes data on sexual and reproductive health indices, child health indices, and data on prevalent health conditions in the community such as malaria and HIV/AIDS (Aday and Cornelius, 1990; ICF, 2016). The first NDHS in Nigeria took place in 1990 (Federal Office of Statistics and IRD/Macro International Inc., 1992), and there have been periodic repeats and sentinel surveys over the years. The last NDHS in Nigeria took place in 2018 (National Population Commission (NPC) [Nigeria] and ICF, 2019). These have however been national surveys with appropriate sampling techniques to make the findings nationally representative. The information provided by these surveys has informed health policy decisions and implementation by the relevant ministries and agencies of the government of the federation.
However, the wholesale application of the findings from a national DHS may not accurately represent the health indices and needs of different communities of a particular country, especially one as large and ethnically and geographically diverse as Nigeria with heterogeneous communities in the different geo-political zones and states. Community based surveys are therefore necessary for health planning to suit communities with similar sociodemographic and health indicators. Even developed countries such as the United States of America that have conducted nationally representative surveys for decades have recognized the need for community surveys (Plescia et al., 2001).
Geographic variation can be a marker of health disparities. It is therefore important to physically characterize a community with the use of such technology as the Geographic Information System (GIS). This enables health disparities in a country to be put in a spatial context (Khan & Skinner, 2011). The mapping of a community entails detailing the features of the community such as population characteristics, leadership structure, housing, presence/absence, and types of social and infrastructural amenities like water supply, toilet facilities, health services (orthodox and traditional), schools, markets (including supermarkets and malls), recreational facilities including spaces for sporting activities, and communication networks. Community mapping helps to identify issues for targeted intervention such as the need for infrastructural development (Khan and Skinner, 2011). Community mapping can be carried out by members of the community themselves, with help from governmental or non-governmental agencies, or it can be initiated by an organization for a particular purpose to ensure comprehensive immunization coverage, or for a field trial for biomedical research purposes. No matter what the purpose of the mapping is the active participation of the members of that community is essential to not only ensure the success of the mapping process, but also the success of any eventual intervention planned.
Community mapping helps to identify community needs for health and social interventions which can then be prioritized and tackled as resources become available. A well-mapped community can also serve as a veritable resource in biomedical research on interventions that can serve, not only the community but also the country, as well as have a global impact. The importance of a Demographic and Health Surveillance System (DHSS), a system that provides the platform for assessing a wide range of health-systems, social and economic interventions in a geographically defined population under continuous monitoring, with timely updates and collection of data on all births, deaths, and migrations (all closely associated with research activities) cannot be over-emphasized. As a reliable structure, DHSS is useful as a viable response mechanism for developing countries, in the absence of effective health and population data, to stimulate rational health planning and meaningful health programs for the people. It will also help policy-makers to set health priorities and allocate resources more efficiently, and serve as a platform for the testing of health interventions, to provide feedback on programs’ effectiveness, and inform future policy development.
Rationale
Well mapped and characterized demographic and health surveillance sites in different parts of Nigeria will be invaluable in the actualization of the Nigerian Institute of Medical Research’s mandate of “health research for national development”. They will provide the platform for the identification of the social and health needs of the communities, which may be extrapolated to the state where the communities exist and even the country as a whole. This will help to inform policy so that targeted interventions, which will be more effective and acceptable to the community, can be developed, prioritized, and implemented as funds become available. Such communities can also serve as sites for the purposes of clinical and field trials.
Researchers in NIMR have worked extensively at the National Malaria Sentinel site in Ijede Community in Ikorodu Local Government Area (LGA) of Lagos State for about 20 years now and are quite familiar with the community and its leadership structure. It was therefore decided to establish the first DHSS site for Nigerian Institute of Medical Research (NIMR) at Ijede, Ikorodu LGA, Lagos, Nigeria. The project map and characterizes Ijede community in Ikorodu LGA of Lagos State, Nigeria in preparation for a DHSS in the community.
MATERIALS AND METHODS
Study design
This was a cross-sectional household survey.
Project site
Ijede is a community in Ikorodu (LGA) in Lagos State, southwestern Nigeria. The state is unique, being the smallest in terms of landmass, the commercial hub, and former administrative capital, and the most densely populated with a projected population density of around 6,871 residents per square kilometer in 2020 (World Population Review, 2020). There are 20 Local Government Areas (LGAs) and 37 Local Council Development Areas (LCDAs) in the state.
