Full Length Research Paper
ABSTRACT
Early pregnancy in school settings is a social, economic and health phenomenon that can hamper the development of countries. This study aims to determine the factors associated with this phenomenon in the health district of Lokossa-Athiémé in southwestern Benin in 2018. The study employed a case-control method. The participants were secondary school girls aged 10 to 19 at the time of the study, enrolled in a public secondary school in the health district of Lokossa-Athiémé and having contracted a pregnancy during school year 2017-2018 In each case, we set three samples selected by simple random choice among girls aged 10 to 19 who had never contracted a pregnancy in the same district, the same secondary school and the same year of study. Data collection was carried out by interviewer-respondent using a questionnaire in accordance with ethical principles. The factors associated with early pregnancies were determined using a multiple conditional logistic regression model at 5% threshold. The average age of case-controls was 17.86 ± 1.34 years and that of participants was 16.75 ± 1.56 years. The factors associated with school-based pregnancies were age greater than 15 years (OR = 6.54; p = 0.045), the existence of an income source other than parents’ (OR = 9.43; p = 0.001), insufficient parental control (OR = 5.83; p = 0.011), low self-esteem (OR = 4.93; p = 0.011) and lack of family sex education (OR = 3.04; p = 0.039). The current study reveals the importance of family circle in controlling the problem of pregnancies in school settings.
Keywords: Early pregnancy, school settings, associated factors, Lokossa-Athiémé, Benin.
INTRODUCTION
Adolescence is a critical period in life from 10 to 19 years old, marked by the transformation from childhood to adulthood. It is characterized by great physical changes such as the onset of secondary and psychological sexual characteristics (United Nations Population Fund (UNFPA), 2013). It disrupts the habits, experiences and self-image established since childhood, both among young people themselves and among their parents, the extended family circle and the social network (Goldbeter-Merinfeld, 2008). This is the case with risky behaviors including early sexuality which can affect the health and future of adolescents and young people. According to statistics, most boys and girls in the world have sex at the age of 15 or earlier (Long, 2011). In Benin, the 2012 Demographic Health Survey reveals that 45% of respondents had had their first sexual experience before the age of 18 (National Institute of Statistics and Economic Analysis (NISEA) Benin, 2013).
Indeed, early sexual intercourses often lead to early pregnancies, the immediate and long period consequences of that are loss of schooling possibility and other opportunities, deaths from clandestine abortions, perpetuation of poverty and girls inability to reach their full potency (UNFPA, 2013). Early pregnancies are public health problem.
To reduce the rate of this phenomenon, many initiatives have been taken around the world. In 2011, the World Health Organization (WHO) published in partnership with the United Nations Population Fund (UNFPA) guidelines on the prevention of early pregnancies and their consequences (WHO, 2015). In Benin, the Ministry of Health is implementing a national, multisectoral strategy for the sexual and reproductive health of adolescents and young people for 2010-2020 so as to improve the sexual health of adolescents and young people. It is essentially based on information and offering sexual health services adapted to adolescents and young people (listening, family planning, management of sexually transmitted infections), with a view to responsible sexuality (Ministry of Health of the Benin, 2010). Despite these efforts, pregnancy in school settings remains a worrying reality that is on the rise in Benin. During the 2016-2017 school year, approximately 2,763 cases of pregnancy were recorded in schools out of 301,821 girls enrolled, that is a proportion of 0.92% (Ministry of Secondary, Technical and Vocational Education of Benin, 2017). In the health district of Lokossa-Athiémé, the number of pregnancy cases in schools rose from 35 in 2017 to 46 in 2018 according to statistics from the Departmental Directorate of Technical Secondary Education and Vocational Training of Mono. Despite its expansion, this phenomenon is poorly documented in Benin. It is to fill this gap that the current study was initiated to identify the factors associated with early pregnancies in schools in the health district of Lokossa-Athiémé. Its results will help improve strategies to fight against early pregnancies in school settings.
