ABSTRACT
Malaria in pregnancy is one of the major disease burdens of public health significance in sub-Saharan Africa. Comprehensive preventive strategy including intermittent preventive treatment and effective use of insecticide treated bed nets has been recommended among pregnant women in endemic regions. However the extent to which these preventive strategies are utilized are not fully explored among pregnant women living in controlled environments like the military barracks. This cross-sectional study explored the practices relating to Insecticide-Treated Nets (ITNs) and Intermittent Preventive Treatment using Sulfadoxine Pyrimethamine (IPT-SP) for the prevention of malaria among 420 purposively selected pregnant women from households in Odogbo and Mokola army barracks, Ibadan, Southwest Nigeria. Data were collected using a validated questionnaire, which contained a nine-point knowledge scale. Data were analysed using descriptive and Chi-square statistics. Mean age was 29.3±6.0 years and mean knowledge score was 8.3±1.8. Forty-nine percent of respondents had heard about SP, 17.5% knew the correct dose of IPT-SP, 31.8% had ever used SP and only 10.5% were aware of the stage of pregnancy at which SP should be initiated. Most (92.3%) respondents had heard about ITNs and 76.7% owned one. Almost 60% of respondents prevented malaria with ITNs, 17.8% used insecticide sprays alone, 15.0% used SP while 2.5% used both insecticide sprays and ITNs. Other preventive measures adopted by respondents included environmental control (4.0%) and use of mosquito coils (2.8%). Public enlightenment, advocacy and community mobilization activities are needed in the barracks to improve utilization of malaria prevention strategies among pregnant women.
Key words: Malaria in pregnancy, malaria preventive practices, insecticide treated nets, Sulfadoxine pyrimethamine.
Malaria is a social and medical problem receiving multidisciplinary and multidimensional solution (WHO, 2003) and has been a major public health problem in sub-Saharan Africa. According to Ogbu et al. (2015) prevalence of malaria parasitaemia was 38.8% in a study conducted among asymptomatic women at booking visit in a tertiary hospital, North central Nigeria.
All ages are susceptible but children under 5 years and pregnant women are particularly at risk of severe and complicated malaria. Malaria has remained a major public health problem in Nigeria and it is responsible for 30% childhood and 11% maternal mortality despite the availability of effective interventions. A study showed that 87% of women had undergone at least one episode of malaria during the current pregnancy with 89.0% of them attributing it to bites from infected mosquitoes, while 75% consider malaria an important health risk during pregnancy (Enato et al., 2007a). In Northern part of Nigeria pregnant women and their unborn children have been reported to be vulnerable to malaria which kills children every 30 seconds (Davidson, 2000; Bawa et al., 2014).
The disease burden is especially high among these groups as a result of immature and weakened immunity. Malaria prevention and control program focus on these biologically vulnerable groups particularly those living in poor and hard to reach communities. These communities often have limited access to primary health care as well as to simple and effective preventive tools such as Insecticide Treated Nets (ITNs). In addition, they are less likely to have access to information regarding the disease and how to avoid it (WHO, 2003; Enato et al., 2007a).
Malaria in pregnancy is a common and serious public health problem in Nigeria as large proportion of the asymptomatic pregnant women had malaria parasitaemia with its attendant anaemia (Ogbu et al., 2015). Malarial infestation during pregnancy affects more primigravidae and teenage mothers than those of higher gravidity and older age group. Malaria increases susceptibility to other infections and retard growth and development in children. It is associated with considerable economic burden including direct loss to government productive work or education (Oladepo et al., 2010; Bawa, 2014). Malaria during pregnancy has been associated with increased incidence of anaemia, spontaneous abortions, preterm labour, fetal distress, congenital infections, fetal death in- utero, still births and intrauterine growth restriction (Mutabingwa, 2003).
Despite the evidence that the use of ITNs decreases malaria related mortality and morbidity, its use is still low as reported by the 2013 Demographic Health survey where only 30% of pregnant women in households with ITN slept under Ione the night preceding the interview (NPC & ICF Macro, 2014). Encouragement of consistent and appropriate use of bed-nets has been reported to be a challenge (Cruz et al., 2006). Up to 400,000 infant deaths due to low birth weight could be averted each year if IPT were routinely available to every woman during pregnancy (USAID Health, 2007). According to a study carried out in Southern Nigeria, the prevalence of malaria in pregnancy was 30% and despite the common occurrence of malaria during pregnancy, there was a limited knowledge and use of recommended anti-malarial intervention by women attending antenatal clinics (Enato et al., 2007b).
