Review
ABSTRACT
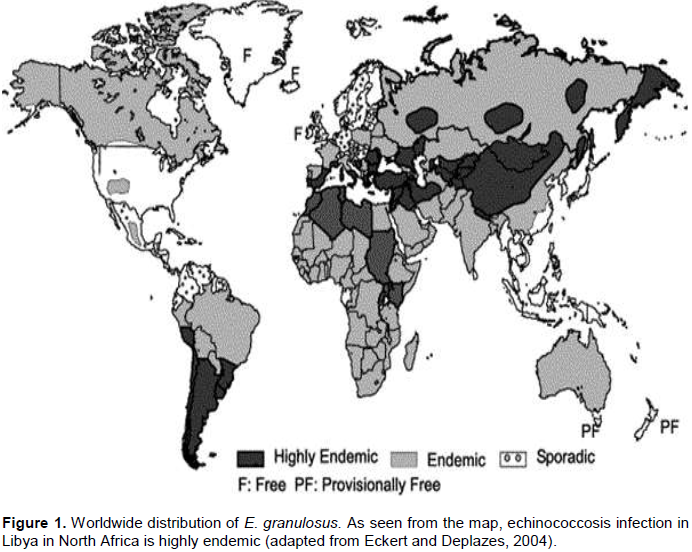
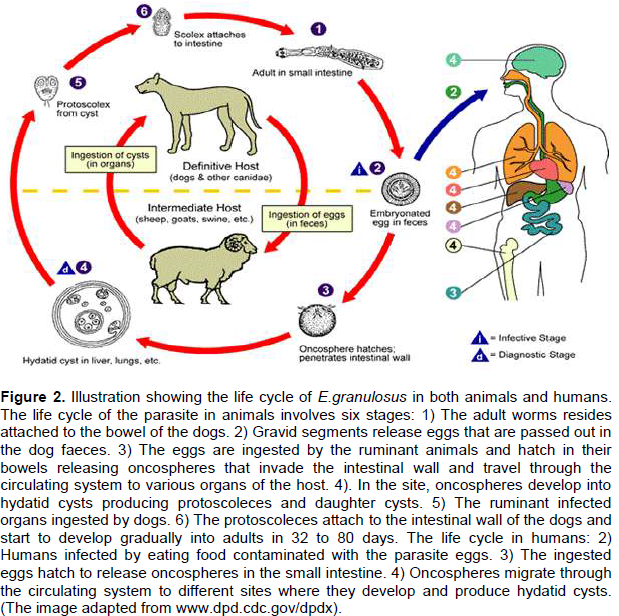
Echinococcus granulosus is a tiny tapeworm that parasitizes the small intestine of canids, mainly dogs, which act as definitive hosts for the parasite. Infected dogs are the main source of infection to humans and livestock which act as intermediate hosts resulting in hydatid disease condition. E. granulosus is widely distributed in many parts of the world, and is very common in North African countries. In Libya, the rate of infection with echinococcosis in dogs was reported to be lower than 7 to 80% in stray dogs, 34.8 to 60% in sheep/guard dogs and 7.7 to 21.6% in farm/house dogs. This data fulfills the world health organization (WHO) criteria and suggests that the incidence of infection with echinococcosis/ hydatidosis in some parts of the country can be reaching the level of hyper endemic. Diagnosis of echinococcosis in infected dogs can be performed by isolating the parasite from their faeces or from the contents of their small intestine after necropsy. Recent developments in immunodiagnostic assays for echinococcosis in dogs have been described. Public health and risk factors as well as ways of hydatid disease treatment and various control strategies, including the use of veterinary vaccines, have also been discussed.
