Full Length Research Paper
ABSTRACT
This study evaluated the prevalence of Surgical Site Infections (SSIs), the enhancing risk factors in small animal hospitals and clinics, and clinicians’ perception of SSIs in South-west, Nigeria. Ten years (2007-2017) surgical patients’ case records from four government veterinary hospitals were initially studied. Fifty-seven copies of structured pre-tested questionnaires were further administered to practice representatives in government and private small animal facilities in 6 states of South-West, Nigeria. Data were analyzed with descriptive statistics and Pearson Chi-square at 95% confidence intervals. One hundred and twenty-six out of 584 small animal surgical patients satisfied the inclusion criteria. Eight (6.3%) cases from the case records had SSIs. Fifty out of 57 retrieved questionnaires satisfied the inclusion criteria for analysis. Sixty-four percent of respondents had the Doctor of Veterinary Medicine (DVM) degree while 36% had additional degrees. The majority (64%) of respondents had 1 to 3 years practice experience with the rest having above 3 years. Most of the respondents (96%) had good knowledge of SSI, 78.7% usually manage SSI cases and 18% had lost patients due to SSIs. Only 48% of the practices perform surgery in designated operating rooms. The environment (94%), hands of clinicians/caregiver (80%) and patients’ skin (62%) were the main sources of SSIs in respondents’ practice. Few respondents (19.1%) administer prophylactic antibiotics for all surgeries, 6.1% discontinue within 24 h post-surgery, while 75.5% continue antibiotic therapy for 3 to 7 days post-surgery. Lack of facilities (40%) and funds (54%) prevented some clinicians from keeping up with SSIs prevention measures. There was an association between the risk factors of post-operative wound dehiscence (P=0.006), classification of the surgical procedures (P=0.032) and SSI occurrence. Although many small animal practitioners are aware of SSIs risk factors, only few adhere to prevention protocols.
Key words: Surgical site infection (SSI), risk factors, small animal clinicians, perception.
INTRODUCTION
Surgical site infections (SSIs) are surgery associated nosocomial infections with multifactorial aetiologies (Eyarefe, 2016). They are defined as infections occurring at the surgical site within 30 days post-surgery or within one year of fixing an implant (Berríos-Torres et al., 2017). SSI is a common nosocomial infection in human patient populations, accounting for 38% of nosocomial infections among surgical patients in the United States (Mangram et al., 1999a, b). SSI is a growing concern in veterinary practice. It accounts for 0.8 to 18% of nosocomial infections among small animal surgery patients (McMillan, 2014; Verwilghen and Singh, 2015) and 1 to 50% among equine surgery patients depending on surgical procedure and wound classification (Ahern and Richardson, 2012). It has also been associated with development of multidrug-resistant pathogens due to antibiotic abuse (Akinrinmade and Oke, 2012; Windahl et al., 2015).
The multifactorial aetiology of SSIs is linked with poor surgery theatre environment, operating techniques, surgery team attitude, as well as poor instrument and patient preparation (Eyarefe, 2016). SSI causes increased patient morbidity, affects the success of initial surgical intervention, delays healing, and results in additional costs for the animal owners (Verwilghen, 2015; Birgand et al., 2014). SSI problem is legendary and dates back to the very beginning of practice of the surgery specialty (Clark, 1907). Earlier infection control measures were implemented following Drs. Ignaz Semmelweis and Oliver Wendell Homes’ observations that contaminated hands of attending physicians served as vehicles for the spread of infections (Humes and Lobo, 2005; Adriaanse et al., 2000). The introduction of compulsory hand scrubbing with chlorinated lime solution before physical examination by attending physicians resulted in an impressive reduction in mortality rate (from 11.4 to 1.3% within two years) in the Vienna maternity ward (Adriaanse et al., 2000; Sabbatani et al., 2014), and propelled the commencement of compulsory antiseptics hand washing regimen as a means of infection control among surgeons (Humes and Lobo, 2005; McMillan, 2014).
This practice became globally accepted following the publication of the Louis Pasteur germ theory of disease in 1860, on the role of germs in infection causation, and a suggestion that instead of killing the microbes in wounds, it would be more reasonable to prevent them (Verwilghen et al., 2013; Ahern and Richardson, 2012). Infection control practice further became entrenched among communities of surgeons with Joseph Lister‘s publications on anti-septic surgery concept and thesis on aseptic principles for surgeons (Hemani and Lepor, 2009). The discovery of antibiotics further enhanced the curbing of SSIs. However, the current global trend in microbial multi-drug resistance poses a major challenge and calls for a strict adherence of SSI risk factors prevention and control strategies.
