Full Length Research Paper
ABSTRACT
The aim of this study was to determine the prevalence of herbal medicines (HM) use among diabetic patients in Oriental Morocco, in order to establish an updated inventory of HM consumption and determine the predictive factors of their use in our patients. We conducted a cross-sectional study during three months from March, 2013 to May, 2013 including all diabetic patients consulting at the Department of Endocrinology and Metabolism of Mohammed VI University Hospital in Oujda. The study included 279 diabetics (200 women and 79 men). The prevalence of HM use was 54.8%. Females were 3.25 times more likely to use HM. All patients did not inform spontaneously their physicians about HM use. More than fifty species belonging to 29 families were used by our population. The five most common HM used were Salvia officinalis (Labiaceae), Trigonella feoenum graecum (Leguminosae), Olea europea (Oleaceae), Artemisia herba-alba (Asteraceae) and Origanum vulgare (Lamiaceae). Besides, education level (p = 0.027), menopause (p = 0.027), type 2 diabetes (p = 0.05) and taking both oral hypoglycaemic agents and insulin injection (p = 0.043) are significant factors associated with HM use. HM is very common among diabetic patients. There is an urgent need for health education regarding the use of herbs in conjunction with conventional medicines. Clinical and randomized trials may be needed in the future to assess the efficacy and the safety of the reported herbs.
Key words: Herbal medicines, medicinal plants, phytotherapy, diabetes, Morocco, complementary and alternative medicine.
INTRODUCTION
Diabetes mellitus is one of the major public health concerns. Data from the International Diabetes Federation (IDF) indicate that there are 382 million diabetics all over the world and in the next 20 years, diabetes may affect about five times more people than it does now. Moreover, diabetes caused 5.1 million deaths in 2013. Epidemiological data show that 80% of people with diabetes live in low- and middle-income countries. In Africa, there are more than 19 million patients with diabetes (International Diabetes Federation, IDF, 2012).
Since ancient time, patients with particularly chronic diseases such as diabetes mellitus use traditional medicine and often without consulting or even were informing their physicians. According to the World Health Organization, traditional medicine, referred to complementary and alternative medicine (CAM) in some countries, covers a wide variety of therapies and practices including the use of herbal medicines (HM). Even if traditional medicine is mostly used by developing countries where a large number of people have poor access to modern health care systems, it is recognized now that the use of CAM is increasing and is observed in both developed and developing countries (WHO, 2014). Population-based studies in many developed countries such as Australia (MacLennan et al., 1996), United Kingdom (Emslie et al., 1996), Taiwan (Lew-Ting, 2003), Singapore (Lim et al., 2005), Canada (McFarland et al., 2002) and the United States of America (Tindle et al., 2005) report that one-half to two-thirds of adults use CAM.
Morocco is characterized by a large diversity of biotopes allowing a rich flora with about 4,200 species of which more than 600 are described in the Moroccan pharmacopeia (Bellakhdar et al., 1991). Many ethno-pharmacological surveys were conducted in various regions of Morocco (center, south and oriental) so as to identify species of HM used by patients or counseled by the herbalists in chronic diseases such as diabetes, hypertension, cardiac diseases (Ziyyat et al., 1997; Jouad et al., 2001; Eddouks et al., 2002) and cancer (Kabbaj et al., 2012). However, none of them determined the related factors to the use of HM in diabetic patients.
The objecttives of the current study were to determine the prevalence of HM use among diabetic patients in Oujda, the largest city of Oriental Morocco, to establish an updated inventory of the used plants and to identify the factors predicting HM use.
MATERIALS AND METHODS
Study design
We carried out a cross-sectional study during three months from March, 2013 to May, 2013 at Mohammed VI University Hospital in Oujda. Each diabetic patient who consulted at the Department of Endocrinology and Metabolism was asked to participate into the study. All patients were informed of the aims of the study and gave their consent.
Data collection
A face-to-face interview was conducted using a semi-structured questionnaire to obtain data including:
1. Data on patient: age, sex, weight, province region (rural or urban), medical insurance, education level (no education, primary, secondary or higher), diabetes type, its duration and treatment.