Key words: Dogs, Echinococcus granulosus, prevalence, diagnosis, treatment, risk factors
INTRODUCTION
CONCLUSION
CONFLICT OF INTERESTS
REFERENCES
|
Abbasi I, Branzburg A, Campos-Ponce M, Abdel Hafez SK, Raoul F, Craig PS, Hamburger J (2003). Copro-diagnosis of Echinococcus granulosus infection in dogs by amplification of a newly identified repeated DNA sequence. Am. J. Trop. Med. Hyg. 69:324-30. |
|
|
Abushhiwa MH, Nolan MJ, Jex AR, Campbell BE, Jabbar A, Gasser RB (2010). Genetic classification of E. granulosus cysts from human, cattle and camels in Libya using mutation scanning-based analysis of mitochondrial loci. Mol. Cell Probes 24:346-351. |
|
|
Ahmad G, Nizami WA (1998). Copro-antigens: Early detection and suitability of an immunodiagnostic method for echinococcosis in dogs Vet. Parasitol. 77:237-244. |
|
|
Akalin S, Kutlu SS, Caylak SD, Onal O, Kaya S, Bozkurt AI (2014). Seroprevalence of human cystic echinococcosis and risk factors in animal breeders in rural communities in Denizli, Turkey. J. Infect. Dev. Count. 8: 1188-1194. |
|
|
Akhan O, Özmen MN (1999). Percutaneous treatment of liver hydatid cysts. Eur. J. Radiol. 32:76-85. |
|
|
Allan JC, Craig PS, Garcia Noval J, Mencos F, Liu D, Wang Y, Wen H, Zhou P, Stringer R, Rogan MT, Zeyhle E (1992). Copro-antigen detection for immunodiagnosis of echinococcosis and taeniasis in dogs and humans. Parasitol. 104:347-356. |
|
|
Allan JC, Wilkins PP, Tsang VC, Craig PS (2003). Immunodiagnostic tools for taeniasis. Acta Trop. 87:87-93. |
|
|
Arif SH, Shams-ul-Bari, Wani NA, Zargar SA, Wani MA, Tabassum R, Hussain Z, Baba AA, Lone RA (2008). Albendazole as an adjuvant to the standard surgical management of liver hydatid cyst. Int J. Surg. 6:448-451. |
|
|
Awan MAQ, Gusbi AM, Beesley WN (1990). Echinococcus in Libya. III. Further studies of E. granulosus in dogs. Ann. Trop. Med. Parasitol. 48:473-475. |
|
|
Babos S, Nemeth I (1962). Az echinococcis szerodiagnoztikajanak kerderehez. Mag. Allat. Lap. 17:58-60. |
|
|
Bal N, Nazim EK, Rabia A, Ali E, Fazilet K (2008). Uncommon locations of hydatid cysts. Saudi Med. J. 29:1004-1008. |
|
|
Ben-Amor N, Gargouri M, Gharbi HA, Golvan YJ, Ayachi K, Kchouck H (1986). Treatment of hepatic hydatid cyst in sheep by echographic puncture. Tunis. Med. 64:325-331. |
|
|
Ben-Musa NA, Sadek GS (2007). Prevalence of echinococcosis in street dogs in Tripoli district, Libya. J. Egypt Soc. Parasitol. 37:793-800. |
|
|
Blanton R, Wachira TM, Zeyhle E, Njoroge EM, Magabo J, Schantz PM (1998). Oxfendazole treatment for cystic hydatid disease in naturally infected animals. Am. Soc. Microbiol. 42:601-605. |
|
|
Bretagna S., Guilloun JP, Morand M, Houin R (1993). Detection of Echinococcus multilocularis DNA in fox faeces using DNA hybridisation. Parasitol. 106:193-199. |
|
|
Brunetti E, Kern P, Vuitton DA (2010). Expert consensus for the diagnosis and treatment of cystic and alveolar echinococcosis in humans. Acta Trop. 114:1-16. |
|
|
Buishi IE, Njoroge EM, Bouamra O, Craig PS (2005). Canine echinococcosis in northwest Libya: Assessment of coproantigen ELISA, and a survey of infection with analysis of risk-factors. Vet. Parasitol. 130: 223-232. |
|
|
Cabrera M, Canova S, Rosenzvit M, Guarnera E (2002). Identification of Echinococcus granulosus eggs. Diagn. Microbiol. Infect. Dis. 44:29-34. |
|
|
Casaravilla C, Malgor R, Rossi A, Sakai H, Nonaka N, Kamiya M, Carmona C (2005). Production and characterisation of monoclonal antibodies against excretory/secretory products of adult Echinococcus granulosus, and their application to coproantigen detection. Parasitol. Int. 54:43-49. |
|
|
Cetinkaya Z, Ciftci IH, Demirel R, Altindis M, Ayaz E (2005). A seroepidemiologic study on cystic echinococcosis in Midwestern region of Turkey. Saudi Med. J. 26:350. |