So far, fewer studies have investigated incidence of post-surgical infections in small and large animals, possible risk factors and veterinary clinicians’ perception of SSIs (Verwilghen and Singh, 2015; Windahl et al., 2015). Since SSI eradication is difficult, prevention strategies represent the most economical, logical and effective means of reducing its impact (Windahl et al., 2015).
In Nigeria, SSI poses a major patient post-surgery health challenge (Eyarefe, 2016). Although SSI cases are prevalent in small animal practice in Nigeria with attendant morbidity and mortality, little concern is raised, and intervention strategies are underestimated due to lack of data on prevalence, clinicians’ perception and enhancing risk factors.
This study was therefore designed to evaluate the SSI risk factors in selected veterinary hospitals and clinics, and assess small animal clinicians’ awareness of SSIs in the southwest states of Nigeria, with the objective of generating empirical data for planning SSI prevention strategies.
MATERIALS AND METHODS
Study of patients’ case records and identification of SSI risk factors
Ten years (June 2007 to June 2017) case records of surgical patients presented at two Veterinary Teaching Hospitals (VTH, UI; VTH, FUNAAB), Oyo State Veterinary Hospital Mokola, Ibadan and Ondo State Veterinary Hospital, Akure were studied. Canine patients (dogs) with postoperative follow-up records between 7 and 30 days were enrolled. SSI risk factors were identified from patients’ case records through evaluation of patient demographic characteristics and operation characteristics (anaesthetic protocol, use of implants, perioperative antimicrobial prophylaxis, and post-operative wound dehiscence) as previously described (Owens et al., 1978; Culver et al., 1991; Imai et al., 2005; Kaye et al., 2005). SSI cases were identified by fulfillment of inclusion/eligibility criteria as stated by Centre for Disease Control and Prevention/National Nosocomial Infection Surveillance (CDC/NNIS, 2017 ). These included purulent drainage from the deep incision or from a drain placed at surgical site; evidence of wound dehiscence with concurrent signs of fever; localized pain or tenderness; presence of abscess following surgery and histopathologic or radiographic evidence of SSIs as identified/diagnosed by a surgeon or attending clinician.
Questionnaire design and administration
Structured questionnaires (Appendix 1) pre-tested by the researcher with a Cronbach reliability coefficient of 0.90 were administered to fifty-seven (57) small animal clinicians, which were representatives of government and private owned veterinary facilities in 6 states (Oyo, Lagos, Ogun, Osun, Ekiti and Ondo) of South-west, Nigeria. The questionnaire consisted of two parts. Part A comprises the clinicians’ demography, while part B included 7 sections: assessment of clinician’s understanding of SSIs, assessment of clinicians’ experience with SSIs, assessment of clinicians’ preventive measures (assessment of clinicians’ adherence to pre-surgical preparation procedures and assessment of post-surgical care), assessment of common sources of SSIs in respondents’practice, and assessment of challenges in providing appropriate SSI prevention. Four items were used to measure knowledge on SSI with a set cut-off limit of at least three correctly answered questions (correctness determined by CDC standards). Respondents with three and above rightly answered questions were classified as having good knowledge of SSI. Respondents with below three rightly answered questions were classified as having inadequate knowledge. Twenty-nine items (Select questions from part B; the preventive measures against SSIs taken by the clinician) were used to measure adherence to prevention protocol, by grading the positive/negative/multiple responses in accordance with the correct standard answers to the select questions, and setting a cut-off limit of at least twenty-three rightly answered questions to reveal either of the categories of adequate or non-adequate adherence to prevention strategies that the respondent falls into. The survey was conducted from October 2017 till February 2018.
Data analysis
Data were analyzed using Statistical Package for Social Sciences (SPSS) for windows version 17 software. Frequency distribution, charts and tables were used to summarize data obtained from the questionnaire and hospital records. Pearson Chi-square was used to test the influence of patient and operation related risk factors on SSI incidence and the relationships between demographics characteristics and the categorical variables (knowledge of SSI, Adherence to Preventive Strategies and Challenges faced in providing Services that enhance Prevention of SSIs) at 95% confidence interval.