Ijede is a semi-urban coastal community of Lagos State, located at latitude 6°34’ 0” North, and longitude 3° 36’ 0” East (Maplandia.com, 2016). It is one of the five Local Council Development Areas (LCDA) of Ikorodu Local Government Area. It is on an average elevation of 42 m above sea level, and is bounded on the south by the Lagos lagoon, west by Bayeku, and east and north by Gberigbe. It is situated about 36 km northeast of metropolitan Lagos and the central business district on the Lagos and Victoria Islands can be accessed from Ijede across the lagoon by ferry in 25-30 min.
Ijede has secondary forest vegetation of mostly broadleaved evergreen or semi-deciduous forest, with swampy areas. It also has two peaks of rainfall in June and September with a mean annual rainfall of about 1900mm ± 250mm and humidity averaging 77%. March is the warmest month of the year with an average temperature of 32.4°C at noon, while August is coolest with an average temperature of 22.6°C at night. The time around January (harmattan season) is the driest month. Ijede has a relatively stable electric power supply as the 1320 MW Egbin Thermal Station, the biggest in West Africa, is situated just next to the community. The Nigerian Institute of Medical Research, Yaba, Lagos, has been carrying out malaria research projects in Ijede Health Centre (now General Hospital, Ijede) since 2001. The Hospital is also one of the 14 sentinel sites for Drug Therapeutic Efficacy Trials (DTET) of antimalarial medicines established by the National Malarial Elimination Programme (NMEP), of the Federal Ministry of Health.
Conceptualization
The Institute conceptualized the need to have a stable community within the Lagos environs that would serve as a site for a demographic and health surveillance system and furnish routine health-related data that would inform health policy. The site, after a thorough characterization, could also be used for future vaccine and drug trials. After consideration of various semi-urban communities, such as Bayeku, Ikorodu, Badagry, and Epe, Ijede community in the Ikorodu Local Government Area was eventually chosen, as NIMR already had a presence in the community via the Malaria Programme. Visits were paid to the Ijede LCDA chairperson, the traditional ruler of the community, and the Medical Officer of Health of the LCDA to brief them on the study, the expected benefits to the inhabitants of the community, and solicit their support and cooperation for the project. Technical meetings were held among the study team to plan the logistics of the project. Consequently, a total of 52 Enumeration Areas (EAs) maps, corresponding to Ijede community, were obtained from the National Population Commission (NpopC) based on the delineated Enumeration Areas for 2006 Census (Nigeria Bureau of Statistics, 2006), for the listing and mapping exercise.
Fieldwork preparation
For ease of data capture, a questionnaire was developed to capture data on housing units and their inhabitants. This tool was tested and uploaded to the electronic device (Android Tablets/ phones) used for the mapping exercise. Field workers and community mobilizers were given a one-day training on community entry, identification of Enumeration Areas, reading of the sketched maps, data capture using the Computer Assisted Personal Interview (CAPI) method as well as capturing the housing units coordinates (longitude and latitude) through the GPS within 5 meters accuracy.
Each Housing Unit was given a number with the format NIMR/2018/EA code/Building number. The Enumeration Areas already had 4-digit codes from the National Population Commission, which were retained for the numbering of housing units in this project. Since there were less than 200 housing units in any enumeration area in Ijede, the EA code had 4 digits and the building number had 3 digits. As an example, the fifth characterized house in Enumeration Area 3285 was numbered NIMR/2018/ 3285/005.
Field mapping and listing of households
After the training, the fieldworkers carried out the following activities:
(i) Obtained the Enumeration Area (EA) Map of the location to be listed,
(ii) Approached the local leaders of the communities and the EA site for permission to work in the area, after explaining their mission, (iii) Began with the “starting point” on the EA map to identify current structures within the boundaries of the EA, and
(iv) Numbered all the buildings/structures within EA.
In identified residential structures, the workers explained their mission and the concept of a ‘household’ to the occupants they met. A household is a unit of one or more persons living in the same structure and sharing meals (Jenkinson, 1999). The workers then identified the households occupying the buildings and listed them with all members (including those absent at the time of enumeration), but living in the dwelling at that moment. The name of the head of the household and the age and sex of the individual members of the households were captured directly using a designed web-based template on a data-capturing tablet and streamed real-time to a central server. Socioeconomic characteristics of the head of the households were also obtained. The workers sketched the Cluster that had been mapped on A3 paper indicating all current structures and landmarks within the EA boundaries.
