Full Length Research Paper
ABSTRACT
Hepatitis B virus co-infection with Hepatitis C virus and/or Hepatitis D virus is known to result in a more deleterious disease than chronic HBV mono-infection, resulting in faster disease progression to cirrhosis and hepatocellular carcinoma. This study aimed at determining the serological prevalence of Hepatitis C and D virus infections among chronic Hepatitis B virus carriers and the frequency of Hepatitis B e Antigen in a tertiary hospital in South-East, Nigeria. This is a cross-sectional study involving 72 consenting participants who are chronic Hepatitis B virus carriers. Blood samples were collected and serological analysis as well as Hepatitis B virus deoxyribonucleic acid quantification was carried out. The Hepatitis B virus/Hepatitis C virus co-infection rate was observed as 37.5% and Hepatitis B virus/Hepatitis D virus co-infection occurred at a frequency of 2.8%. The Hepatits B viral load and serum alpha fetoprotein levels were observed to have significantly higher median values among the Hepatitis B virus/HCV co-infected participants than among the mono-infected participants (P<0.05). The median Hepatitis B viral load and serum alpha fetoprotein level were also higher among the Hepatitis B virus/Hepatitis D virus co-infected participants than the Hepatitis B mono-infected participants but the difference in viral load was not statistically significant. However, the difference in serum alpha fetoprotein level was observed to be statistically significant. These findings suggest the possibility of a more serious outcome of chronic Hepatitis B virus infection within the study area. Hence, there is need for regular monitoring and aggressive antiviral treatment.
Key words: Hepatitis B virus, hepatitis C virus, hepatitis D virus, hepatitis B e Antigen.
INTRODUCTION
Viral hepatitis is one of the major health issues in recent times. It is the main cause of liver cirrhosis and hepatocellular carcinoma (HCC) in sub-Saharan Africa (Lemoine and Thursz, 2017). The global prevalence of liver cirrhosis is between 4.5 and 9.5% and the annual incidence of HCC is around 5.6% with an annual mortality rate of 2 million deaths per year (Marcellin and Kutala, 2018).
The major risk factors for HCC are viral factors which include Hepatitis B virus (HBV), Hepatitis C virus (HCV) and Hepatitis D virus (HDV), as well as environmental factors such as aflatoxin and iron overload, with more than 50% being attributable to HBV (Mak and Kramvis, 2021). The HBV, HCV and HDV are transmitted through similar routes such as through blood or blood products. So as a result, dual infection and even triple infection can occur in some patients (Liu and Hou, 2006). This frequently occurs in high endemic areas and among people with a high risk for parenteral infections (Tyson et al., 2013).
Infection with these three viruses increases the risk of fulminant hepatitis which is severe necrosis of hepatocytes or severe impairment of hepatic functions (wu et al., 1994). Patients with triple infection of HBV, HCV and HDV suffer from more severe liver lesions. The synergic effects of HBV, HCV and HDV infections can result in more severe liver damage. These patients show a high tendency for liver cirrhosis and they also show increased risk for disease progression to HCC (Crockett and Keeffe, 2005). Treatment in HBV co-infected or tri-infected patients is complex, due to the interaction of the viruses and the potential for reactivation of any of the viruses when antiviral therapy is directed against only one of the viruses (Mavilia and Wu, 2018).
It has been reported severally that Hepatitis B e Antigen (HBeAg) which is a biomarker of active viral replication in hepatocytes, signifies high infectivity and transmission and is also associated with an increased risk of HCC (You et al., 2004). In Nigeria, the presence of HBeAg was always associated with active liver disease, HCC and death (Otegbayo et al., 2003). So, testing for HBeAg in Nigeria can aid in planning patient management and in identifying individuals with a high risk of developing HCC. This can also provide information on the future burden of HCC associated with HBV (Forbi et al., 2012).
This study therefore aimed at determining the burden of HCV and HDV infections among chronic HBV infected patients and the frequency of HBeAg among chronic HBV infected patients in a tertiary hospital located in South-Eastern Nigeria.