2. Information on HM use, use duration, the vernacular name, the used part, preparation method, use frequency, use resources, the reason of its use and side effects related to its use. .
The following references were used to identify the vernacular name and then to match it to the scientific name and the family to which they belong: (Hmamouchi, 2001; Bellakhdar et al., 1991)
Statistical analysis
Statistical analysis of data was performed using the IBM SPSS Statistics Standard version 21.0. Descriptive data were expressed using means, medians, standard deviations and percentages. Categorical data were compared using chi-square test c2. Statistical significance was defined as p < 0.05.
RESULTS
Socio-demographic and clinical characteristics
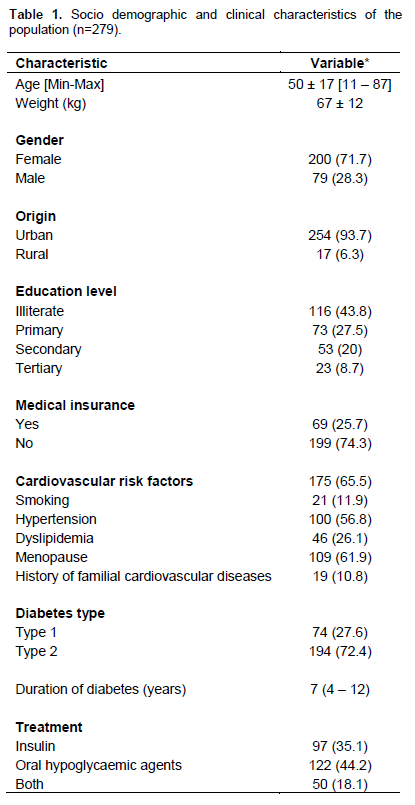
The study included 279 diabetic patients (200 women and 79 men) with a mean age of 50 ± 17 years and a mean weight of 67 ± 12 kg. Most of them came from urban regions (93.7%), had no education (43.8%) or studied at a primary level (27.5%) and had no medical insurance (74.3%). Type 2 diabetes was more common in our population than type 1 (72.4% vs. 27.6%) with a median duration of 7 years [4 – 12]. Sixty five percent of patients had at least one cardiovascular risk factor. The main risk factors in our population were menopause followed by hypertension. Table 1 shows socio-demographic and clinical characteristics of our patients.
Prevalence and resources on HM use
The prevalence of HM use was 54.8%. Females used HM 3.25 times more likely than males. None of our patients disclosed HM use spontaneously to their physician. More than ninety percent of HM users (93.8%) reported HM usage for more than a month. The frequency of consumption of HM was everyday for 51.2% and once a week for 28.1%. Most patients learned about HM use primarily from friends, neighbors and families (84.8%), followed by media (radio in 9% and television in 5.5%). The majority of patients (80%) got HM from the herbalists and 17% of them directly from nature. Few patients (8%) reported gastro-intestinal effects while 91.7% had no side effects.
Patterns, attitudes, beliefs, and perceptions toward HM
Most HM users (81.1%) believed that HM can potentiate the effect of the drug medicines and can help them achieve better control in diabetes while only 7% of them used HM because they think that medicines are not effective as they must be. Some use HM (4.9%) because they do not have any confidence in medicines (Table 2).