Data management
All the completed entries for each household were checked for completeness and accuracy by the supervisor before being sent to the central server for the study. Data were subsequently retrieved, downloaded, and transferred to Microsoft excel for cleaning and analysis by the data officers. Data analysis was with descriptive statistics and results are presented as tables and charts.
Ethical consideration
Ethical approval for the project was obtained from the Institutional Review Board (IRB) of the Nigerian Institute of Medical Research, Lagos Nigeria. Social approval for the project was got from the Lagos State Ministry of Health. Advocacy visits were paid to the Lisa (traditional ruler) and his council, the Chairperson of Ijede LCDA, and the Medical Officer of Health (MOH) of Ijede LCDA before the commencement of the project. The Lisa ensured that the information on the project was disseminated to the community through the town crier in announcements in various religious gatherings. The Health Educator of the community and two other workers in the office of the LCDA Chairperson also went with the field workers to facilitate community entry. Verbal consent was obtained from each household head before the survey was conducted.
RESULTS
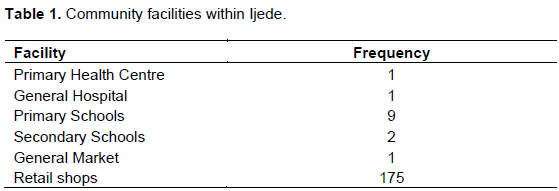
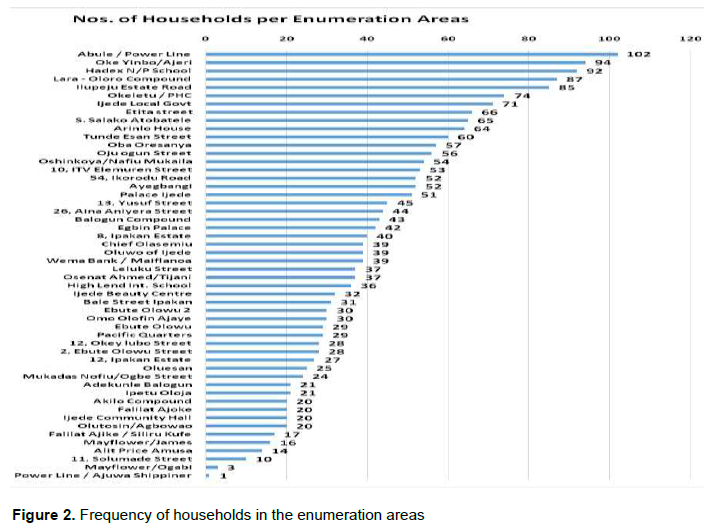
Fifty-two enumeration areas were characterized. The facilities in the community included health facilities, schools, and markets as outlined in Table 1. The retail shops are mainly small grocery shops in front of many residential buildings. There were 2,171 households in the 52 EAs. The median number of households per EA was 38 (IQR 25 - 55). Abule/Powerline EA had the highest number of households while Ajuwa Shippiner had the lowest. Figure 1 depicts the map of EA 3670 as obtained by an enumerator while Figure 2 depicts the number of households per EA in Ijede.

Living accommodation
The 2,171 households identified lived in different kinds of residential accommodation with the multifarious tenement building, commonly called “face me, I face you”, being the commonest. These are large, sometimes multi-story buildings with several single rooms or room-and-parlour units, each occupied by a household. Other living structures included blocks of flats, multi-compounds i.e. several buildings in one enclosed compound, each with one or more households, and shacks/squatter settlements.