Many pregnant women who due to poverty and/or lack of education do not go for antenatal care and have no access to preventive malaria care may hence present when the disease is severe. This may lead to abortion, stillbirth, premature delivery, low birth weight babies and/or high mortality for pregnant women. Malaria infection is estimated to cause 400,000 cases of severe maternal anaemia and from 75,000-200,000 infant deaths annually in sub-Saharan Africa (Centre for Disease Control and Prevention, 2007).
According to Abasiatai et al. (2008) in order to prevent the deleterious effects of malaria during pregnancy, intermittent preventive treatment (IPT) of asymptomatic pregnant women, use of insecticide treated bed nets (ITNs) and prompt and effective case management of malaria have been recommended by the World Health Organisation (WHO) as a three pronged approach to the prevention and control of malaria during pregnancy in areas of stable transmission (WHO, 2004).
In the Barracks there is congestion in the accommodation areas and the level of sanitation is quite low, especially in non-commissioned officers’ quarters. The use of Insecticide Treated nets and intermittent preventive treatment to prevent malaria in pregnancy is relatively new in the barracks where they were launched in 2005 and there has not been an effective follow-up to ensure the sustainability of the practice. Also, out-patient records in the Second Mechanized Division Military Hospital in Odogbo Barrack one of the study sites showed that about 12,000 people reported sick from January to October 2007 and 550 had malaria constituting 5.0% of all the patients. From the maternity section of the hospital, out of one hundred and eleven (111) pregnant women that booked between same period 20(18.0%) had malaria related illness. These records showed that pregnant women are at risk of malaria and there is the need to target them for malaria prevention and treatment interventions. The study was therefore carried out to assess the knowledge and practice of malaria prevention in pregnancy among women in the two army barracks in Ibadan, Nigeria.
The study was conducted in two Army Barracks in Ibadan the capital of Oyo State and Nigeria’s third most populous city after Lagos and Kano (NPC, 2006). It is located in south-western
Nigeria. It is an ancient city and a major center for trade in cassava, kolanut, cotton, timber, rubber and palm oil. The growth rate is high and with rapid urbanization which replete with urban slums. This slum poses public health problems. Ibadan’s geographical position and climatic conditions had been favourable to the transmission of malaria. Temperature, humidity, rainfall and attitude affect the transmission of malaria.
A relatively high humidity is required for the survival of adult vector while rainfall is essential in regions lying between latitude 60° north and 40° south. Ibadan falls into the region where malaria is commonly found and it is one of the major causes of mortality and morbidity among children under five years and pregnant women.
Study design and population
The cross-sectional design was used for the study, which involved the collection of self-report information from sample participants with the aim of describing the population based on variables involved. The population for the study consisted of women who were pregnant during the period of study and residing within the Military Barracks in Ibadan. Sample size was calculated using the formula n = Z2pq/d2 yielding a minimum sample of 323 with a prevalence of 30% (Isreal, 1992) but 400 women were recruited so as to account for possible non-response.
Sampling process
Non-probability sampling method (convenience) was used where all pregnant women attending antenatal clinic have opportunity to participate. Other pregnant women who were not attending antenatal clinic were recruited by snowball approach where one pregnant woman was used to link another one giving them equal opportunity to participate.
Instrument for data collection
The instrument used in this study was an interviewer-administered questionnaire. The instrument divided into five sections was designed through review of literature and extracting pertinent variables relating to the prevention practice of malaria in pregnancy. The study instrument was pre-tested in another military barrack in Lagos state.
Data analysis
Administered copies of the questionnaire were edited and hand coded. The data were entered into the computer. An attitudinal score was constructed from the responses. Each correct item was scored on a one-point scale and incorrect items were zero. A 10-point sore was generated and respondents that scored (0-6) points were categorized as negative attitude while those with (7-10) points were categorized as positive attitude. The categorization was based on 50th percentile attitudinal score of 7 points descriptive statistics of frequency counts and percentages were used to describe the attribute of respondents and also inferential statistics of Chi square (x2) were used to test hypothesis at 0.05 alpha level.
Ethical consideration
Ethical approval to conduct the study was sought for and obtained from the Commanding Officer of the intelligent department of the Division, Commander 2 Division Hospital Nigerian Army Ibadan and the Commanding Officer 81 Battalion Nigerian Army Ibadan. Also, the study instrument contained an informed consent clause to respect voluntary participation of the respondents. Confidentiality of the respondents was assured by not writing names or address on the copies of the questionnaire. The right and integrity of the study participants were fully protected. The objectives of the study were explicitly made known to the respondents.