MATERIALS AND METHODS
Study framework
The study was carried out in the public secondary schools in the health district of Lokossa-Athiémé. With an area of ??498Km², this district is located in the southwest of Benin Republic and is made up of the municipalities of Lokossa and Athiémé which has 23 secondary schools including respectively 13 and 10 in the municipalities of Lokossa and Athiémé. The secondary schools in Benin set from the 7th to 13th class of the school curriculum that is awarded by the Baccalaureate diploma. We distinguish between private and public secondary schools; but this study focused on audiences usually attended by children of parents of low socioeconomic status. According to statistics from the Ministry of Secondary Education, for the 2017-2018 academic years, 14,816 students were enrolled in the Lokossa-Athiémé health district including 8,694 boys and 6,122 girls, which is a sex ratio of 1.4 in favor of boys.
Study design
This was a case-control study carried out from June 1 to July 15, 2018, focusing on adolescent girls enrolled in public secondary schools in the health district of Lokossa-Athiém for the school year 2017-2018.
Participants
The cases were secondary school girls aged 10 to 19 years at the time of the study, enrolled in a public secondary school in the health district of Lokossa-Athiémé for 2017-2018 school year and having become pregnant during the same school year. Secondary school girls meeting these criteria but who did not give their consent or were not present on the day of data collection and whose address was not known to school authorities and classmates were excluded. The controls were selected from among secondary school girls who had never contracted a pregnancy and who were enrolled in public colleges who had registered at least one case of pregnancy during the 2017-2018 school years in the Lokossa-Athiémé health district. The controls selected but who did not give their consent was excluded from the study. The match was done on the basis of the municipality, the secondary school and the year of study, focusing one case for three controls. For each case, the control was selected in the same municipality, in the same secondary school and in the same year of study.
Sampling
To identify the cases, the list of public secondary schools in the health district of registration of at least one case of early pregnancy during the year 2017-2018 was obtained from the Departmental Directorate of Technical Secondary Education and Vocational Training of Mono. In the secondary school concerned, the list of cases of early pregnancy was desegregated by year of study. Pregnant girls meeting the required condition were included in the sample exhaustively. For the samples, the selection was made by simple random choice. For each case identified in a class, a simple random choice of three samples was made in the same class. The sampling frame consisted of the list of all adolescent girls (aged 10 to 19) in the same class who had never contracted a pregnancy until the day of data collection. In case only three girls met the selection criteria in the classroom, they were systematically enrolled. When less than three girls met the criteria for selection of controls in a class, the supplement was sought in the same year of study from another teaching group from the same secondary school. When the secondary school has more than two teaching groups, a simple random choice was made to take one.
Variables
The variables studied included: socio-demographic characteristics (age, family type, sibling rank, and marital status, place of residence, educational level, ethnicity and religion), socio-economic (monthly pocket money, existence of a secondary source of income, level of socioeconomic well-being), characteristics of the social settings (peer influence, parental control, parent-child communication skills).
The adolescent's socioeconomic level was determined by a composite indicator of the household economic well-being that it belongs to. It was built according to the approach of (Filmer and Pritchett, 2001), focusing on the characteristics of the household and its assets which rate was calculated and then divided into tertiles. The first, second and third tertile correspond respectively to the low, medium and high socioeconomic level.
Parental control and parent-child communication skills were assessed according to the scale used to assess parental educational practices (Claes et al., 2010). Parental control was measured through the parental authorization criteria, school supervision and family rules. The appreciation of parent-child communication was made through the openness criteria, self-disclosure and problematic aspects of communication. Self-esteem was measured with the Rosenberg Self-Esteem scale made up of ten statements that focus on a person's level of worth as well as the satisfaction they feel with themselves (Vallieres and Vallerand 1990).
The methods for the different variables were spited into several questions and each response rated from 1 to 4. The average scores were calculated for each variable, from the minimum and maximum rates. Thus, for parent-child communication skills, the maximum expected rate was 20 and the minimum was 5, with an average of 12.5 Parental control had a maximum expected score of 28 and a minimum of 7, with an average of 17.5 Self-esteem had an average rate of 25.5, with an expected low of 10 and a high of 40. For each of the variables, the average rate was used as an assessment threshold. The character corresponding to the variable was therefore weak / insufficient when the total rate obtained by the respondent is lower than the average and strong / sufficient when it is greater than or equal to the average required.
Data collection tools
The data were collected by addressing a questionnaire, previously pretested in one of the secondary schools in the commune of Houeyogbé located in the same district as Lokossa and Athiémé.