RESULTS
SSIs prevalence and risk factors in veterinary hospitals
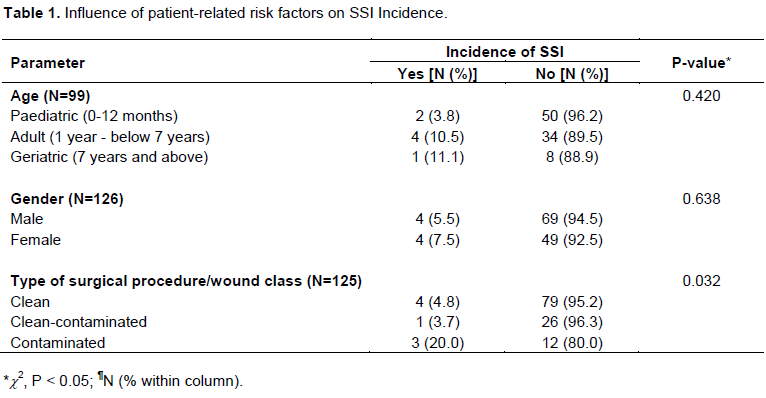
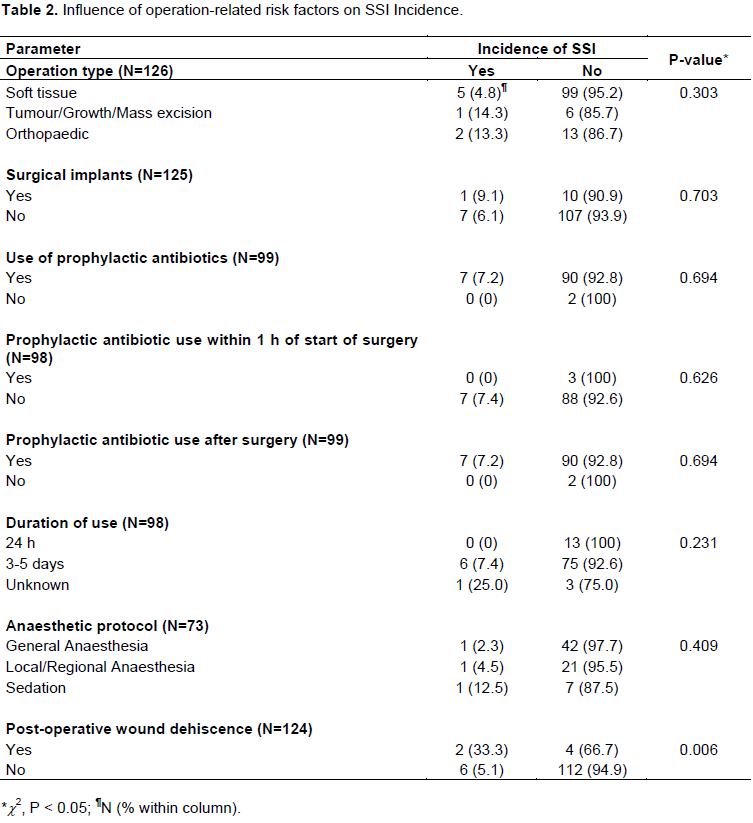
Out of 584 small animal (dogs) surgical cases obtained, only 126 cases (dogs) had completed postoperative case records and were thus eligible for inclusion. There were 57.9% males and 32.1% females. Most of the patients (41.3%) were of age group less than 1 year; 30.2% of 1-7 years and 7.1% of age above 7 years, while in 31.4% of the patients age was not recorded. Eight patients (6.3%) out of 126 cases had SSI. There was an association between post-operative wound dehiscence and SSI occurrence (P=0.006) and classification of the surgical procedures and SSI occurrence (P=0.032) (Tables 1 and 2).
Respondents’ educational qualifications and years of experience
Eighty percent of the respondents were male, while 20% were female, 90% respondents were in the age group of 24-40 years, 2% were in the 41-44 years, 4% were in the 45-54 years and 4% were in the 55-64 age group. The majority of respondents (64%) had only the Doctor of Veterinary Medicine (DVM) degree, while 36% had additional qualifications (Masters and Ph.D. in fields in Veterinary medicine). Most (64%) of the respondents had between 1 and 3 years of experience; 24% had between 4 and 10 years of experience; 6% of the respondents had between 11 and 20 years of experience and 6% had beyond 20 years of experience.