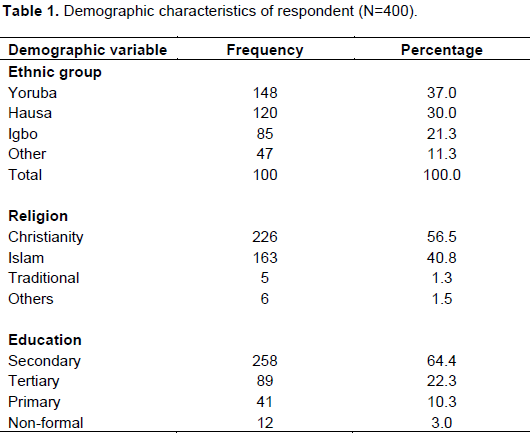
Socio-demographic characteristics of the respondents
Four hundred respondents completed the questionnaire consisting 340 in Odogbo and 60 in Mokola cantonments. The ages of the pregnant women in the two barracks ranged from 17 to 49 years with a mean age of 29.3±6.0 years. A higher number 348(87%) of the respondents were married, while 40(10.0%) were single and 12(3.0%) were divorced. A total of 148(37.0%) were Yorubas, 120(30.0%) were Hausas, 85(21.3%) were Igbos and 47(11.8%) were other ethnic groups such as Igala and Idoma.
Two hundred and twenty six (56.5%) of the respondents were Christians while 163 (40.8%), 5(1.3%) and 6(1.5%) were Moslems, traditional and other religions respectively. Two hundred and fifty eight (64.4%) of them had secondary education and 41(10.3%) had primary education. Two hundred and sixteen (54%) were housewives while 23 (5.8%) were unskilled. However, 163 (40.8%) had two children, 92(23.0%) had three children or more. 90(22.5%) had one child while 53(13.3%) had no child prior to the study (Table 1).
Respondents’ knowledge about malaria
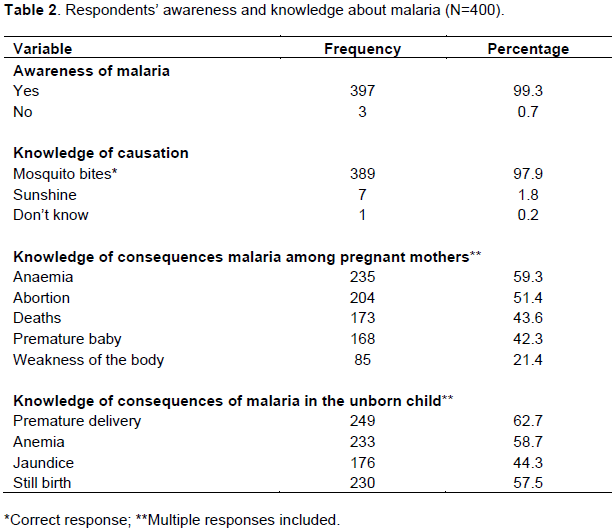
Three hundred and ninety seven (99.3%) of the respondents have heard about malaria before, 384(96%) said they knew the causes of malaria; 389(97.9%) correctly knew that the mosquito bites led to malaria while 7(1.8%) said that the cause of malaria was sunshine and 1 (0.2%) did not know what causes malaria (Table 2). The mean knowledge score of the respondents was 8.3±1.8 of malaria out of 9-point scale.
Respondents’ knowledge about the consequences of malaria to the pregnant woman and unborn child was assessed. Consequences for the pregnant woman known by respondents included anaemia (59.3%) and abortion (51.4%). Consequences to the unborn child included anaemia, (58.7%), and stillbirth (57.5%) (Table 2).
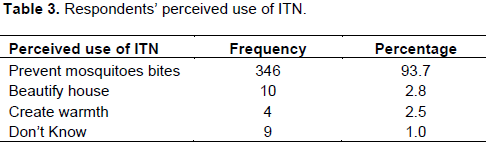
Respondents’ knowledge about preventive measures for malaria
Three hundred and forth-six (93.7%) knew that ITNs are used to prevent mosquito bites. Ten (2.8%) of the respondents believe that ITNs are used to beautify their houses, 4(1.0%) to create warmth while nine (2.5%) did not know what ITN is used for (Table 3).