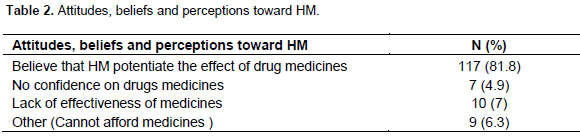
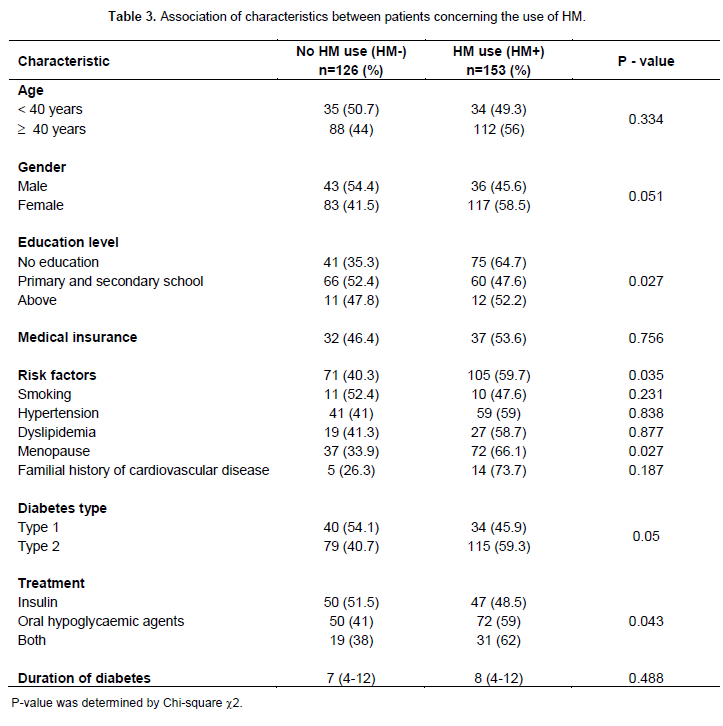
Table 3 provides a comparison of characteristics between HM users (HM +) and no users (HM-). Patients with cardiovascular risk factors use HM more than patients who do no’t (p = 0.035). Menopause seems to be a significant risk factor associated to HM use (p = 0.027).
We observed that patients with type 2 diabetes used HM (59.3%) more than patients with type 1 diabetes (45.9%), although this is not statistically significant (p = 0.05). Duration of diabetes did not differ between HM+ and HM- (p=0.48). Most HM users were treated by the combination of hypoglycaemic agents and insulin injection (p = 0.043). We also observed that the majority of patients treated only by insulin did not use HM (51.1%).
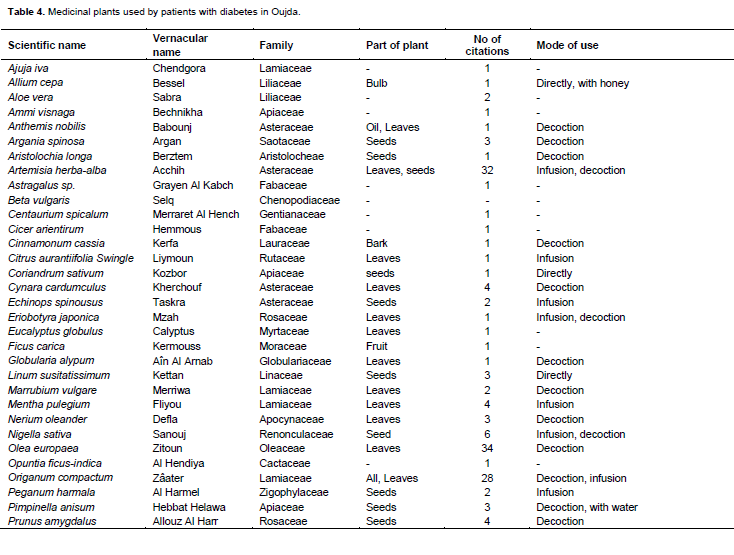
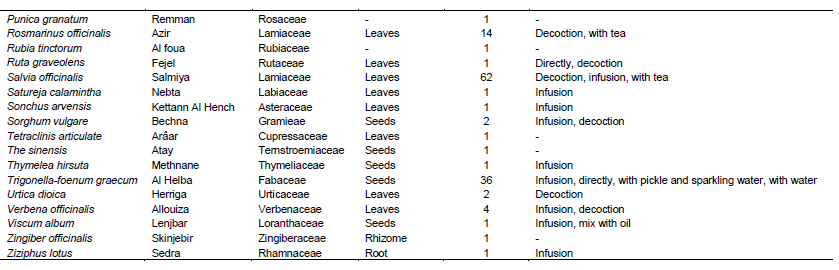
Inventory of plant species used by diabetic patients
In 60% of cases, a mixture of plants was used. More than fifty plant species belonging to 32 families were used by our population, of which the five most used were: Salvia officinalis (62 citations), Trigonella feoenum-graecum (36 citations), Olea europea (34 citations), Artemisia herba -alba (32 citations) and Origanum vulgare (28 citations). An inventory of the 49 plants identified and used is given in Table 4 with the vernacular name, family name, part used, mode of use and number of citations.