|
|
Chhabra MB and Singla LD (2009). Food-borne parasitic zoonoses in India: Review of recent reports of human infection. J. Vet. Parastol. 23:103-110. |
|
|
Christofi G, Deplazes P, Christofi N, Tanner I, Economides P, Eckert J (2002). Screening of dogs for E. granulosus coproantigen in a low endemic situation in Cyprus. Vet. Parasitol. 104:299-306. |
|
|
Cicogna D (1961). L,echinociccosi in Tripolitania. Boll. San. Del. Trip. pp. 2:3. |
|
|
Craig PS, Gasser RB, Parada L, Caprera P, Parietti S, Brgues C, Acuttis A, Agulla J, Snowden K, Paolillo E (1995). Diagnosis of canine echinococcosis: comparison of coproantigen and serum antibody test with arecoline purgation in Uruguay. Vet. Parasitol. 56:293-301. |
|
|
Craig PS, McManus DP, Lightwolers MW, Chabalgoity JA, Garcia HH, Gavidia CM, Gilman RH, Gonzalez AE, Lorca M, Naquira C, NietoA, Schantz PM (2007). Prevention and control of cystic echinococcosis. Latent Infect. Dis. 7:385-394. |
|
|
Craig PS, Rogan MT, Campos-Ponce M (2003). Echinococcosis: disease, detection and transmission. Parasitol. 127:Suppl S5-20. |
|
|
Dakak A (2010). Echinococcosis/hydatidosis: A severe threat in Mediterranean countries. Vet. Parasitol. 174:2-11. |
|
|
Dalimi A, Motamedi GHR, Syavashi M, Paykari H, Hablolvarid MH (2010). Detection of Echinococcus granulosus infection in dogs using coproantigen enzyme linked immunosorbent assay. Arch. Razi. Inst. 65:9-14. |
|
|
Deplazes P, Eckert J (1996). Diagnosis of the Echinococcus multilocularis infection in final hosts. Appl. Parasitol. 37:245-252. |
|
|
Deplazes P, Gottstein B, Eckert J, Jenkins DJ, Ewald D, Jimenez-Palacios S (1992). Detection of Echinococcus coproantigens by enzyme linked immunosorbent assay in dogs, dingoes and foxes. Parasitol. Res. 78:303-308. |
|
|
Dinkel A, Njoroge EM, Zimmermann A, Walz M, Zeyhle E, Elmahdi EI, Mackenstedt U, Romig T (2004). A PCR system for detection of species and genotypes of the Echinococcus granulosus-complex, with reference to the epidemiological situation in eastern Africa, Int. J. Parasitol. 34:645-653. |
|
|
Eckert J, Deplazes P (2004). Biological, epidemiological and clinical aspects of echinococcosis, a zoonosis of increasing concern. Clin. Microbiol. Rev. 17:107-135. |
|
|
Eckert J, Deplazes P, Craig PS, Gemmell MA, Gottstein B, Heath D, Jenkins DJ, Kamiya M, Lightowlers M, Meslin FX, Pawłowski ZS (2001). Echinococcosis in animals: clinical aspects, diagnosis and treatment. WHO/OIE Manual on echinococcosis in humans and animals: a public health problem of global concern. pp. 72-99. |
|
|
Gavidia CM, Gonzalez AE, Lopera L, Jayashi C, Angelats R, Barron EA, Ninaquispe B, Villarrea L, Garcia HH, Verastegui MR, Gilman RH (2009). Evaluation of nitazoxanide and oxfendazole efficacy against cystic echinococcosis in naturally infected sheep. Am. J. Trop. Med. Hyg. 80: 367-372. |
|
|
Gemmell MA, Johnstone PD, Oudemans G (1979). The effect of oxfendazole on Echinococcus granulosus and Taenia hydatigena infections in dogs. Res. Vet. Sci. 26:389-390. |
|
|
Gonzales AE, Garcia HH, Gilman RH, Gavidia CM, Tsang VCW, Bernal T, Falcon N, Romero M, Lopez-Urbina MT (1996). Effective, single-dose treatment of porcine cysticercosis with oxfendazole. Am. J. Trop. Med. Hyg. 54:391-394. |
|
|
Gusbi AM (1987a). Echinococcosis in Libya. I. Prevalence of Echinococcus granulosus in dogs with particular reference to the role of the dogs in Libyan Society. Ann. Trop. Med. Parasitol. 81:29-34. |
|
|
Gusbi AM (2010). The prevalence of E. granulosus infection in dogs and the parasitic risk in Libya. 4th Sci. Congr. Egypt. Soc. Anim. Manag. 112-119. |
|
|
Heath D1, Yang W, Li T, Xiao Y, Chen X, Huang Y, Yang Y, Wang Q, Qiu J (2006). Control of hydatidosis. Parasitol. Int. 55:247-252. |
|
