ABSTRACT
The main objective of this paper was to examine the effect of internal control on quality health service delivery in Greater Iganga Local Government. This study adopted a cross-sectional research design. A population of 205 health facilities were targeted. Stratified and simple research techniques were applied to obtain a sample size of 127 health facilities whose accounting managers, health managers and instructors, laboratory officers, personnel managers and drug stock administrators and supervisors formed the unit of inquiry on internal control while health service clients formed the unit of inquiry on the quality of health services offered. Data were collected by the use of questionnaires which were self-administered to 635 respondents. The responses were aggregated to the respective units of analysis (Health Centers). SPSS was employed to execute correlation and regression analysis. The finding revealed that internal control is positive and significantly linked to quality health service delivery (r=0.715; p<0.001). This implies that internal control considerably influences quality health service delivery in Greater Iganga Local Government. The study findings accrued from cross-sectional study design which is screwed with certain limitations. Future study should consider the same study through other study designs. Moreover, the study was done within the setting of Uganda local government, thus future study should consider testing this model in other local governments.
Key words: Internal control, quality health service delivery, local government.
Attaining service gratification in the whole world demands that local governments improve on the quality of services they offer (Makanyeza et al., 2013; McNeil et al., 2009; Sudhahar and Selvam, 2008). Service quality particularly in the health sector is linked with improved human well-being and in return, enhances productivity of life (Kimenyi, 2013).
Nevertheless, in spite of the imperative role of quality health service delivery as characterized above, the health service delivery in Uganda is poor (Nabukeera, 2016). Lack of trained human resources, poor organization of health services, and drug inadequacy, dilapidated health infrastrature systems among others have combined in services, and drug inadequacy, dilapidated health infrastrature systems among others have combined in numerous proportions to weaken the health service quality (Nabukeera, 2016; Wane and Gayle, 2013). This condition has continued in spite of several reforms such as improved training health institutions, improved health service management system, more fund allocation by various funding organizations, revamped health infrastructures, improved drug management approaches, enhanced health models, upgraded remuneration systems among others (Nabukeera, 2016; WHO, 2015; UNHCO, 2014).
Health service quality in Uganda is underpinned by the Health Sector Strategic Plan (HSSP) with an objective of improving the health of every person in a manner that is legitimate and quick to respond to their health needs. This is further articulated in the vision 2040 blueprint for example, that aims at enabling government to transform its society and provide citizens with better standard of living by focusing on improving quality health. Despite this, poor service delivery in the health sector has evidently persisted (MOH, 2013).
Health service delivery in Uganda is often characterized by weak public health systems (Nabukeera, 2016; UNHCO, 2014). Besides, an audited report published in 2016 by Auditor General on local authorities in Uganda show that health services offered in Greater Iganga Local Government is unsatisfactory (Office of The Auditor General, 2016). The aforementioned report and studies indicate deficient and dilapidated infrastructure, questionable drug inventory techniques and quality, unreliable staff, unqualified and limited human resources among others. Consequently, there has been increased mortality rate, low life expectancy, questionable health conditions, lack of trust in health systems among others (MOH, 2013; WHO; 2015).
In view of the aforementioned, internal control has been regarded a distinctive factor to enhanced health quality service delivery (Wane and Gayle, 2013; Ntongo, 2012). Internal control is a system that is guided by a framework invented to reliably assure the organization that its purpose for existence will be achieved (COSO, 2013).
The frame between internal control and quality health service delivery is well explained by stakeholder theory (Freeman, 1984). This theory explains how organizations, people and the group relate to one another. This theory assumes that an organization is comprised different stakeholders and each stakeholder has differing interests which need to be taken into account if the organization is to achieve its purpose (Shao, 2010). Guided by stakeholder theory, Greater Iganga Local Government needs to identify and incorporate needs of stakeholders such as clients, government, funding agencies and employees in order to improve on the quality of services they deliver. In spite of the effectiveness of internal control in improving quality health service delivery in the health sector (Ntongo, 2012), this link has not been empirically tested in Uganda’s public health sector.
The closest was by Ntongo (2012) however, this was in private sector. The absence of a similar study in the public sector necessitates this study. Furthermore, empirical evidence indicates that such test in the realm of Greater Iganga Local Government is subtle.
Internal control and quality service delivery in organizations
Internal control has been pointed out as unique and essential to the success of organizations (Synder et al., 1989; Pillai, 2010). Internal control is a process guided by the organization’s framework that reliably assures the entity that its purpose for existence will be achieved (COSO, 2013). The rationale is that the stakeholders are demanded to provide framework that safeguard resources, promote consistent information, enhance adherence to recommended laws and meet effectively the operations of the organization. Conceptually, internal control is comprised five interconnected components: control environment, risk assessment, control activities, information and communication, and monitoring activities (COSO, 2013). There effective implementation safeguard resources against loss, misuse and damage (Long and Jeremy, 2013; Brent, 2010). This requires each organization to adopt internal control that is appropriate to its particular needs and activities (MWE, 2018).