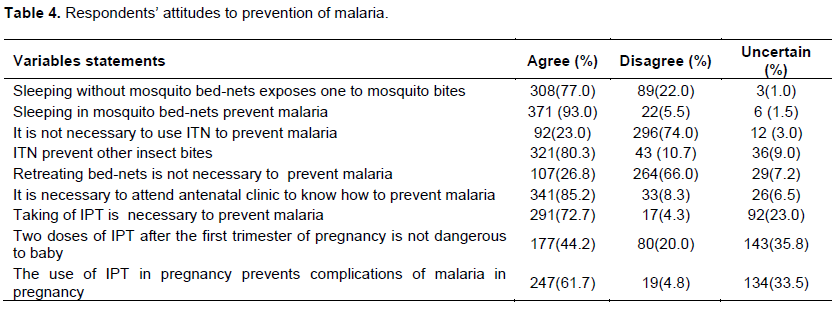
Respondents’ attitudes to prevention of malaria
The respondents’ responses to attitudinal statements are presented in Table 4. Three hundred and eight (77.0%)
respondents agreed that sleeping without mosquito bed-nets exposes one to mosquito bites while 89 (22.0%) disagreed. A good number 371 (92.8%) agreed that it prevents malaria while 22 (5.5%) disagreed. Two hundred and ninety six of them disagreed that it is not necessary to use ITN to prevent malaria while 92(23.0%) agreed. Three hundred and seventy eight (94.5%) agreed that ITN kills mosquitoes and prevents their bites while 15(3.7%) disagreed. Forty-three (10.7%) disagreed that ITN prevents other insect bites while 321(80.3%) agreed and 107 (28.8%) agreed that it is not necessary to retreat ITN with insecticides while 264(66.0%) disagreed.
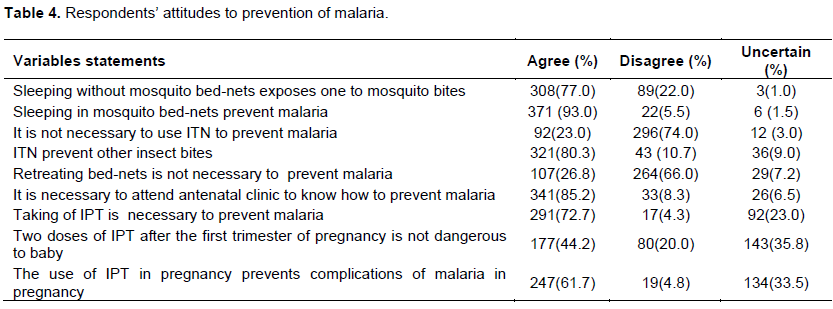
Furthermore 341 (85.2%) agreed that it is necessary to go to antenatal clinic to know how to prevent malaria while 33 (8.3%) disagreed. Two hundred and ninety one (72.7%) agreed that taking of intermittent preventive treatment drug to prevent malaria in pregnancy is necessary while 17 (4.3%) disagreed. One hundred and seventy seven (44.2%) agreed that two doses of IPT is not dangerous to baby while 80(20.0%) disagreed. Two hundred and forty seven (61.7%) agreed that IPT in pregnancy prevents the complications of malaria in pregnancy while 19 (4.8%) disagreed (Table 4). It was observed that (52.5%) of the respondents had positive attitude while the remaining (47.5%) had negative attitude.
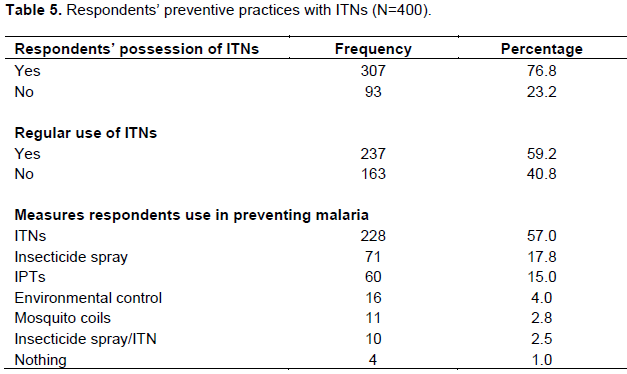
Respondents’ preventive practices with ITNs
Three hundred and eighty eight (97.0%) respondents
said that malaria is preventable, 2 (0.5%) knew it was not while 10 (2.5%) did not know whether malaria is preventable or not. A total of 307 (76.8%) respondents had ITN. A total of 228 (57.0%) of the respondent used ITN as a measure for malaria prevention and 10 respondents out of this number used a combination insecticide spray and ITNs. Two hundred and thirty seven of the respondents (59.2%) used ITN regularly to prevent mosquito bites. Seventy-one (17.8%) of the respondents used insecticide only, while 5(1.3%) did not use anything as a preventive measure (Table 5).