DISCUSSION
The prevalence of HM use among diabetic patients in this study population was high (54.8%). The use of medicinal plants for diabetes treatment is reported worldwide. It is also a national widespread practice. However, this result is lower when compared to that of other national previous studies undertaken by Ziyyat et al. (1997) in the same region (67.5%) and in other regions of Morocco such as Fez-bouleman (76%) (Jouad et al., 2001) and Tafilalet (80%) (Eddouks et al., 2002). A large access to medicines and progressive awareness of population over the years may explain this finding. Another possible reason for the differences in the rate of HM use between these studies may be attributed to differences in the research methodology used. This prevalence remains higher in comparison to other Arabic countries such as Palestine, Jordan, Saudi Arabia, and Kuwait (Ali-Shtayeh et al., 2012; Otoom et al., 2006; Wazaify et al., 2011; Al-Rowais, 2002; Awad et al., 2008) where the following prevalence’s were recorded: 51.9, 31, 16.6 to 17.4 and 13%. In Turkey, 41% of diabetic patients used at least one of CAM practices (Ceylan et al., 2009).
Females used HM more likely than males (58.5% vs. 45.6%), though not significant (p = 0.05). This is consistent with findings in other studies (Ziyyat et al., 1997; Jouad et al., 2001; Eddouks et al., 2002) and could be explained by the attachment of women in our country to traditional medicine. It may be also linked to the fact and that they stay more often at home as most of them are housewives.
Education level influences HM use (p = 0.027) whereas holding a medical insurance did not (p = 0.57). In fact, most HM+ were illiterate (64.7%) in comparison to HM- (35.3%). This is in contrast with the results of an Indian survey where higher levels of education and socio-economic status were significant positive correlates of CAM use (Kumar D et al., 2006). All patients practicing CAM used HM alongside allopathic treatment with a significant result with patients treated by both oral hypoglycaemic agents and insulin injection (p = 0.043). One possible reason for our findings is that patients with diabetes had poor blood-sugar control, as the conventional treatment requires them to be disciplined with respect to diet, lifestyle and behavior. So patients use HM to potentiate the anti-diabetic activity of the allopathic treatment and thus contribute to the management of their disease. In addition, 51% of patients with insulin therapy do not use HM. To explain this, patients at the stage of insulin therapy received improved diabetes education counseling. An alarming result is that none of our patients (100%) did inform us spontaneously about HM use.
Similar studies conducted in among Jordanian (Wazaify et al., 2011)[, Sudanian (Al-Rowais, 2002) and Palestinian patients (Ali-Shtayeh et al., 2012) have showed that respectively 84.3, 70 and 68% of patients did not tell their physicians or pharmacists about HM use. This result indicates that patients are not aware of the dangers that may occur when herbs are used in conjunction with medicines. The combination of herbal remedies and medical prescriptions may lead to ineffective diabetic management and adverse effects (Chavez et al., 2006)[101]. It is therefore important that patients disclose HM use to their health care professionals and physicians. This information about CAM usage should be incorporated into clinical practice and sought after by clinicians.
The most common sources of HM information were recommendation from friends, neighbors and families, followed by media. This finding highlights the importance of the patients close environment (friends, neighbors, family) in decision-making processes and health beha-viors. So, health professionals should be aware of the impact of their beliefs and attitudes on the beliefs and attitudes of their patients. The present study indicates that we must involve patients’ families during diabetes education counseling regarding the efficacy and potential side-effects of plants . In addition, health authorities should monitor advertising on radio and television by choosing qualified experts in the field to make advice to the population.
The majority of plants used by patients was purchased locally. This highlights that plants are easy to access, available and cheap. In most cases (60%), patients did not use one plant but a mixture of plants. The reported number of herbs used by patients with diabetes in this work was about fifty species. This is slightly higher than the same study that was done earlier by Ziyyat et al. (Ziyyat et al., 1997) in Oriental Morocco (41 species) but considerably higher than that reported in Jordan (Wazaify et al., 2011) (12 species) and lower than a Palestinian study which reports (100 species) (Ali-Shtayeh et al., 2012).