MATERIALS AND METHODS
Study design
A total of seventy two participants were recruited by consecutive sampling method from chronic HBV infected patients who accessed care at a tertiary level hospital in South-East Nigeria. They include 39 males and 33 females aged between 20 and 67 years. The sample size (n) was calculated using the formula stated (Daniel, 1999):
n = Z² P (1-P) / d²
where Z = confidence interval of 95% equivalent to confidence coefficient of 1.96, P = prevalence rate in % which is 4.9% (Umeanaeto et al., 2016), and d = desired level of precision or significance (0.05).
This cross-sectional study was carried out between January, 2018 and June, 2019. The consenting participants who met the inclusion criteria were recruited. The inclusion criteria was a diagnosis of chronic hepatitis B virus infection which is defined as HBsAg positivity for more than six (6) months. The patients that are already undergoing treatment and those diagnosed with liver cirrhosis or HCC as well as the pregnant women and the patients that tested positive to Human Immunodeficiency Virus (HIV I & II) antibodies, were excluded from the study so as to eliminate bias.
Ethical issue
An ethical approval with the reference number NAUTH/CS/66/ VOL.10/33/2017/028, was obtained from the Health Research Ethics Committee of the Nnamdi Azikiwe University Teaching Hospital, Nnewi, Anambra State. The study participants signed an informed consent form, and they were duly assured of the confidentiality of the information provided.
Serology
Whole blood samples measuring 5 mL were collected from the participants into plain tubes. The samples were centrifuged at 3000 rpm for 5 min and the serum was separated within 24 h. Serological assays were carried out by testing the serum samples for HBeAg, anti-HBe, HBsAg, anti-HBc and anti-HBs using a lateral flow chromatographic immunoassay (Combo Cassette HBV panel immunoassay manufactured by Lusys laboratories Inc U.S.A) which has a 99.9% sensitivity and 99.75% specificity. The interpretation of test results were performed according to the manufacturer’s specification. An assay was also carried out for HCV antibodies using the SD Bioline immunochromatographic rapid test kit (Standard Diagnostics Inc., Korea). The serum samples were further tested by Enzyme Linked Immunosorbent Assay (ELISA) technique according to the manufacturer’s instruction for anti-HDV IgG ELISA diagnostic kit (Melsin Medical Co., Limited, Jilin Province, China) and serum alpha fetoprotein level using the Accubind ELISA microwells (Monobind Inc., Lake forest, CA, USA).
Quantitative assay of HBV DNA
Hepatitis B virus DNA quantification was done on all the samples using the Cobas AmpliPrep/Cobas TaqMan system (Roche Molecular Systems, Inc., Branchburg, NJ, USA). The assay was performed according to the manufacturer's instruction. The COBAS AmpliPrep/COBAS TaqMan system is a fully automated system consisting of two integrated platforms: the COBAS AmpliPrep for automated nucleic acid extraction from plasma specimens and the COBAS TaqMan, a real-time PCR assay based on TaqMan technology. HBV DNA levels were expressed in IU/mL. The range of quantification is 20 to 170,000,000 IU/mL (1.3 to 8.2 Log IU/mL).
Statistical analysis
The data generated from this study were analyzed using the Stata statistical package, version 16 (Stata statistical software, Stata Corporation, College Station, TX, USA). A skewness/Kurtosis test for normality was done and the data was not normally distributed.
Hence, non parametric tests were employed. The categorical variables were compared using Pearson’s Chi-square or Fisher’s exact test while the median (Interquartile Range, IQR) of continuous variables were compared by Mann-Whitney U- test. A P-value of less than 0.05 was considered as statistically significant.
RESULTS
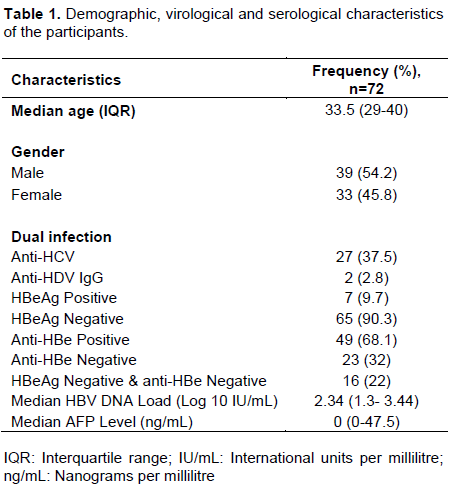
The virological and serological characteristics of the participants are shown in Table 1. The participants had a median age of 33.5 (IQR 29-40) years and were mostly males (54.2%). All the participants were positive to HBsAg and anti-HBc. The HBV/HCV co-infection rate was determined to be 37.5% while the HBV/HDV co-infection rate was 2.8%. There was no participant with HBV/HCV/HDV triple infection.