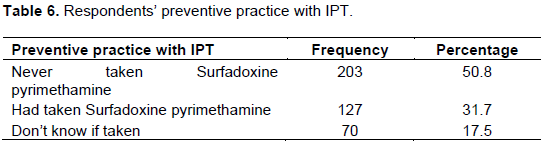
Respondents’ preventive practices with intermittent preventive treatment
One hundred and twenty seven (31.8%) had taken IPT while more than half (50.8%) of the respondents had never taken SP for malaria and 70(17.5%) did not know about IPT before (Table 6). Two hundred and sixty three (65.8%) did not know the number of doses that should be taken in each pregnancy, 70 (17.5%) of them said that two doses should be taken in each pregnancy. Thirty-three (8.3%) respondents said that one dose should be taken, while the same number said that three doses should be taken.
The study showed that there was statistical significance difference between measures of preventing malaria and knowledge of causation of malaria (p=0.16, c2=15.394). The study also showed that there was no statistical difference between knowledge of ITN and its use for prevention of malaria in pregnancy (p=0.550, c2=0.001).
The age distribution of the respondents showed that most of respondents fall within the age of 20 to 29 years, which corresponds with the active reproductive age group for women (Lawson et al., 1991). The majority (87.0%) of them were married which was expected, as pregnancy is usually an outcome of marriage. People marry usually for
procreation. Thirty seven percent of them were Yorubas. This was so as the study was carried out in south-western Nigeria which is predominantly Yorubas.
A majority, (64.4%) attended secondary school and 22.3% tertiary institution. The high number of those who attended secondary is not unconnected with Universal Basic Education (UBE) in Nigeria supported by UNICEF (UNICEF, 2002). Women with formal education were more likely to prevent malaria in pregnancy using ITN and IPT (Gikandi et al., 2008). Most of them were housewives as majority of them were wives of junior non- commissioned officer who are of the lower cadre of soldier of the Nigerian Army.
Knowledge is the key to behavioural antecedent though knowledge alone cannot influence behaviour. In this study, the awareness and knowledge of malaria among the respondents’ was high as 99.3% knew about malaria, and 97.3% of them knew that mosquito bites transmit the parasites which lead to malaria. The knowledge of the causation of malaria in pregnancy was one of the factors that influence prevention of malaria by the respondents.
The respondents knew that malaria has adverse consequences on the pregnant woman which are fever, anemia, weakness, and death. They also knew that the unborn baby is exposed to the risk of prematurity, abortion, and stillbirth and even after birth malaria can give the risk of jaundice. This corresponds therefore with the assertion of the consequences of malaria infection to the mother and baby by Bawa et al. (2014) and Lucas and Gilles (2003) which stated that malaria causes severe maternal anemia, spontaneous abortion, stillbirth, premature delivery (gestation of less than 37 weeks), intrauterine growth retardation and low birth weight increasing rise of infant death. The findings was also similar to those of Abasiattai et al. (2008) at the maternity unit of the University of Uyo Teaching Hospital, Uyo where they determined the degree of awareness and practice of malaria prevention strategies among antenatal attendees in Uyo, South-South Nigeria and found about 71.2% of the respondents knew that malaria had adverse effects in pregnancy.
Respondents’ knowledge of malaria, causes and preventive methods of malaria in pregnancy was high. These had positive effect on the ways the respondents prevent malaria during pregnancy. Their preventive practices of malaria in pregnancy with some preventive methods were also high as majority of them knew that malaria is a preventable disease. They adhered to one or combination of methods for prevention. Majority of the respondents used ITNs to prevent malaria in their homes.
This is probably because malaria including its causes, effects and prevention are often discussed by midwives while giving health talks in the antenatal clinic of the hospital. In addition following the Roll back malaria initiative (RBM) in 1998 and the United Nations Millennium declaration and Abuja declaration in 2000, (FMoH, 2005), there has been a lot of public enlightenment particularly concerning adverse effects of malaria in children and pregnant women (Abasiattai et al., 2008).
CONCLUSION AND RECOMMENDATIONS
The study showed that there was statistical significance difference between measures of preventing malaria and knowledge of causation of malaria. There was also no statistical difference between knowledge of ITN and use to prevent malaria in pregnancy. The study also showed that there was a no statistical difference between knowledge of ITN and use to prevent malaria in pregnancy. Health education of pregnant women on the different methods of preventing malaria in pregnancy during ANC is essential to prevention of malaria in pregnancy.