Data analysis
The data collected were grabbed using the Epi info 7.2.1.0 software and analyzed with the Stata 11 software. The description of the sample was made using the parameters of central tendency (mean ± standard deviation) and dispersion (median and quartiles) for the quantitative variables and the proportions for the qualitative variables.Factors associated with early pregnancies were identified by univariate and multivariate analysis. The univariate analysis done by method of a simple conditional logistic regression has allowed determining associations between dependent and independent variables through the odds ratios or raw Odds Ratio (OR) and their 95% confidence interval [95% CI]. Crossings between independent variables were also carried out in order to identify interactions. The chosen significance level was 5%. In multivariate analysis, a multiple conditional logistic regression model was used. Variables with a p-value of less than 20% during univariate analysis were introduced into the initial model of multiple conditional logistic regressions with step-down elimination. The variables retained in the final model were those with a p-value of less than 5%. The reference modalities were those that are least risky.
Ethical considerations
The authorization from the Departmental Director of Technical Secondary Education and Vocational Training of Mono, Directors of the various secondary schools and informed consent of parents' association had been obtained before data collection starting. All targets had been informed of the nature and objectives of the study and given their consent before the questionnaire addressing. It was explained to them that the data are treated anonymously and confidentially and they are free to ‘‘stop answering questions whenever they want. For this end, the questionnaire did not mention any identity and was addressed within isolated location so as to avoid eavesdropping on conversation by other people, thus ensuring confidentiality.
RESULTS
Description of the sample
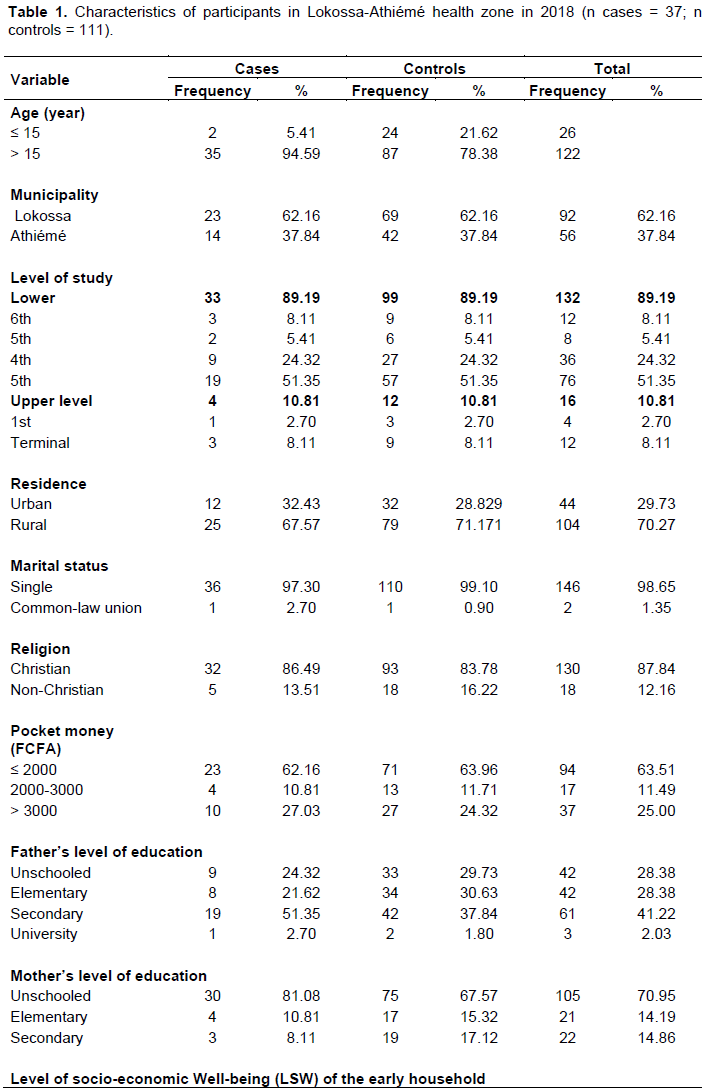
The average age in the sample was 17.03 years ± 1.57 with 17.86 years ± 1.34 for cases and 16.75 years ± 1.56 for respondents. The majority ethnic group represented was that of Kotafon with 59.46% among cases and 41.44% among respondents. The average parent-child communication rate was 10 ± 3.14 in the sample, respectively 8.84 ± 3.11 and 10.38 ± 3.06 in cases and respondents. For parental control, the overall average rate was 18.78 ± 4.07, 16.22 ± 4.02 in cases and 19.63 ± 3.72 in respondents. Among the participants 54.05% had already had at least one intercourse. The median age at first sexual intercourse was 16 years with an IIQ of 3 years in cases and respondents. Also, almost all of the cases and 66.67% of the participants had a boyfriend. The partner’s average ages of the cases were 21.70 years ± 3.08 and that of the respondents’ partners was 20.09 years ± 2.76. Other characteristics of the sample are summarized in Table 1.