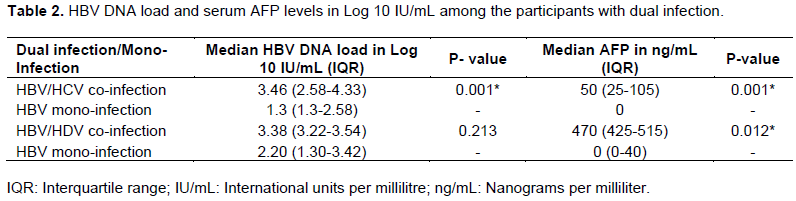
The HBV DNA load and serum AFP levels were observed to differ significantly (P< 0.05 for both) among the HBV/HCV co-infected participants and the HBV mono-infected participants. Higher median values were observed for both parameters among HBV/HCV co-infected participants than the mono-infected participants. The median HBV DNA load and AFP level were also higher among the HBV/HDV co-infected participants than the HBV mono-infected participants but the difference in viral load was not statistically significant (P > 0.05) while the difference in AFP level was observed to be statistically significant (Table 2).
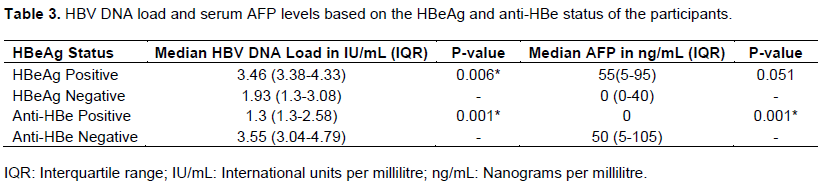
The median HBV DNA load was observed to be higher among the HBeAg positive participants than the HBeAg negative participants and the difference was statistically significant. There was no statistically significant difference between the median AFP levels among HBeAg positive and negative participants. On the other hand, the median HBV DNA load among the anti-HBe positive participants was lower than that of the anti-HBe negative participants and the difference between them was statistically significant (P <0.05) shown in Table 3.
DISCUSSION
The prevalence of HBV/HCV co-infection reported in this study among chronic HBV infected participants is 37.5%. The report of HBV/HCV co-infection from this study was higher than the estimated prevalence of HBV/HCV co-infection among HBsAg positive patients, which has been reported as 5 to 20% (Caccamo et al., 2014). The HCV seroprevalence in Nigeria is known to vary based on the studied population as well as the geographical region (Onyekwere et al., 2016). The report from this study was based on chronic HBV infected patients and this population may have a high chance of contracting HCV, since the two viruses share the same route of transmission which is parenterally (Assih et al., 2018). The high prevalence of HBV/HCV co-infection reported in this study is worrisome and is a great public health concern as HBV/HCV co-infection results in a more severe disease outcome. It has been reported that patients with HBV/HCV co-infection have a higher risk of developing liver cirrhosis and HCC than those with mono-infection of either virus (Huang et al., 2011; Lou et al., 2017). It is crucial that chronic HBV infected patients in South-Eastern Nigeria are tested for HCV infection for the purpose of accurate diagnosis and effective treatment.
Interestingly, a significantly higher median serum AFP level, which is the most widely used biomarker for HCC (Lou et al., 2017) was observed in this study among HBV/HCV co-infected participants than among HBV mono-infected participants (Table 2). High serum AFP level in adults generally indicates a high possibility of HCC in patients with chronic hepatitis or cirrhosis (Zhou et al., 2008). This finding suggests the need for continuous monitoring of patients with HBV/HCV co-infection as they may be at risk of disease progression to HCC.