|
Heath DD, Chevis RAF (1974). Mebendazole and hydatid cysts. Lanc. 2:218-219. |
|
|
Ibrahem, MM, Ibrahem WM, Abdorrahem MM, Ibrahem KM (2016). Livestock Hydatid Disease (Cystic Hydatidosis) in Libya: A review. Am. J. Anim. Vet. Sci. 11:70-84. |
|
|
Ito A, Urbani C, Jiamin Q, Vuitton DA, Dongchuan Q, Heath DD, Craig PS, Zheng F, Schantz PM (2003). Control of echinococcosis and cysticercosis: A public health challenge to international cooperation in China. Acta Trop. 86:3-17. |
|
|
Jenkins D J, Fraser A, Bradshaw H, Craig PS (2000). Detection of Echinococcus granulosus coproantigens in Australian canids with natural or experimental infection. J. Parasitol. 86:140-145. |
|
|
Kamiya M, Lagapa JT, Ganzorig S, Kobayashi F, Nonaka N, Yuzaburo O (2007). Echinococcosis risk among domestic definitive hosts, Jap. Emerg. Infect. Dis. 13:346-47. |
|
|
King CH, Fairley JK (2010). Cestodes (Tapeworms). In. Mandell GL, Bennett JE, Dolin R (Eds). Principles and Practice of Infectious Diseases. 7th edition. Philadelphia, Churchill Livingstone. pp. 3607-3616. |
|
|
Lacey E (1990). Mode of action of benzimidazole. Parasitol. Tod. 6:112-115. |
|
|
Lopera L, Moro P, Chavez A, Montes G, Gonzales A Gilman R (2003). Field evaluation of a coproantigen enzyme linked immunosorbent assay for diagnosis of canine echinococcosis in a rural Andean village in Peru. Vet. Parasitol. 117:37-42. |
|
|
Macpherson CNL, Karstad L, Stevenson P, Arundel JH (1983). Hydatid disease in the Turkana District of Kenya. III. The Significance of Wild |
|
|
Magnaval JF, Boucher C, Morassin B, Raoul F, Duranton C, Jacquiet P, Giraudoux P, Vuitton DA, Piarroux R (2004). Epidemiology of alveolar echinococcosis in southern Cantal, Auvergne region, France. J. Helminthol. 78:237-242. |
|
|
Malgor R, Nonaka N, Basmadjian I, Sakai H, Carambula B, Oku Y, Carmona C, Kamiya M (1997). Coproantigen detection in dogs experimentally and naturally infected with Echinococcus granulosus by a monoclonal antibody-based enzyme linked immunosorbent assay. Int. J. Parasitol. 27:1605-1612. |
|
|
Mathis A, Deplazes P (2006). Copro-DNA tests for diagnosis of animal taeniid cestodes. Parasitol. Int. 55:87-90. |
|
|
Mathis A, Deplazes P, Eckert J (1996). An improved test system for PCR-based specific detection of Echinococcus multilocularis eggs. J. Helminthol. 70:219-22. |
|
|
Maureen A (2008). More about Echinococcus tape worm in dogs. Worms & Germs Blog, Ont. Vet. Coll., Centre for Public Health and Zoonosis. |
|
|
McManus DP, Zhang W, Li J, Bartley PB (2003). Echinococcosis. Lanc. 362:1295-1304. |
|
|
Menezes da Silva A (2003). Hydatid cyst of the liver: Criteria for the selection of appropriate treatment. Acta Trop. 85: 237-242. |
|
|
Njoroge E, Mbithi P, Wachira T, Gathuma J, Gathura P, Maitho TE, Magambo J, Zeyhle MSE (2005). Comparative study of albendazole and oxfendazole in the treatment of cystic echinococcosis in sheep and goats. Int. J. Appl. Res. Vet. Med. 3:97-101. |
|
|
Office International des Epizootics (OIE) (2008). Echinococcosis/ hydatidosis. Terrestrial manual. |
|
|
Packer DE, Ali TM (1986). Echinococcus granulosus in dogs in Libya. Ann. Trop. Med. Parasitol. 80:137-139. |
|
|
Pawloeski ZS, Eckert J, Vuiton DA, Ammann RW, Kern P, Craig PS, Dar KF, Rosa F, de Filice C, Gottesein B, Grimm F, Macpherson CNL, Sato N, Todorov T, Uchino J, Sinner W, von Wen H (2001). Echinococcosis in humans: clinical aspects, diagnosis and treatment. In. Eckert J, Gemmell MA, Pawloeski ZS, (Eds). Manual on echinococcosis in humans and animals: A public health problem of global concern. WHO/OIE. pp: 20-66. |
|
|
Polat KY, Balik AA, Oren D (2002). Percutaneous drainage of hydatid cyst of the liver: long-term results. HPB. 4:163-166. |
|
|