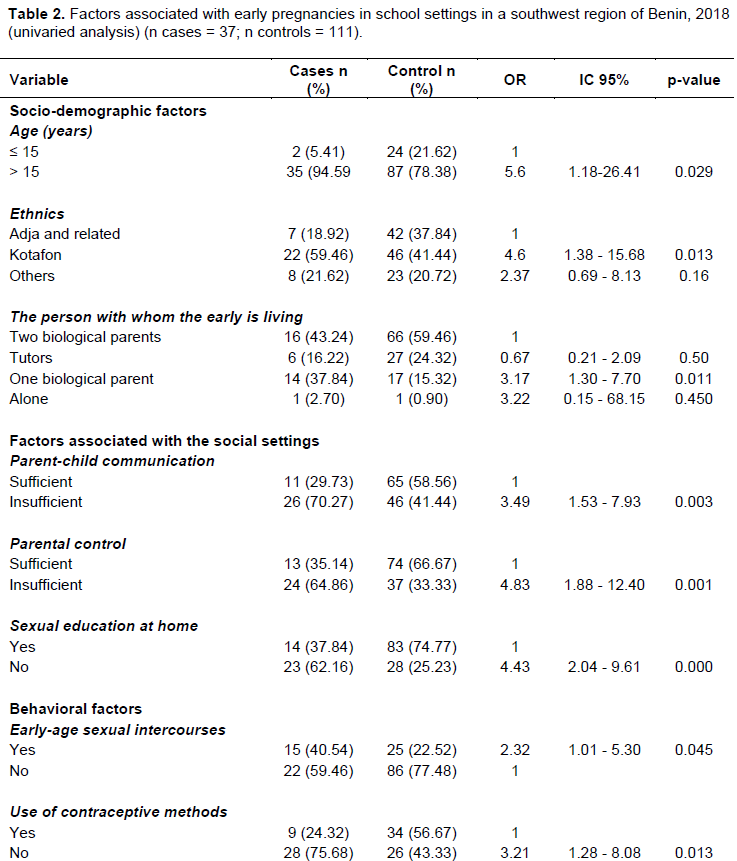
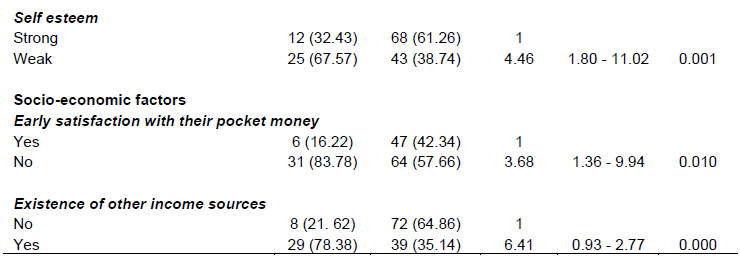
Identification of factors associated with early pregnancies by univariate analysis
Through univariate analysis, the factors associated with early pregnancies are summarized in Table 2.