The study showed that there was statistical significance difference between measures of preventing malaria and knowledge of causation of malaria. There was also no statistical difference between knowledge of ITN and use to prevent malaria in pregnancy. The study also showed that there was a no statistical difference between knowledge of ITN and use to prevent malaria in pregnancy. Health education of pregnant women on the different methods of preventing malaria in pregnancy during ANC is essential to prevention of malaria in pregnancy.
The following recommendations were made based on the findings from the study:
1.There should be sustenance and increased distribution of free insecticide treated nets (ITNs).
2.Involvement of the mass media in community enlightenment programs for improving malaria preventive practices among pregnancy women.
3.Organization of regular training on currents trends in malaria preventive measures for all health staff involved in maternity care are advocated.
The authors have not declared any conflict of interests.
REFERENCES
|
Abasiattai A, Etukumana E, Umoiyoho A (2008). Awareness and Practice of Malaria Prevention Strategies among Pregnant Women in Uyo, South-South Nigeria. Int. J. Gyn. Obstet. 11(1):1-6.
|
|
|
|
Bawa JA, Auta T, Liadi S (2014). Prevalence of Malaria: Knowledge, Attitude and cultural practices of Pregnant Women in Katsina Metropolis, Nigeria. Euro. Sci. J. 10:21.
|
|
|
|
Center for Disease Control and Prevention (2007) Malaria Vector Control. Retrieved 14, September 2007
|
|
|
|
Cruz NDL, Crookston B, Desrden K, Gray B, Ivin N, Alder S, Davis R (2006). Who sleeps under bednets in Ghana? A doer/non-doer analysis of malaria prevention behaviours. Malar. J. 5:61.
Crossref
|
|
|
|
Davidson L, (2000). Malaria. The Horn News paper Nigeria, LT Publication, pp. 11-14.
|
|
|
|
Enato EFO, Okhamafe AO, Okpere EE (2007). A survey of knowledge, attitude and practice of malaria management among pregnant women from two health care facility in Nigeria; Acta Obstet. Gynecol. Scand. 81(1):33-36.
Crossref
|
|
|
|
Enato EFO, Okhamafe AO, Okpere EE, Oseji FI (2007). Prevalence of malaria during pregnancy and anti malaria intervention in urban secondary health care facility in Southern Nigeria: Int. J. Kuwait Univ. Health Sci. Center 3:16.
|
|
|
|
Federal Ministry of Health (2005). National Anti-malarial Treatment Guidelines. Federal Ministry of Health Abuja.
|
|
|
|
Gikandi PW, Noor AM, Gitonga CW, Ajanga AA, Snow RW (2008). Access and barriers to measures targeted to prevent malaria in pregnancy in rural Kenya. Trop. Med. Int. Health 13:2.
Crossref
|
|
|
|
Isreal GD, (1992). Determining Sample Size.
|
|
|
|
Lucas AO, Gilles HM (2003). Short Textbook of Public Health for Tropics. Fourth Edition Bookpower. Malaria and Vector Control Division, Abuja–Nigeria. pp. 192-210.
|
|
|
|
Mutabingwa TK (2003) Treating malaria during pregnancy in Africa. Postgrad. Doc. Africa 25(4):66-73.
|
|
|
|
National Population Commission (NPC) Nigeria and ICF International (2014). Nigeria Demographic and Health Survey 2013. Abuja, Nigeria, and Rockville, Maryland, USA: NPC and ICF International.
|
|
|
|
Ogbu GI, Aimakhu CO, Anzaku SA, Ngwan S, Ogbu DA (2015). Prevalence of malariaparasitaemia among asymptomatic women at booking visit in a tertiary hospital, North Central Nigeria. J. Rep. Biol. Health 3(1):1-7.
Crossref
|
|
|
|
Oladepo O, Tona GO, Oshiname FO, Titiloye MA (2010). Malaria knowledge and agricultural practices that promote mosquito breeding in two rural farming communities in Oyo State, Nigeria. Malar. J. 9:911.
Crossref
|
|
|
|
United Nation International Children Fund (UNICEF) (2002). Procuring supplies for children: The Roll Back Malaria partnership.
|
|
|
|
World Health Organization (WHO) (2003). Lives at risk: malaria in pregnancy.
View
|
|
|
|
World Health Organization (WHO) (2004). A strategic framework for malaria prevention and control during pregnancy in the African region. Brazzaville, World Health Organisation AFR/MAL/04/01.
|