The evaluation of serum HBV DNA and HCV RNA amounts has revealed that complex virological profiles may be present in co-infected patients. The replication of either virus can be inhibited, just as either virus can be dominant or the dominance can alternate between the two (Marot et al., 2017). It has been reported that a possible competition exists during HBV and HCV co-infection, and the HBV replication is dominant resulting to higher HBV DNA levels (Caccamo et al., 2014). This is in line with the report from this study as the median HBV DNA levels were significantly higher among the HBV/HCV co-infected participants when compared with the HBV mono-infected participants (Table 2). Very limited studies regards HBV DNA levels in mono-infection and co-infection with HCV in South-Eastern Nigeria. The report from this study showing increased HBV DNA replication in co-infected patients is an indication that HBV/HCV co-infection could result to a faster disease progression.
Co-infection of HBV and HCV has also been reported to result in reduced HBV DNA levels and occult HBV infection (Torbenson and Thomas, 2002; Raimondo et al., 2005). A decreased HBV DNA level in HBV/HCV coinfected patients compared to their monoinfected counterparts have been reported (Marot et al., 2017). The reduced HBV DNA level and occult HBV phenomenon were not observed in this study, as all the HBV/HCV co-infected participants also tested positive to HBsAg in addition to significantly higher HBV DNA levels. However, occult HBV infection has previously been reported in South-eastern Nigeria (Nna et al., 2014; Osuji et al., 2018).
The HBV/HDV co-infection rate in this study was observed to be 2.8%. This is lower than 26.2% reported in Pakistan (Rahman et al., 2019), 12.5% reported in South-Eastern, Nigeria (Nwokediuko and Ijeoma, 2009) and 4.9% reported in South-Western Nigeria (Opaleye et al., 2016). Co-infection of HBV and HDV produces a more aggressive disease and faster development of HCC as compared to mono-infection with Hepatitis B (Abbas et al., 2015). The median AFP level of the HBV/HDV co-infected participants in this study was observed to be significantly higher than that of the HBV mono-infected participants (Table 2). This suggests the likelihood of a faster disease progression to HCC among HBV/HDV co-infected participants within the study area and necessitates an early intervention.
There is evidence that co-infection with HDV can result in suppression of HBV replication by HDV with lower levels of HBV viraemia (Williams et al., 2009; Giersch and Dandri, 2015). On the other hand, there are also reports of a fluctuating pattern of HBV and HDV replication over time (Schaper et al., 2010). These issues are conflicting because of different opinions which may be as a result of different geographical locations and viral genotype (Nguyen et al., 2017). The suppression of HBV replication resulting in low HBV DNA levels in HBV/HDV co-infection was not observed in this study. The HDV positive participants had a higher median HBV DNA load than the HBV mono-infected participants but the difference was not statistically significant (Table 2). To our knowledge, there are no reports comparing HBV DNA levels in mono-infection and HBV/HDV co-infection in South-Eastern Nigeria. The implication of a higher HBV DNA load in HBV/HDV co-infection than in HBV mono-infection observed in this study, could be a quicker development of severe liver damage as a result of increased HBV DNA replication..
Several reports have documented that HCV superinfection in the setting of chronic HBV infection can result in HBeAg seroconversion to anti-HBe (Konstantinou and Deutsch, 2015) which is likely due to HBV suppression by HCV. It is worthy to note that the high prevalence of HBV/HCV infection among chronic HBV infected participants in this study occurred with a concomitant high prevalence of anti-HBe shown in Table 1. However, this did not result in HBV suppression as the HBV DNA load was observed to be significantly higher among co-infected participants than in HBV mono-infected participants. This occurrence may be attributed to the presence of HBV precore/core region mutations which have been previously reported (Mbamalu et al., 2021). Hepatitis B virus precore/core region mutations alters or terminates the expression of HBeAg but does not affect the replicative ability of the virus, rather it may result to increased HBV DNA replication (Kramvis, 2008).