Multivariate analysis
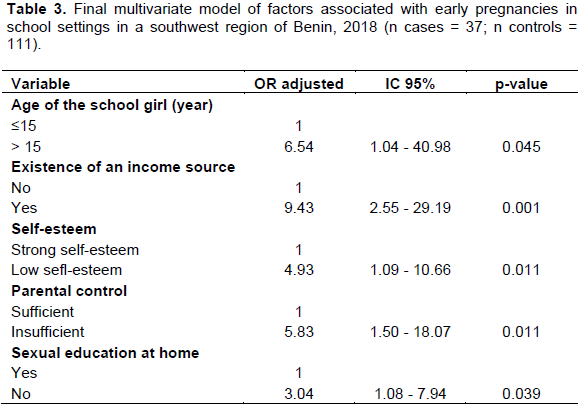
The multivariate analysis showed that all things being equal, secondary school girls over 15 years of age, those with a secondary income source, low self-esteem, insufficient parental control and a lack of family sex education were more likely to be the victim of early pregnancy in school settings (Table 3).
DISCUSSION
The choice of study type is justified by the low frequency of early pregnancies in schools. In addition, the level of parental control, parent-child communication skills and self-esteem were assessed with international standard. Finally, the factors associated with pregnancies were identified by a conditional logistic regression model. These methodological arrangements were made to ensure validity of the results. However, the current study could be matter of biases in particular about selection and information. Indeed, among the respondents, some secondary school girls could have lied about their pregnancy history, thus inducing a selection bias. Information biases could be linked on the one hand to the sensitive nature of the themes (pregnancy and sex life of the respondents) and to the memorization on the other hand. These biases were minimized by the respondents’ confidence and the anonymous nature of the survey. Recalling bias could be related to issues such as age of first sexual experience and history of pregnancy that however are so important in an individual's life to be forgotten. Beyond these possible biases, we consider that the results of this study can be extrapolated and constitute an inventory that can contribute to fighting against early pregnancies in Benin school settings.
The sample's average age is very close to that of several other authors. Indeed, a study carried out in 2015 by Glèlè et al. of adolescents living in community in Lokossa had reported an average age of 17.75 ± 3.1 years (Glèlè Ahanhanzo et al., 2018) and Melaku et al. in Ethiopia, 16.55 years in 2014 (Melaku et al., 2014).
Of the 37 recorded early pregnancies, 33 (89.19%) were in the first cycle and 4 (10.81%) in the second of secondary school. Probably, not because senior adolescent girls are more conscientious but because they are few in number due to dropout mainly caused by early pregnancies. More than half of early pregnancy cases (19/37, or 51.35%) are in the fourth grade, class where the exam is prepared to give access to the first secondary school diploma. Early pregnancies being a factor in school dropout, these adolescents risk dropping out of school without a diploma that can allow them to reorient themselves in professional settings.
The median age at first sexual intercourse (16 years) is close to the results of (Ahodakin, 2015). (16.1 years), but higher than that reported by Glèlè et al. in 2018 in Benin (14.75 years old) (Glèlè Ahanhanzo et al., 2018) and in the 2017-2018 Demographic and Health Survey, where more than 50% of adolescents had their first sexual intercourse before the age of 15 (NISEA, 2018). This difference in the age of the first sexual intercourse could be explained by the fact that these two studies were carried out in community whereas the current one focuses only on adolescent girls in secondary school. It may reflect a beginning of awareness about advantage of the adolescent girls’ education. In fact, adolescent girls in school are under pressure from academic activities and parents. They also acquire awareness sessions organized to their sake. However the relatively early sexual intercourse (compared to the current study) reported by the Health Behavior in School-aged children survey in Brussels (first sexual intercourse at 14.9 years) (Beghin et al., 2006) could reflect the Western context where sexuality is not a taboo as in African society.
The association between age and the onset of early pregnancies was also revealed by (Amouzou, 2014). who had reported in Senegal that the risk of contracting a premature pregnancy increased significantly according to the age of adolescent .One might think that with puberty at average of 14 years, development of sexual characteristics and observable morphological transformations, the adolescent not only becomes a covetousness for the male sex by her attractive morphology but also by her risky behavior. The results of secondary school girls fewer than 15 appear to be pregnant is in accordance with the median age of first sexual intercourse that is 16 years according to our study. Although 94.59% of pregnancies were recorded among secondary school girls over 15 years of age, the distribution of the sample by level of education shows that only about 11% of pregnancies were among senior secondary school girls. This could be justified by the natural sciences course which addresses human reproduction in the second cycle of secondary school. In view of these results, inserting of human reproduction concepts and sexual education in the first cycle of secondary school would have more beneficial effects in terms of fighting against early pregnancies in school settings.