The most commonly used herbs by our population included officinalis (Labiaceae), feoenum-graecum (Leguminosae), Olea. europea (Oleaceae), . herba-alba (Asteraceae) and vulgare (Labiaceae). Anti-diabetic activity has been demonstrated on diabetic animal models for . foenum-graecum (Xue et al., 2007) and europea (Kaeidi et al., 2011). Many researchers have studied the hypoglycaemic effect of hydro-alcoholic extracts of herba-alba and confirmed the possibility of its use in the treatment of type 2 diabetes (Hamza et al., 2011) as well as in prevention (Hamza et al., 2010). [167]. Furthermore, some studies have suggested that the methanolic and the water ethanolic extracts of officinalis leaves have hypoglycaemic effects in Streptozotocin- and alloxan-induced diabetic animals without changes in insulin level (Eidi et al., 2005; Alarcon-Aguilar et al., 2002). In addition, the essential oil of sage has been tested and has proved its hypoglycaemic effect in normal and in alloxan-induced diabetic rats (Moradabadi et al., 2013) but not in streptozotocin-induced diabetic rats (Awad et al., 2008; Lima et al.. 2006) observed a metformin-like effect of infusion of S. officinalis on rat hepatocytes that may be useful as a food supplement in the prevention of type 2 diabetes by lowering the plasma glucose of individuals at risk. (Lemhadri et al., 2004) have shown that the aqueous extract of vulgare, commonly named “zaâtar” and growing wild in Tafilalet region of Morocco has an anti-hyperglycaemic activity in Streptozotocin-rats without affecting basal plasma insulin concentrations. Therefore, these studies provide a scientific basis to conduct clinical and randomized trials to assess the efficacy and the safety of these plants in humans.
However, there was a report of the use of Aristolochia longa by one patient. longa is commonly used in traditional medicine (Bellakhdar et al, 1991). In 2001, Food and Drug Administration (FDA) published an alert about the safety of aristolochic acid, the active ingredient of . longa (Food and Drug Administration (FDA), 2014). In 2002, the International Agency for Research on Cancer has classified products containing aristolochia species as a human carcinogen (IARC, 2002). Aristolochic acid, is recognized to cause aristolochic acid nephropathy associated with a high long-term risk for renal failure and urothelial cancer (Al-Rowais, 2002; Zhou et al., 2010; Arlt VM et al., 2002) by DNA adduct formation (Allard et al., 2013). From this scientific evidence-base, aristolochic acid-containing herbs should be banned in our country by health authorities as it is the case in many countries.
LIMITATIONS OF THE STUDY
The present study has several limitations. Firstly, the survey was carried out on patients attending the Department of Endocrinology and metabolism of a University Teaching hospital for treatment of diabetes and hence does not reflect the common practices in the general population. Secondly, we were unable to assess objectively and scientifically harmful or beneficial effects associated with HM use.
CONCLUSION
HM use among patients with diabetes mellitus in Oriental Morocco is very common. Menopausic and illiterate women, with type 2 diabetes under both oral hypoglycaemic agents and insulin as a conventional treatment have a higher likelihood of HM use. Physicians should seek and discuss with their patients during diabetes education counseling the use of HM, their potential interactions and side-effects when used in conjunction with medicines.
CONFLICT OF INTEREST
There is no conflict of interest to declare.