Polat P, Mecit K, Fatih F, Selami S, Melike BK, Adnan O (2003). Hydatid Disease from Head to Toe 1. Radiographics 23(2):475-494 |
|
|
Prathiush PR, Placid ED, Ananda KJG (2008). Diagnosis of Echinococcus granulosus infection in dogs by a coproantigen sandwich ELISA. Vet. Arch. 78:297-305. |
|
|
Sakai H, Malgor R, Basmadjian I, Gallardo R, Carmona C, Sato H, Oku Y, Kamiya M (1995). An enzyme linked immunosorbent assay (ELISA) for the detection of Echinococcus granulosus coproantigen in dogs. Japan J. Parasitol. 44:453-461. |
|
|
Sakashita M, Sakai H, Kohno H, Ooi V, Oku V, Vagì K, Ito M, Kamiya M (1995). Detection of Echinococcus multilocularis coproantigens in experimentally infected dogs using murine monoclonal antibody against adult worms. Jap. J. Parasitol. 44:413-420. |
|
|
Schantz PM, Van den Bossche H, Eckert J (1982). Chemotherapy for larval echinococcosis in animals and humans: Report of a workshop. Z. Parasit. 53:5-26. |
|
|
Shambesh MK, Craig PS, Macpherson CNL, Rogan MT, Gusbi AM, Eechtuish FE (1999). An extensive ultrasound and serologic study to investigate the prevalence of human cystic echinococcosis in northern Libya. Am. J. Trop. Med. Hyg. 60:462-468. |
|
|
Stefania S, Avram E, Cozma V (2006). Detection of Echinococcus coproantigens by enzyme linked immunosorbant assay in dogs from the northwest of Romania. Bull. USAMV-CN 63:395-398. |
|
|
Stefanic S, Shaikenov BS, Deplazes P, Dinkel A, Torgerson PR, Mathis A (2004). Polymerase chain reaction for detection of patent infections of Echinococcus granulosus (sheep strain) in naturally infected dogs. Parasitol. Res. 92: 347-351. |
|
|
Teggi A, Lastilla MG, De Rosa F (1993). Therapy of human hydatid disease with mebendazole and albendazole. Antimicrob. Agents Chemother. 37:1679-1684. |
|
|
Thompson RCA (2008). The taxonomy, phylogeny and transmission of Echinococcus. Exp. Parasitol. 119:439-446. |
|
|
Thompson RCA (1995). Biology and systematics of Echinococcus. In: Thompson RCA, Lymbery AJ (Eds.). The biology of Echinococcus and hydatid disease. Cab International. pp. 1-50. |
|
|
Torgerson PR, Shaikenov BS, Rysmukhambetova AT, Abdybekova AM, Usenbayev AE, Baitursi nov KK (2003). Modelling the transmission dynamics of Echinococcus granulosus in rural Kazakhstan. Vet. Parasitol. 114:143-153. |
|
|
Unruh DHA, King JE, Eaton RDP, Allen JR (1973). Parasites of dogs from Indian settlements in northwestern Canada: A survey with public health implications. Can. J. Comp. Med. 37:25-32. |
|
|
Wachira TM, Macpherson CNL, Gathuma JM (1991). Release and survival of Echinococcus eggs in different environments in Turkana, and their possible impact on the incidence of hydatidosis in man and livestock. J. Helminthol. 65:55-61. |
|
|
Watson-Jones DL, Macpherson CNL (1988). Hydatid disease in the Turkana district of Kenya. VI. Man-dog contact and its role in the transmission and control of hydatidosis amongst the Turkana. Ann. Trop. Med. Parasitol. 82:343-356. |
|
|
Yorganci K, Sayek I (2002). Surgical treatment of hydatid cysts of the liver in the era of percutaneous treatment. Am. J. Surg. 184:63-69. |
|
|
Zare-Bidaki M, Mobedi I, Naddaf SR, Kia EB, Mahmoudi M, Piazak N, Nekouie H, Sadeghieh Ah ari S, Habibzadeh Sh, Siavashi M (2009). Prevalence of Echinococcus spp. infection using coproantigen ELISA among canids of Moghan plain, Iran. Iran J. Public Health 38:112-118. |
|
|
Zhang W, Li J, McManus PD (2003). Concepts in immunology and diagnosis of hydatid disease. Clin. Microbiol. Rev. 16:18-36. |
|
|
Zhang W., Zhang Z., Shi B, Li J, You H, Tulson G, Dang X, Song Y, Yimiti T, Wang J, Jones MK, McManus DP. (2006). Vaccination of dogs against Echinococcus granulosus the cause of cystic hydatid disease in humans. J. Infect. Dis.194:966-974. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