According to Rosenberg and James quoted by Potard, self-esteem is defined as the more or less favorable feeling that each individual has towards his own person (Potard, 2010). The link between low self-esteem and coming of early pregnancies corroborates with the results of Potard in France in 2010 that reported that low self-esteem is associated with sexual risk-taking and a greater frequency of unplanned pregnancies (Potard, 2010). According to (Boden and Horwood. 2006) sexuality and self-image influence each other. A low self-esteem would reduce the psychological resources of adolescent girls implying calmly communicating hardship on topics relating to sexuality with their partners. They would be afraid of being rejected. These difficulties relating to self-confidence could make them more vulnerable in a weak comfort and ready to accept suffering. In contrast, low self-esteem could by complexity lead adolescent girls to adopt risky sexual characteristics to assert themselves in their social settings forgetting or ignoring the consequences of their actions.
The lack of family sex education as a factor associated with the occurrence of early pregnancies in school reflects practices in conservative socio-cultural settings that continue to make sexuality a taboo issue. Glèlè et al. went in the same direction, reporting that weak communication between parents and children about sex was associated with early sexual initiation (Glèlè Ahanhanzo et al., 2018).
It is no longer to be demonstrated that in African families sexuality remains a taboo issue. Parents who have not had such an education would feel embarrassed or ashamed when it comes to discussing issues of sexuality with their children. Especially when parents mainly mothers are of low educational level as in this study, this dialogue is difficult to set. For Adjahoto et al., The parent’s difficulty to conduct a gender-based conversation with children leads them to seek sometimes unreliable information outside the family settings (street, friends, and media) (Adjahoto et al., 2000). Thus, insufficiently armed girls fail to resist pressure from boys and engage in sexual intercourse without precaution leading them to early pregnancy.
Family is the primary educational framework for a child who will grow up to be an adolescent, young person and then an adult. A favorable family setting to adolescent education is a protective factor against risks. A comparative study conducted by (Stephenson et al., 2014). in four African countries (Burkina Faso, Ghana, Malawi, Uganda) among adolescent girls aged 15-19 reported that regular parental control protected adolescent girls from early sex. A cohort study focusing on adolescents aged 12 to 16 in Nairobi also found that lack of parental control and family instability were associated with premature sexuality especially among adolescents (Marston et al., 2013). Indeed parental control helps to curb risky behavior and negative peer influence and reduce its consequences. Parental control coupled with family sex education would be more beneficial to adolescents and make them more responsible for her sexuality.
The pocket money of adolescent girls seems insignificant (27.03% of cases and 24.36% of respondents receive more than 3000 F CFA per month) but perhaps reflects the socio-economic level of households and adolescent girls should be content with it. Unfortunately, dissatisfaction with their pocket money, disproportionate ambition, and easy-earning lure might justify looking for a secondary income source provided in most of time by their boyfriend. Redeem of the favors bestowed by boyfriend on earlyr is very often sex, the earlyr will have no other choice but accepting the boyfriend pressure for fear of losing latter favors. Base on lack of sexuality education background and poor parental control this addiction could lead earlyr into risky sex that can lead to early pregnancy.
CONCLUSION
Early pregnancies in school settings by their upward trend constitute a major public health concern. This study has identified five factors associated with this phenomenon. Most of these factors can be avoided by the combined action of qualified authorities at various levels concerning parents and adolescent girls. Efforts are already being made at the Government level with gradual sex education insertion in school training curricula. A large part of the responsibility falls on the parents as they need to be supported in their role of children sexuality education.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interest.
ACKNOWLEDGMENTS
The authors are grateful to the Departmental Director of Secondary Education, Technical and Vocational Training of Mono and his staff for the ease in the administrative formalities essential for data collection. They also appreciate the directors and administrative staff of municipalities’ secondary schools of Lokossa and Athiémé for their confidence, their availability and their contribution to carrying out the study. The parents for the consent given and secondary school students for trust, consent and participation in the study are also appreciated.