The HBeAg is a marker of active viral replication and HBeAg positive patients are highly infective and viremic with often high HBV DNA levels (Kao, 2008). The prevalence of HBeAg in this study was observed to be 9.7% (Table 1) and its presence was marked with a significantly higher HBV DNA level (Table 3). This depicts a high rate of transmission of a vaccine preventable viral infection and is a major public health concern. This report is similar to a previous report from Enugu, South-East, Nigeria where a prevalence rate of 8.6% for HBeAg was reported (Ijoma et al., 2009). The prevalence of HBeAg from this study is also consistent with the report from Lagos, South-West, Nigeria where a prevalence rate of 8.0% was reported (Lesi et al., 2019). The authors also reported a significantly higher detection of HBV DNA load among HBeAg-positive subjects compared with the HBeAg-negative subjects, which agrees with the report from this study. A higher prevalence rate of 19.2% which is not consistent with the report from this study was reported in North-Central, Nigeria (Forbi et al., 2013). Loss of HBeAg is usually associated with the production of anti-HBe (a marker of immune-mediated control) and typically associated with lower viral loads (Tong et al., 2005). This was evident in this study as the prevalence of anti-HBe was observed in this study as 68.1% (Table 1) and its presence was marked with a significantly lower HBV DNA (P<0.05) shown in Table 3.
This study is not without limitations. In addition to serum AFP, other assays that would have provided more information about the extent of hepatological injuries caused by the HBV co-infection with HCV and HDV were not done. Some of these tests include serum alanine aminotransferase (ALT), aspartate aminotransferase (AST), alkaline phosphatase level (ALP), prothrombin time, albumin and total proteins.
CONCLUSION
This study reported a high prevalence of HBV/HCV co-infection in South-Eastern Nigeria where HBV is highly endemic while a very low prevalence of HBV/HDV co-infection was also reported within the study area. The study findings also include HBeAg positivity which was observed to be associated with a higher HBV DNA load, indicating active viral replication and high infectivity. These findings have been shown to be indicators of a faster disease progression to cirrhosis and HCC.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Abbas Z, Abbas M, Abbas S, Shazi L (2015). Hepatitis D and hepatocellular carcinoma. World Journal of Hepatology 7(5):777-786 |
|
|
Assih M, Ouattara AK, Diarra B, Yonli AT, Compaore TR, Obiri-Yeboah D, Djigma FW, Karou S, Simpore J. (2018). Genetic diversity of hepatitis viruses in West-African countries from 1996 to 2018. World Journal of Hepatology 10(11):807-821. |
|
|
Caccamo G, Saffioti F, Raimondo G (2014). Hepatitis B virus and hepatitis C virus dual infection. World Journal of Gastroenterology 20(40):14559-14567. |
|
|
Crockett SD, Keeffe EB (2005). Natural history and treatment of hepatitis B virus and hepatits C virus coinfection. Annals of Clinical Microbiology and Antimicrobials 4(1):1-13. |
|
|
Daniel WW (1999). Biostatistics: a foundation for analysis in the health sciences- 7th Edition. New York: John Wiley and sons. |
|
|
Forbi JC, Ben-Ayed Y, Xia GL, Vaughan G, Drobeniuc J, Switzer WM, Khudyakov YE (2013). Disparate distribution of hepatitis B virus genotypes in four sub-Saharan African countries. Journal of Clinical Virology: the official publication of the Pan American Society for Clinical Virology 58(1):59-66. |
|
|
Forbi JC, Iperepolu OH, Zungwe T, Agwale SM (2012). Prevalence of hepatitis B e antigen in chronic HBV carriers in North-central Nigeria. Journal of Health, Population, and Nutrition 30(4):377-382. |