Respondents’ awareness of SSIs
The majority (97.7%) of respondents agreed that purulent drainage from deep incision or from a drain placed at surgical site can be evidence of post-surgical infection. Many (95.6%) also agreed that concurrent signs of fever, localized pain or tenderness with/without wound dehiscence can be evidence of post-surgical infection;
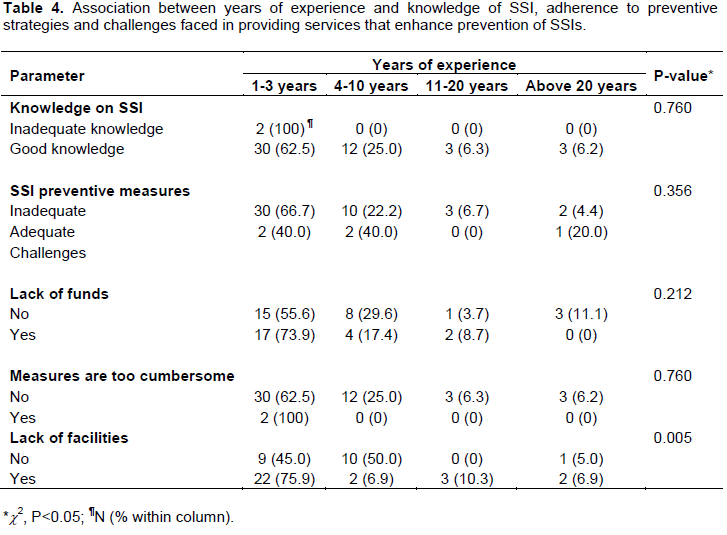
75.6% of respondents also agreed that swelling/presence of abscess following surgery can be evidence of post-surgical infection. All respondents (100%) agree that post-surgical infection could cause prolonged wound healing time. Pearson Chi-square revealed that 96% of respondents based on analysis of their responses to the four items used to measure knowledge with a cut-off limit set have very good knowledge of SSI (Table 4).
Respondents’ experience with SSI cases
Seventy-eight percent of respondents were used to managing SSI in their practice. Eighteen percent (18.0%) had lost patients due to SSIs, while 64% of respondents had witnessed patient’s recovery from SSI complications.
Assessment of respondents’ surgical facilities and aseptic practices
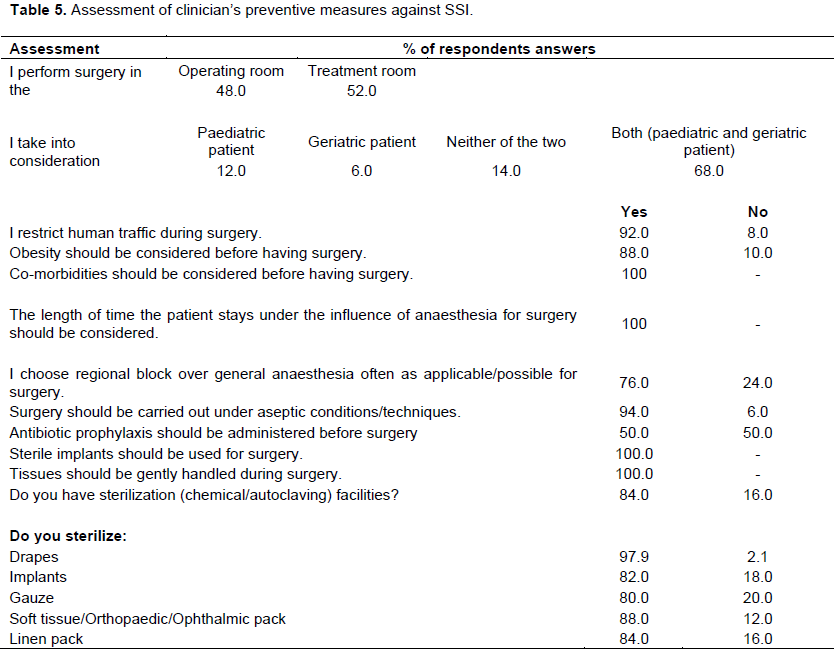
Only 48% of the respondents perform surgery in a designated operating room; however, the majority of respondents (92%), restrict human traffic during surgery. All respondents agree that: concurrent diseases should be considered before surgery; sterile implants should be used; and tissues should be handled gently. They also agreed that anaesthetic timing could influence SSI rate. Ninety-four percent agreed that adhering to aseptic principles and possession of sterilisation facilities could help prevent SSI occurrence. The majority of the respondents sterilise their drapes (97.9), gauze (80.0), implants (82.0), and soft tissue/orthopaedic pack (88.0). Drapes (58.7%) and gauze (69.2%) were sterilised by autoclaving. Implants were sterilised by chemical method (6.3%), autoclaving (68.8%) and both methods (25%). Surgical instrument packs were sterilised by chemical method (13.3%), autoclaving (73.3%) and both methods (13.3%) (Table 5).