REFERENCES
|
Alarcon-Aguilar FJ, Roman-Ramos R, Flores-Saenz JL, Aguirre-Garcia F (2002). Investigation on the hypoglycaemic effects of extracts of four Mexican medicial plants in normal and alloxan-diabeti mice. Phyto. Res. 16(4):383-386. Crossref |
||||
|
Ali-Shtayeh MS, Jamous RM, Jamous RM (2012). Complementary and alternative medicine use amongst Palestinian diabetic patients. Complement. Ther. Clin. Pract. 18(1):16-21. Crossref |
||||
|
Allard T, Wenner T, Greten HJ, Efferth T (2013). Mechanisms of herb-induced nephrotoxicity. Curr. Med. Chem. 20:2812-9. Crossref |
||||
|
Al-Rowais NA (2002). Herbal medicine in the treatment of diabetes mellitus. Saudi Med. J. 23:1327-31. Pubmed |
||||
|
Arlt VM, Stiborova M, Schmeiser HH (2002). Aristolochic acid as a probable human cancer hazard in herbal remedies: a review. Mutagenesis 17:265-277. Crossref |
||||
|
Awad A, Al-Rabiy S, Abahussain E (2008). Self-medication practices among diabetic patients in Kuwait. Med. Princ. Pract. 17(4):315-20. Crossref |
||||
| Baricevic D, Bartol T (2000). The biological/ pharmacological activity of the Salvia genus. In Sage-the Genus Salvia, [SE Kintzios, editor]. Amsterdam: Harwood Academic publishers. pp. 143-184. | ||||
|
Bellakhdar J, Claisse R, Fleurentin J, Younos C (1991). Repertory of standard herbal drugs in the Moroccan pharmacopoea. J. Ethnopharmacol. 35:123-143. Crossref |
||||
|
Ceylan S, Azal O, Taslipinar A, Türker T, Açikel CH, Gulec M (2009). Complementary and alternative medicine use among Turkish diabetes patients. Compl. Ther. Med. 17:78-83. Crossref |
||||
|
Chavez ML, Jordan MA, Chavez PI (2006). Evidence-based drug-herbal interactions. Life Sci. 78:2146-57. Crossref |
||||
|
Eddouks M, Maghrani M, Lemhadri A, Ouahidi ML, Jouad H (2002). Ethnopharmacological survey of medicinal plants used for the treatment of diabetes mellitus, hypertension and cardiac diseases in the south-east region of Morocco (Taï¬lalet). J. Ethnopharmacol. 82:97-103. Crossref |
||||
|
Eidi M, Eidi A, Zamanizadeh H (2005). Effect of Salvia officinalis L. leaves on serum glucose and insulin in healthy and streptozotocin-induced diabetic rats. J. Ethnopharmacol. 100:310-313. Crossref |
||||
|
Emslie M, Campbell M, Walker K (1996). Complementary therapies in a local healthcare setting Part 1. Is there real public demand? Complement Ther. Med. 4:39-42. Crossref |
||||
| Food and Drug Administration. Dietary supplements: aristolochic acid. http://www.fda.gov/Food/RecallsOutbreaksEmergencies/SafetyAlertsAdvisories/ucm096388.htm . Accessed on May 28th, 2014. | ||||
|
Hamza N, Berke B, Cheze C, Le Garrec R, Lassalle R, Agli AN, Robinson P, Gin H, Moore N (2011). Treatment of high fat diet induced type 2 diabetes in C57BL/6J mice by two medicinal plants used in traditional treatment of diabetes in the east of Algeria. J. Ethnopharmacol. 133:931-933. Crossref |
||||
|
Hamza N, Berke B, Cheze C, Agli AN, Robinson P, Gin H, Moore N (2010). Prevention of type 2 diabetes induced by high fat diet in the C57BL/6J mouse by two medicinal plants used in traditional treatment of diabetes in the east of Algeria. J. Ethnopharmacol. 128:513-518. Crossref |
||||
| Hmamouchi M. Plantes médicinales et aromatiques du Maroc.2nd Edition, 2001. IARC monographs on the evaluation of carcinogenic risk of chemicals to humans. Volume 82. Lyons, France: IARC Press, 2002.Some traditional herbal medicines, some mycotoxins, naphthalene and styrene. International Diabetes Federation, IDF, Diabetes Atlas. 6th Ed.: International Diabetes Federation; 2012. | ||||
|