Population
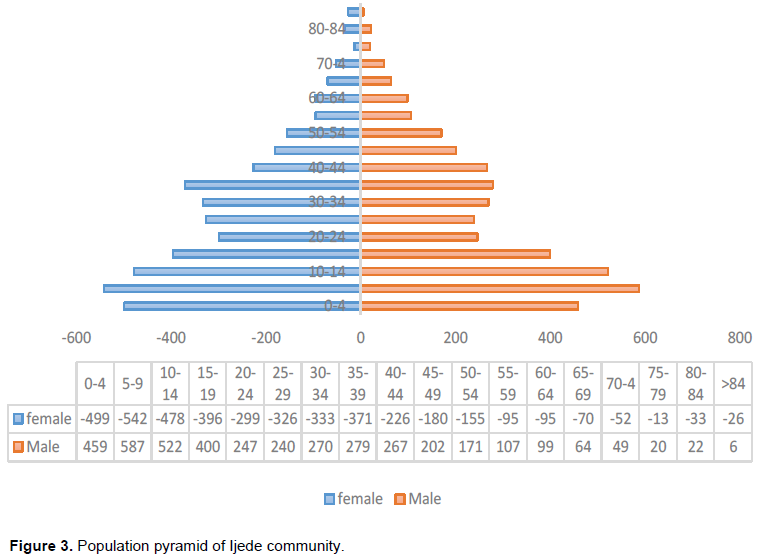
The population of the mapped 52 EAs in 2,171 households was 8,208. There were slightly more females than males (4,131 [50.3%]) than males (4,077 [49.7%]) but the male: female ratio was 1.1. No age was recorded for eight persons so they were not included in age group calculations and the construction of the population pyramid.
Children aged 0-4 years constituted 11.7% of the population, while 47.4% were aged less than 20 years. Women of childbearing age (15-44 years) made up 20.1% of the population. Figure 3 depicts the population pyramid of the community. Concerning the proportion of females in the different age groups, there were proportionally more females in the age group 15-29 years (53.5%), 30-44 years (53.3%), and those aged 60 years and above (52.6%) when compared to the age group of 0-14 years (49.2%) and 45-59 years (48.8%).
Households
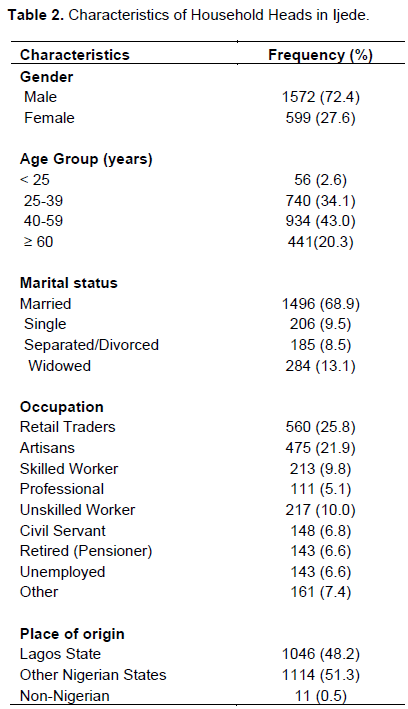
Household members ranged from one person to 13 persons with a mean of four persons per household. Three- to five-person households were in the majority at 1,130 (52.0%) and 11-13- person households constituted the least at 13 (0.6%). Of the 2,171 household heads, majority were males (72.4%), in the age group of 40-59 years (43.0%), married (68.9%), and retail traders (25.8%). About half of the household heads were indigenes of Lagos State (48.2%), while the rest were from other states in Nigeria (51.3%), and a minority was from neighbouring West African countries (0.5%). The characteristics of the household heads are detailed in Table 2.
Facilities in households in Ijede
All households in Ijede had access to electric power supply. Majority of households owned television and mobile phones. However, ownership of refrigeration facilities for food preservation was available in less than 60% of households. Assessment of the Water, Sanitation, and Hygiene (WASH) facilities in Ijede showed that the major source of water supply for drinking and other household use was a borehole (59.6%). The water was purified in 40% of households and the major means of purification was by boiling (93.3%). Toilet facilities were the flush (water closet) type in most households (74.7%). However, pit latrines without slabs covers and bucket latrines constituted 15.4% of toilet facilities. Cooking fuel was liquefied natural gas and kerosene in the majority of cases (69.5 and 64.2% respectively) and the cooking was done within the house in 82.4% of cases.
DISCUSSION
Community listing and mapping are essential strategies for baseline characterization of physical features, landmarks, and households existing in a particular environment (Rocheleau, 2005; Marcil et al., 2016). These processes establish collaboration between communities and health/research institutions involved thus strengthening health programs and identifying public health conditions affecting the communities under investigation (Marcil et al., 2016). The Nigerian Institute of Medical Research (NIMR) conducted a social mapping and listing exercise in Ijede community, a local council development area in Ikorodu Local government area of Lagos State, Nigeria with an ultimate aim to establish a Health and Demographic Surveillance System.