Respondents’ compliance with theater etiquette
Most practitioners (91.3%) change into surgical attire before surgery and 54% put on cap, facemask, theatre gown, surgeon’s gown, gloves and theatre shoes for surgery. Fourteen percent change gloves 1 to 2 h into surgery while most (86%) do not change their gloves during surgery.
Respondents’ evaluation of risk factors for SSI
Age extremes and obesity were considered as risk factors by 88% of respondents (88%). Seventy-six percent prefer regional to general anaesthesia.
Assessment of adherence to pre-surgical preparation procedures
Test of relationship
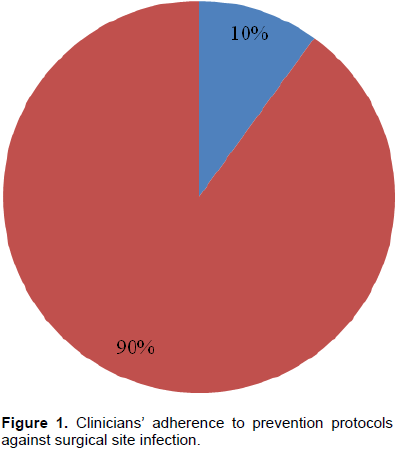
Pearson Chi-square revealed that 90% of respondents did not adequately adhere to prevention strategies based on analysis of their responses to the twenty-nine items (Select questions from part B; the preventive measures against SSIs taken by the clinician) used to measure adherence to prevention protocol, with a cut-off limit set. Only 10% adequately adhered to prevention protocols. (Figure 1 and Table 4)
Forty-eight percent of respondents have a place for specialized surgery and 66% have a recovery room. The majority of the respondents clipped the operative site using razor blade (64%) and 36% prepare patients’ skins with chlorhexidine and alcohol mixture. Sixty-two percent (62%) of respondents scrub their arms with water and antiseptic soap, 58.3% with brush, water and antiseptic soap, 10% scrub with water and non-antiseptic soap and 28.6% also use alcohol/alcohol based rubs.
Respondents’ experience with antibiotic therapy
Few respondents (19.1%) administer prophylactic antibiotics for all surgeries, some (25.5%) do, depending on the type of surgery and 62% administer antibiotics after surgery. The majority (75.5%) of respondents continues antibiotics for 3 to 7 days and 6.1% discontinue within 24 h.
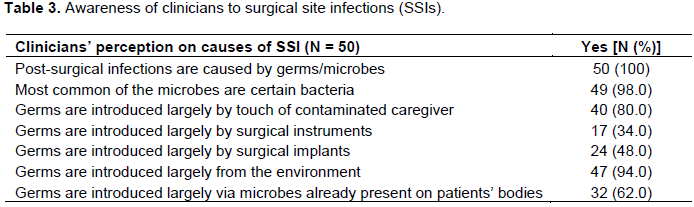
Assessment of sources of surgical site infections in clinicians’ practice
The majority (94%) of respondents agreed that microbes were introduced from the environment, hands of clinicians and caregivers (80%), surgical instruments (34%), surgical implants (48%) and patients’ bodies (62%) (Table 3).
Respondent challenges with SSIs prevention
Forty-six percent (46%) of the respondents agreed that they find it hard to keep up with preventive measures because of funding, while 58% agreed that they find it hard to keep up with preventive measures because of non-availability of facilities.