REFERENCES
|
Adjahoto EO, Hodonou K, De Souza A, Tété V, Baeta S (2000). Information des jeunes en matière de sexualité. Cahiers d'études et de Recherches Francophones 3(10):195-199. |
|
|
Ahodakin HM (2015). Prévalence et facteurs de risque des avortements provoqués chez les adolescents en milieu scolaire à Parakou. Thèse de Médecine; Université de Parakou ; n°109: 72p. |
|
|
Amouzou M (2014). Famille et grossesse précoce au Sénégal: Maternités adolescentes. |
|
|
Beghin D, Cueppens C, Lucet C, Ndamè S, Masuy-Stroobant G, Sasse A, Piette D (2006). Adolescentes: sexualité et santé de la reproduction. Etat des lieux en Wallonie et à Bruxelles. Bruxelles. Avec le soutien de la Communauté française de Belgique, p. 80. |
|
|
Boden JM, Horwood LJ (2006). Self-esteem, risky sexual behavior, and pregnancy in New Zealand birth cohort. Archive of Sexual Behavior 35(5):549-560. |
|
|
Claes M, Debrosse R, Miranda D, Perchec C (2010). Un instrument de mesure des pratiques éducatives parentales à l'adolescence : validation auprès d'adolescents du Québec et de France. Revue Européenne de Psychologie Appliquée 60(1):65 78. |
|
|
Filmer D, Pritchett LH (2001). Estimating wealth effects without expenditure data or tears: an application to educational enrollments in states of India. Demography 38(1):115-132. |
|
|
Fonds des Nations Unies pour la (UNFPA) (2013). La mère-enfant : face aux défis de la grossesse chez l'adolescente. [En ligne] Disponible sur : |
|
|
Glèlè Ahanhanzo Y, Sossa-Jérôme C, Sopoh G, Tchandana M, Azandjèmè C, Tchamdja T (2018). Factors associated with early sexual intercourse among earlyrs and young adults in rural south of Benin. Journal of Public Health in Africa 9(2):88-91. |
|
|
Goldbeter-Merinfeld E (2008). L'adolescence en contexte : Cahiers critiques de thérapie familiale et de pratiques de réseaux. Belgique : Bruxelles. [En ligne]. Disponible sur: |
|
|
Institut National de la Statistique et de l'Analyse Economique (INSAE). (2013). Enquête démographique et de Santé (EDSB IV). [En ligne]. Disponible sur |
|
|
Institut National de Statistiques d'Analyse et d'Economique (INSAE). (2018). Enquête Démographique et de santé (EDSB-V). [En ligne]. Disponible sur : |
|
|
Long M (2011). Chronique ONU: La sexualité des adolescents.10(4). [En ligne] Disponible |
|
|
Marston M, Beguy D, Kabiru C, Cleland J (2013). Predictors of sexual debut among young adolescents in Nairobi's informal settlements. International Perspectives on Sexual and Reproductive Health 39(1):22-31. |
|
|
Melaku YA, Berhane Y, Kinsman J, Reda HL (2014). Sexual and reproductive health communication and awareness of contraceptive methods among secondary school female students, northern Ethiopia: a cross-sectional study. BMC Public Health 14(1):1. |
|
|
Ministère de la Santé du Bénin. Direction de la Santé de la Mère et de l'Enfant (2010). Stratégie Nationale Multisectorielle de Santé Sexuelle et de la Reproduction des Adolescents et Jeunes au Bénin 2010-2020. Bénin: MS. p. 48. [En ligne]. Disponible sur: View. |
|
|
Ministère des enseignements secondaire, technique et de la formation professionnelle. Nombre de grossesses en milieu scolaire par département au titre de l'année 2016 - 2017 [En ligne]. Disponible sur: |
|
|
Organisation Mondiale de la Santé (WHO) (2015). La grossesse chez les adolescentes. WHO. [En ligne]. Disponible sur |
|
|
Potard C (2010). Attachement parental, Sexualité à l'adolescence et estime de soi. Psychologie: Tours:Univ Franç - Rabelais; 2010. |
|
|
Stephenson R, Calleen S, Finneran C (2014). Community Factors Shaping Early Age at First Sex among Adolescents in Burkina Faso, Ghana, Malawi, and Uganda. Journal of Health, Population and Nutrition 32(2):161-75. |
|
|
Vallieres EF, Vallerand RJ (1990). Traduction et validation canadienne?française de l'échelle de l'estime de soi de Rosenberg. International Journal of Psychology 25(2) :305-16. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