|
|
Giersch K. Dandri M (2015). Hepatitis B and Delta virus: Advances on studies about interactions between the two viruses and the infected hepatocyte. Journal of Clinical and Translational Hepatology 3(3):220-229. |
|
|
Huang YT, Jen CL, Yang HI, Lee MH, Su J, Lu SN, Iloeje UH, Chen CJ (2011). Lifetime risk and sex difference of hepatocellular carcinoma among patients with chronic hepatitis B and C. Journal of Clinical Oncology: official journal of the American Society of Clinical Oncology 29(27):3643-3650. |
|
|
Ijoma U, Nwokediuko S, Onyenekwe B, Ijoma C (2009). Low Prevalence Of Hepatitis B 'E' Antigen In Asymptomatic Adult Subjects With Hepatitis B Virus Infection In Enugu, South East Nigeria. The Internet Journal of Gastroenterology 10(1):1-5. |
|
|
Kao JH (2008). Diagnosis of hepatitis B virus infection through serological and virological markers. Expert Review of Gastroenterology and Hepatology 2(4):553-562. |
|
|
Konstantinou D, Deutsch M (2015). The spectrum of HBV/HCV coinfection: epidemiology, clinical characteristics, viral interactions and management. Annals of Gastroenterology 28(2):221-228. |
|
|
Kramvis A (2008). Molecular characterization of the genotypes and mutants of hepatitis B virus from South Africa. South African Journal of Epidermiology and Infection 23(1):29-31. |
|
|
Lemoine M, Thursz MR (2017). Battlefield against hepatitis B infection and HCC in Africa. Journal of Hepatology 66(3):645-654. |
|
|
Lesi OA, Audu RA, Okwuraiwe AP, Adeleye OO, Ige FA, Iwuorah JC (2019). Serological and virological markers of nigerian patients with hepatitis B infection. Nigerian Journal of Clinical Practice 22(4):534-538. |
|
|
Liu Z, Hou J (2006). Hepatitis B virus (HBV) and hepatitis C virus (HCV) dual infection. International Journal of Medical Sciences 3(2):57-62. |
|
|
Lou J, Zhang L, Lv S, Zhang C, Jiang S (2017). Biomarkers for Hepatocellular Carcinoma. Biomarkers in Cancer 9:1-9. |
|
|
Mak D, Kramvis A (2021). Epidemiology and aetiology of hepatocellular carcinoma in Sub-Saharan Africa. Hepatoma Research 7:39. |
|
|
Marcellin P, Kutala BK (2018). Liver diseases: A major, neglected global public health problem requiring urgent actions and large-scale screening. Liver International: official Journal of the International Association for the Study of the Liver: 38 Supplement 1:2-6. |
|
|
Marot A, Belaid A, Orlent H, Sersté T, Michielsen P, Colle I, Laleman W, de Galocsy C, Reynaert H, D'Heygere F, Moreno C, Doerig C, Henrion J, Deltenre P (2017). Characteristics of patients with hepatitis B virus and hepatitis C virus dual infection in a Western European country: Comparison with monoinfected patients. Clinics and Research in Hepatology and Gastroenterology 41(6):656-663. |
|
|
Mavilia MG, Wu GY (2018). HBV-HCV Coinfection: Viral Interactions, Management, and Viral Reactivation. Journal of Clinical and Translational Hepatology 6(3):296-305. |
|
|
Mbamalu C, Ekejindu I, Enweani I, Kalu S, Igwe D, Akaeze G (2021). Hepatitis B virus precore/core region mutations and genotypes among hepatitis B virus chronic carriers in South-Eastern, Nigeria. International Journal of Health Sciences (Qassim) 15(2):26-38. |
|
|
Nguyen HM, Sy BT, Trung NT, Hoan NX, Wedemeyer H, Velavan TP, Bock C-T (2017). Prevalence and genotype distribution of hepatitis delta virus among chronic hepatitis B carriers in Central Vietnam. PLoS ONE 12(4):e0175304. |
|
|
Nna E, Mbamalu C, Ekejindu I (2014). Occult hepatitis B viral infection among blood donors in South-Eastern Nigeria. Pathogens and Global Health 108(5):223-228. |
|
|