DISCUSSION
The results of this study have provided preliminary data on clinicians’ perception, risk factors and prevalence of SSIs in some small animal practices in Southwest Nigeria, which may be representative of the situation in many veterinary hospitals and clinics in Nigeria (Eyarefe, 2016). South-west Nigeria is the hub of small animal practice in the country due to its cities, commercial activities, relative peace and increasing dog acquisition for homes’ security and companionship (Eyarefe and Adetunji, 2018).
A large number of cases from hospital case records did not satisfy the inclusion criteria due to incompleteness of the patients’ medical records. A previous report (Akinrinmade, 2012) had raised concern about poor case record keeping in many veterinary clinics and hospitals in Nigeria. Unavailability of such data hampers planning and deductive information for decision making on patient health management. In this study, apart from 6.8% of SSIs cases obtained from case records, 78.7% of surveyed practice usually manage SSIs cases and 18.7% had lost patients due to SSIs. These findings corroborate a previous concern raised on the prevalence of SSI cases in veterinary practice in Nigeria (Eyarefe, 2016), which may have a far-reaching implication on patients’ morbidity, mortality and cost burden on pet owners (Birgand et al., 2014; Verwilghen, 2015). The study results have also revealed that many small animal practices have no designated room for surgery, have poor theater etiquette, poor patient presurgical preparation approach and post-surgical management protocol. This attitude contrasts the robust knowledge about SSIs garnered from literature and practice experience, as expressed in the result. The challenge of keeping up with standards for SSIs prevention and control seem global, but perhaps worst with veterinarians in the third world. Previous studies have shown that small animal clinicians’ poor attitude to SSI prevention strategies is a key factor behind SSI prevalence (Verwilghen and Singh, 2015). Similar observations were made among human surgeons due to failure of compliance with prevention guidelines (Anderson et al., 2013). It was noted that although SSIs was considered the most easily preventable hospital acquired infections judging by available literature and mitigating guidelines, yet compliance rate remain unsatisfactory (Anderson et al., 2013; Leaper et al., 2014; Umit et al., 2014).
SSI is a major problem in small animal practice in Nigeria. Effort at surveillance, training of veterinary health care providers and instituting prevention strategies must be heightened. Policy at reprimanding careless culprits must also be put in place to curb the menace.
CONCLUSION
The prevalence of SSIs in many veterinary clinics and hospitals calls for concern. Although many small animal practitioners have robust knowledge of SSIs risk factors, their compliance with prevention protocols is poor resulting in the prevalence and adverse effects.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Adriaanse AH, Pel M, Bleker OP (2000). Semmelweis: the combat against puerperal fever. Europe Journal Obstetric Gynaecology Reproduction Biology 90:153-158. |
|
|
Ahern BJ, Richardson DW (2012). Surgical site infection and the use of antimicrobials. In: Equine Surgery, 4th edn. Eds: JA Auer JA Stick, Elsevier/Saunders, St Louis, Missouri. pp. 68-84. |
|
|
Akinrinmade JF (2012). Evaluation of pattern of pet animal trauma at the veterinary Teaching hospitals, Ibadan, Nigeria. Nigeria Veterinary Journal 35(3):1007-1014. |
|
|
Akinrinmade JF, Oke BO (2012). Antibiotic prophylaxis in Gastro-intestinal surgery: An evaluation of current Veterinary Practices in Southwest Nigeria. International Journal Administration Veterinary Advance 4(4):256-262. |
|
|
Anderson ME, Foster BA, Weese JS (2013). Observational study of patient and surgeon preoperative preparation in ten companion animal clinics in Ontario Canada. BMC Veterinary Reserve 9:194. |
|
|
Berríos-Torres SI, Umscheid CA, Bratzler DW, Leas B, Stone EC, Kelz RR, Reinke CE, Morgan S, Slomkin JS, Mazuski JE, Dellinger EP (2017). Centers for Disease Control and Prevention Guideline for the Prevention of Surgical Site Infection, 2017. JAMA Surgery 152(8):784-791. |