Jouad H, Haloui M, Rhiouani H, El Hilaly J, Eddouks M (2001). Ethnobotanical survey of medicinal plants used for the treatment of diabetes, cardiac and renal diseases in the North centre region of Morocco (Fez–Boulemane). J. Ethnopharmacol. 77:175-182. Crossref |
||||
| Kabbaj F, Meddah B, Cherrah Y, Faouzi A (2012). Ethnopharmacological profile of traditional plants used in Morocco by cancer patients as herbal therapeutics. Phytopharmacology. 2:243-256. | ||||
|
Kaeidi A, Esmaeili-Mahani S, Sheibani V Abbasnejad M, Rasoulian B, Hajializadeh Z, Afrazi S (2011). Olive (Olea europea L.) leaf extract attenuates early diabetic neuropathic patin through prevention of high glucose-induced apoptosis : in vitro and in vivo studies. J. Ethnopharmacol. 136:188-196. Crossref |
||||
|
Kumar D, Bajaj S, Mehrotra R (2006). Knowledge, attitude and practice of complementary and alternative medicines for diabetes. Public Health.120:705-711. Crossref |
||||
|
Lemhadri A, Zeqqwagh A, Maghrani M, Jouad H, Eddouks M (2004). Anti-hyperglycaemic activity of the aqueous extract of Origanum vulgare growing winld in Tafilalet region. J. Ethnopharmacol. 92:251-256. Crossref |
||||
| Lew-Ting CY (2003). Who uses non-biomedical, complement and alternative health care? Sociodemographic undifferentiation and the effects of health needs. Taiwan J. Public Health. 22:155-66. | ||||
|
Lima CF, Azevedo MF, Araujo R, Fernandes-Ferreira M, Pereira-Wilson C (2006). Metformin-like effect of Salvia officinalis (common sage): is it useful in diabetes prevention? Br. J. Nutr. 96:326-33. Crossref |
||||
|
Lim MK, Sadarangani P, Chan HL, Heng JY (2005). Complementary and alternative medicine use in multiracial Singapore. Complementery Ther. Med. 13:16-24. Crossref |
||||
|
MacLennan AH, Wilson DH, Taylor AW (1996). Prevalence and cost of alternative medicine in Australia. Lancet 347:569-573. Crossref |
||||
|
McFarland B, Bigelow D, Zani B, Newsom J, Kaplan M (2002). Complementary and alternative medicine use in Canada and the United States. Am. J. Public Health. 92:1616-1618. Crossref |
||||
|
Moradabadi L, Montasser Kouhsari S, Fehresti Sani M (2013). Hypoglycemic Effects of Three Medicinal Plants in Experimental Diabetes: Inhibition of Rat Intestinal α-glucosidase and Enhanced Pancreatic Insulin and Cardiac Glut-4 mRNAs Expression. Iran J. Pharm. Res.12:387-397. Pubmed |
||||
|
Otoom SA, Al-Safi SA, Kerem ZK, Alkofahi A (2006). The use of medicinal herbs by diabetic Jordanian patients. J. Herb Pharmacother. 6:31-41. Crossref |
||||
| Tindle HA, Davis RB, Phillips RS, Eisenberg DM (2005). Trends in use of complementary and alternative medicine by US adults: 1997-2002. Altern Ther Health Med. 13:16-24. | ||||
|
Wazaify M, FU. Afifi, M El-Khateeb, Ajlouni K (2011). Complementary and alternative medicine use among Jordanian patients with diabetes. Complementary Ther. Clin. Pract. 17:71-75. Crossref |
||||
| World Health Organization (WHO). http://www.who.int/topics/traditional_medicine/en/. Accessed on March 16, 2014. | ||||
|
Xue WL, Li XS, Zhang J, Lliu YH, Wang ZL, Rui-Juan Zhang RJ (2007). Effect of Trigonella foenum-graecum (Fenugreek) extract on blood glucose, blood lipid and hemorheological properties in streptozocin-induced diabetic rats. Asia Pac. J. Clin. Nutr. 16 (Suppl 1):422-426. Pubmed |
||||
|
Zhou L, Fu P, Huang XR, Liu F, Chung AC, Lai KN, Lan HY (2010). Mechanism of chronic aristolochic acid nephropathy: role of Smad3. Am. J. Phys. Renal Physiol. 298:F1006-17. Crossref |
||||
|
Ziyyat A, Legssyer A, Mekhfi H, Dassouli A, Serhrouchni M, Benjelloun W (1997). Phytotherapy of hypertension and diabetes in oriental Morocco. J. Ethnopharmacol. 58:45-54. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