In this survey, 52 enumeration areas with a population of 8208 were listed in Ijede community. The male to female ratio [number of males per 100 females] was 98. The dependency ratio in the survey was 41.9%. Majority of the household heads are gainfully employed with a significant proportion being retail traders and artisans living in multifarious compounds. The commonest source of water supply for drinking and other household use is borehole (59.6%) and piped water (23.4%), while the flush system [74.7%] was the commonest form of sewage disposal. The majority of respondents had access to electricity supply, mobile phones, and mass media. The distribution of the population with respect to gender depicts males per 100 females of 98, showing the slight preponderance of the female gender. This finding is similar to the 2018 NDHS survey of males per 100 females of 97 (National Population Commission (NPC) [Nigeria] and ICF, 2019).
The dependency ratio of approximately 42% is slightly lower than the national report of 50% (National Population Commission (NPC) [Nigeria] and ICF, 2019).
Although a similar proportion of the dependent adults (>65years) is reported in the current survey, the reasons for the slight variation in the overall dependent population could be due to our semi-urban setting compared to the NDHS which was inclusive of rural and urban settings. Furthermore, our dependency ratio is similar to reports in other African countries (United Nations, Economic Commission for Africa and UNFPA, 2016; United Nations, 2019). The average urban household size in Nigeria is 4.3 persons with a majority of the households headed by men, which is in agreement with our findings (National Population Commission (NPC) [Nigeria] and ICF, 2019). The broad-based population pyramid in this survey is similar to the population pyramids of Nigeria and other African countries; and thus, affirms the fact the Nigerian and the African population has a low life expectancy and high fertility rate (United Nations, Economic Commission for Africa and UNFPA, 2016; National Population Commission (NPC) [Nigeria] and ICF, 2019; United Nations, 2019).
The access to improved water supply in this community (100%) with approximately 40% of the populace further purifying the water, mostly by boiling, is above that reported by both the Lagos State Household Survey 2010 (Lagos Bureau of Statistics, 2010)and the Nigerian DHSS 2018 (National Population Commission (NPC) [Nigeria] and ICF, 2019). The presence of a mini-water work close to this community may appear to be responsible for this improved access to potable water. However, access to piped/tap water (from the waterworks) remains low at 23.4%, with the major source of water supply being the borehole. The improved water access may therefore be due to the semi-urban nature of the community with dug-up underground water and boreholes serving majority of households.
The predominant sewage disposal system is the flush system (water closet) in most households (74.7%). This again may be accounted for by the semi-urban nature of the community. It is thus expected that diseases associated with poor sanitary conditions such as diarrhea and cholera will not be endemic in this community. However, pit and bucket latrines without slab covers constituted 15.4% of toilet facilities. These toilet facilities are likely to be shared by households considering the tenement style residential buildings with shared facilities constitute the major type of household dwelling. This is contrary to the 2018 DHSS (National Population Commission (NPC) [Nigeria] and ICF, 2019), which reported that the predominant sewage system was the pit latrine system, which is not shared by households. The varied difference could be attributed to the ease of access to water supply, the semi-urban characteristics of the environment, in addition to the socio-economic and development advancement of Lagos as the commercial hub of the nation.
The ease of access to electricity in this community is consonance with the Lagos state fact sheet on electricity supply (Lagos Bureau of Statistics, 2013), though contrary to report at the national level where only 59%of households have access to electricity (82% in urban and 39% in rural areas) (Jenkinson, 1999). The plausible reason for this ease of access is due to the presence of a functional power station in the vicinity.
Liquified natural gas (LNG) and kerosene were the commonest cooking fuels used within the households. The readily available access to LNG is explained by Lagos state’s drive to increase uptake of cleaner cooking fuels. This finding is contrary to the national survey showing 69% of households using solid fuels for cooking (National Population Commission (NPC) [Nigeria] and ICF, 2019). Exposure to indoor smoke has potentially harmful health effects. This highlights the need for measures to limit the hazardous effect of exposure to indoor smoke in the community.