Nwokediuko SC, Ijeoma U (2009). Seroprevalence of antibody to HDV in Nigerians with hepatitis B virus-related liver diseases. Nigerian Journal of Clinical Practice 12(4):439-442. |
|
|
Onyekwere C A, Ogbera A, Dada A O, Adeleye OO, Dosunmu AO, Akinsegun AA, Osikomaiya B, Hameed O (2016). Hepatitis C Virus (HCV) Prevalence in Special Populations and Associated Risk Factors: A Report From a Tertiary Hospital, Hepatitis Monthly 16(5):e35532. |
|
|
Opaleye OO, Japhet OM, Adewumi OM, Omoruyi EC, Akanbi OA, Oluremi AS, Wang B, Tong H v, Velavan TP, Bock CT (2016): Molecular epidemiology of hepatitis D virus circulating in Southwestern Nigeria. Virology Journal 13:61. |
|
|
Osuji A, Agbakoba NR, Ifeanyichukwu MO, Tatfeng M (2018). Occult Hepatitis B virus infection among blood donors at two teaching hospitals in Nigeria: Implications for blood transfusion. American Journal of Infectious Diseases and Microbiology 6(1):16-25. |
|
|
Otegbayo JA, Fasola FA, Abja A (2003). Prevalence of hepatitis B surface and e antigens, risk factors for viral acquisition and serum transaminase among blood donors in Ibadan, Nigeria. Tropical Gastroenterology: official Journal of the Digestive Diseases Foundation 24(4):196-197. |
|
|
Rahman AS, Amir M, Siddiqui MA, Jamal O, Riaz M, Aziz A (2019). HBV and HDV Seroprevalence Among Healthy People Admitted for Hepatitis B Vaccination. Turkish Journal of Family Medicine and Primary Care 13(1):60-66. |
|
|
Raimondo G, Cacciamo G, Saitta C (2005). Hepatitis B virus and hepatitis C virus co-infection: additive players in chronic liver disease? Annals of Hepatology 4(2):100-106. |
|
|
Schaper M, Rodriguez-Frias F, Jardi R, Tabernero D, Homs M, Ruiz G, Quer J, Esteban R, Buti M (2010). Quantitative longitudinal evaluations of hepatitis delta virus RNA and hepatitis B virus DNA shows a dynamic, complex replicative profile in chronic hepatitis B and D. Journal of Hepatology 52(5):658-664. |
|
|
Tong S, Kim KH, Chante C, Wands J, Li J (2005). Hepatitis B Virus e Antigen Variants. International Journal of Medical Sciences 2(1):2-7. |
|
|
Torbenson M, Thomas DL (2002). Occult hepatitis B. The Lancet. Infectious Diseases 2(8):479-486. |
|
|
Tyson GL, Kramer JR, Duan Z, Davila JA, Richardson PA, El-Serag HB (2013). Prevalence and predictors of hepatitis B virus coinfection in a United States cohort of hepatitis C virus-infected patients. Hepatology (Baltimore, Md.) 58(2):538-545. |
|
|
Umeanaeto PU, Dioji VC, Ifeanyichukwu MO, Onyido AE, Irikannu KC, Okwelogu IS (2016). Malaria and Hepatitis B virus co-infection in Enugwu-ukwu community, Njikoka Local Government Area, Anambra State, Nigeria. Ewemen Journal of Epidemiology and Clinical Medicine 2(1):21-28 |
|
|
Williams V, Brichler S, Radjef N, Lebon P, Goffard A, Hober D, Fagard R, Kremsdorf D, Dény P, Gordien E (2009). Hepatitis delta virus proteins repress hepatitis B virus enhancers and activate the alpha/beta interferon-inducible MxA gene. The Journal of General Virology 90(Pt 11):2759-2767. |
|
|
Wu JC, Chen CL, Hou MC, Chen TZ, Lee SD, Lo KJ (1994). Multiple viral infection as the most common cause of fulminant and subfulminant viral hepatitis in an area endemic for hepatitis B: application and limitations of the polymerase chain reaction. Hepatology (Baltimore, Md.) 19(4):836-840. |
|
|
You SL, Yang HI, Chen CJ (2004). Seropositivity of hepatitis B e antigen and hepatocellular carcinoma. Annals of Medicine 36(3):215-224. |
|
|
Zhou YM, Yang JM, Li B, Yin ZF, Xu F, Wang B, Liu P, Li ZM (2008). Clinicopathologic characteristics of intrahepatic cholangiocarcinoma in patients with positive serum a-fetoprotein. World Journal of gastroenterology 14(14):2251-2254. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