|
|
Birgand G, Azevedo C, Toupet G, Pissard-Gibollet R, Grandbastien B, Fleury E, Lucet JC (2014). Attitudes, risk of infection and behaviours in the operating room (the ARIBO Project): a prospective, cross sectional study. BMJ Open 4(1):e004274. |
|
|
Clark FC (1907). A brief history of antiseptic surgery. Medical Library History Journal 5:145-172 |
|
|
Culver DH, Horan TC, Gaynes RP, Martone WJ, Jarvis WR, Emori TG, Banerjee SN, Edwards JR, Tolson JS, Henderson TS, Hughes JM (1991). National Nosocomial Infections Surveillance System. Surgical wound infection rates by wound class, operative procedure, and patient risk index. American Journal of Medicine 91:152S-157S. |
|
|
Eyarefe OD (2016). Risk factors, prevention and control strategies for surgical site infections in veterinary practice in Nigeria - A review. Journal of Veterinary Medicine and Animal Health 8(8):72-82. |
|
|
Eyarefe OD, Adetunji AG (2018). Dog breeds acquisition and owners awareness of associated surgical conditions in Nigeria. Journal of Veterinary Medicine and Animal Health 10(7):173-179. |
|
|
Hemani ML, Lepor H (2009). Skin preparation for the prevention of surgical site infection: which agent is best? Reverse Urology 11(4):190-195. |
|
|
Humes D, Lobo D (2005). Asepsis, antisepsis and skin preparation. Surgery (oxford). 23:297-298. 10.1383/surg.2005.23.8.297. |
|
|
Imai E, Ueda M, Kanao K, Miyaki K, Kubota T, Kitajima M (2005). Surgical site infection surveillance after open gastrostomy and risk factors for surgical site infection. Journal Infect Chemotherapy 11:141-145. |
|
|
Kaye KS, Schmit K, Pieper C, Sloane R, Caughlan KF, Sexton DJ, Schmader KE (2005). The effect of increasing age on the risk of surgical site infection. Journal of Infect Disease 191:1056-1062. |
|
|
Leaper DJ, Tanner J, Kiernan M (2014). Surgical site infection: poor compliance with guidelines and care bundles. International Wound Journal [Epub ahead of print]. |
|
|
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR, Hospital Infection Control Practices Advisory Committee (1999a). Guideline for prevention of surgical site infection, 1999. Infection Control and Hospital Epidemiology 20(4):247-280. |
|
|
Mangram AJ, Horan TC, Pearson ML (1999b). Guideline for Prevention of Surgical Site Infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. American Journal Infect Control 27(2):97-132. |
|
|
McMillan S (2014). An evidence-based approach to infection control in the operating theatre. Veterinary Nurse 5(4):194-200. |
|
|
National Nosocomial Infections Surveillance (NNIS) (1999). System report, data summary from January 1990-May 1999, issued June 1999. American Journal Infectious Control 27(6):520: |
|
|
Owens WD, Felts JA, Spitznagel EL Jr (1978). ASA physical status classifications: a study of consistency of ratings. Anesthesiology 49:239-243. |
|
|
Sabbatani S, Catena F, Neri F, Vallicelli C, Ansaloni L, Sartelli M, Coccolini F, Di Saverio S, Catena R, Lazzareschi D, Tarasconi A, Abongwa HK, De Simone B, Pinna A (2014). The Bolognese surgeon Guiseppe Ruggi: how and why septic surgery was introduced in Bologna in the middle half of the XIX century. Journal Surgical Resource 192:555-563 |
|
|
Umit UM, Sina M, Ferhat Y (2014). Surgeon behavior and knowledge on hand scrub and skin antisepsis in the operating room. Journal Surgical Education 71(2):241-245.at |
|
|
Verwilghen D (2015). Surgical site infections: What do we know? Equine Veterinary Journal 47:753-755. |
|
|
Verwilghen D, Singh A (2015). Fighting surgical site infections in small animals are we getting anywhere? Veterinary Clinical North American Small Animal Practice 45:243-276. |
|
|
Verwilghen D, Findji S, Weese JS, Singh A, Dupre G, Catry B, Van Galen G (2013). Evidence based hand hygiene in veterinary surgery: what is holding us back? In: Annual Symposium of the American College of Veterinary Surgeons, ACVS, San Antonio, Texas. |
|
|
Windahl U, Bengtsson B, Nyman AK, Holst BS (2015).The distribution of pathogens and their antimicrobial susceptibility patterns among canine surgical wound infections in Sweden in relation to different risk factors. Acta Veterinaria Scandinavica. 57:1. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