This baseline survey [DHSS] would aid the institute in addressing health concerns of the community as well as help formulate much-needed policies to improve the overall health and wellbeing of inhabitants of the community. The Ijede DHSS reflects the Nigerian sociodemographic characteristics and thus would serve as a veritable study site (clinical and field trials) in line with the mission of the institute to conduct research into diseases of public health importance, develop structures for the dissemination of research finding as well as provide enabling environment for health research.
CONCLUSION
The demographic profile of Ijede projects a population that reflects the Nigerian demographic scenario with features tending towards urbanization. Hence, establishing a DHSS provides continuous demographic monitoring and health-related data that can inform health policy in Lagos State and Nigeria.
LIMITATIONS
The main limitation of this cross-sectional study is inability to measure trends over time. However, several baseline demographics have been established, which can form the basis of in-depth prospective studies, in the planned DHS. The survey was also impacted negatively by funding constraints that limited the study’s capacity to list and map the entire Ijede community and its environs.
CONFLICT OF INTERESTS
The author has not declared any conflict of interests.
REFERENCES
|
Aday LA, Cornelius LJ (1990). Designing and conducting health surveys: a comprehensive guide, Choice Reviews Online. |
|
|
Corsi DJ, Neuman M, Finlay JE, Subramanian SV (2012). 'Demographic and health surveys: a profile', International Journal of Epidemiology 41(6)1602-1613. |
|
|
El-Zanaty F, Way AA (2000) Egypt Demographic and Health Survey. |
|
|
Federal Office of Statistics and IRD/Macro International Inc. (1992) Nigeria Demographic and Health Survey 1990. |
|
|
Fisher AA, Way AA (1988). The demographic and health surveys program: An overview, International Family Planning Perspectives. |
|
|
Gambia Bureau of Statistics (2014). The Gambia Demography and Heath Survey, The Gambia Demography and Health Survey. |
|
|
ICF (2016). The DHS program: demographic and health surveys, DHS Model Questionnaires. |
|
|
ICF Macro (2009). 'Measure DHS Demographic and Health Surveys', The DHS Program Demographic and Health Surveys, pp. 1-16. |
|
|
Jenkinson C (1999). 'Measuring Health Status and Quality of Life' 1998, Question Bank Topic Commentary on Health', Question Bank Topic Commentary on Health P 7. |
|
|
Khan OA, Skinner R (2011). Geographic Information Systems and Health Applications, Idea Group Publishing. IGI Global. |
|
|
Lagos Bureau of Statistics (2010). Further analysis of lagos state specific demographic and socio- economic data / indicators. |
|
|
Lagos Bureau of Statistics (2013). Household survey 2013. Lagos Bureau of Statistics, Ministry of Economic Planning and Budget, the Secretariat, Alausa, Ikeja, Lagos. |
|
|
Maplandia.com (2016). Ijede Google Earth 3D map | Mainland, Lagos, Nigeria in Google Earth. |
|
|
Marcil L, Afsana K, Perry HB (2016). 'First Steps in Initiating an Effective Maternal, Neonatal, and Child Health Program in Urban Slums: the BRAC Manoshi Project's Experience with Community Engagement, Social Mapping, and Census Taking in Bangladesh', Journal of Urban Health: Bulletin of the New York Academy of Medicine 93(1). |
|
|
National Population Commission (NPC) [Nigeria] and ICF (2019). 'Nigeria Demographic Health Survey 2018', The DHS Program ICF Rockville, Maryland, USA P 748. |
|
|
Nigeria Bureau of Statistics (2006). Nigeria - General Household Survey 2006, Third edition - Overview. |
|
|
Plescia M, Koontz S, Laurent S (2001). Community Assessment in a Vertically Integrated Health Care System Primary Data. American Journal of Public Health 91(5):811. |
|
|
Rocheleau D (2005). 'Maps as Power Tools: Locating Communities in Space or Situating People and Ecologies in Place?', Communities and Conservation: Histories and Politics of Community-based Natural Resource Management. |
|
|
United Nations (2019). 'World Population Prospects 2019: Data Booklet', Department of Economic and Social Affairs Population Division, pp. 1-25. |
|
|
United Nations, Economic Commission for Africa and UNFPA (2016). The Demographic Profile of African Countries. |
|
|
World Population Review (2020). Lagos Population 2020 (Demographics, Maps, Graphs). |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