Literature exhibits the significant role of internal control in quality service delivery. Effective internal control enhances desired service quality (Ntongo, 2012). In this regard, organizations with well-structured internal control improves performance and meets client’s expectations (Oppong et al., 2016; Umar et al., 2018). This translates into quality service delivery. Internal control promotes efficiency in utilization of organization resources whereby jobs are carried out as described, employees available at work at all times, and equitable allocation of resources and hence, timely service quality delivery (MWE, 2018). Similarly, internal control has a potential to ensure usage of funds on planned organizational activities, investment of idle funds, and regular monitoring of utility (Oppong et al., 2016). Monitoring is an important driver to quality service delivery. It provides vital feedback on the extent of service delivery and whether delivery of those services makes any difference both to clients and organization (Rossi, 1993). Besides, it provides insights which are useful for detecting changes in performance and understanding trends over time (Woodall et al., 2015). The objective is to ensure that organization is functioning as envisioned and that their systems are enhanced to proactively respond to variations to gain competitive advantage (Long and Jeremy, 2013). Comprehensively, monitoring measure if the core objective spelt out in the description of the organization core existence is being achieved (Long and Jeremy, 2013)
Similarly, organization’s aptitude to make better resolutions that reciprocate desired outcome is influenced by the good information (COSO, 2013), thus, information must be suitable, well-time, up-to-date, exact, and available (COSO, 2013). Moreover, for information to meet its purpose, it must be communicated to the intended persons (Long and Jeremy, 2013). As communication is enhanced, there is a possibility that service quality will improve as organizations become more focused on clients requirements and needs (Musenze et al., 2014; Mwazo et al., 2017). This positions communication as a unique predictor to QSD (Musenze et al., 2013; Mwazo et al., 2017). Furthermore, communication is seen to be important in all quality service delivery practices. Complete and timely communication, simplifies employees tasks thereby incorporating their needs and meet them as required (Musenze et al., 2013). This means that all communication practices must be controlled in order to realise better outcome.
Effective control activities have been positioned as a key to performance (QSD) (Oppong et al., 2016). Service quality is reliant on insight of organizational control activities. Effective and efficient processes (internal activities) directly impact quality of service delivery (World Meteorological Organization (WMO), 2014). In this view, control activities are considered as activities that provide evidence on the status of the organization and actions to be taken. The said actions must be supported by internal control objectives, procedures and policies that enable managers to address risk timely, effectively and efficiently (COSO, 2013) as cited by Oppong et al. (2016). According to Australian Council of Healthcare Standards (ACHS, 2018), COSO (2013), and Long and Jeremy, (2013), risk assessment is important in mitigating risks towards realization of service quality. Risk assessment and service quality, are not isolated processes (Mwazo et al., 2017). They provide a system through which organization’s operations are assessed, the processes involved examined, and enhance its performance in an effort to foster service quality (COSO, 2013; ACHS, 2018). Evidence showed that organizations that have successfully implemented risk management reciprocated quality improvements scenario (Umar et al., 2018; ACHS, 2018; Mwazo et al., 2017). This programme to be functional, organizations (Lgs) need to exhibit allegiance to the procedures stipulated and define the objectives of all participants. Similarly, governing authority must allocate adequate resources to proficiently lessen, regulate and govern all risk in the organization (ACHS, 2018; COSO, 2013). The reviewed literature demonstrates internal control as a considerable indicator of quality service delivery in organization (Mwazo et al., 2017; Pillai, 2010). Therefore, it is hypothesized that: H1: Internal control is positively linked to quality health service delivery in Greater Iganga Local Government.
Service quality
Service quality reveals the general judgement as to whether service offered meets client’s contentment (Parasuraman et al., 1988). According to Zeithmal et al. (1990), service quality is the variance obtained from what customer anticipate and the results received. Furthermore, in some scenarios, clients’ anticipation surpasses performance of services received leading to discontentment (Parasuraman et al., 1985). Nevertheless, Philip and Hazlett (1997) point out that as much as SERQUAL model (Parasuraman et al., 1988) is universally used, there is dissatisfaction that the present operationalization of service quality is highly inadequate, besides, it may in fact be flawed more especially in evaluating the quality service offered in other service organizations, namely: database service, education, hospitals/healthcare, libraries, or information services. Furthermore, it is uncertain as to whether SERQUAL measures service quality or satisfaction (Philip and Hazlett, 1997). On the other hand, SERPERF model (Gronroos, 1984) measured service quality based on the test of qualitative methods. Conversely, Philip and Hazlett (1997) suggested a hierarchical model known as pivot-core-periphery model for assessing service quality in service sector. This model exhibits the distinction between the service delivered, workforce and the organization delivered of the service. Moreover, P-C-P model only holds the employee(s) and organization accountable for service delivery and the proof as to whether service delivered is of quality and met the intendent purpose depends on the client (Philip and Hazlett, 1997). Similarly, P-C-P model allocates divergent intensity to the quality service measurements. Therefore, to assess service quality, judgments of all measurements of the service: input, processes and outputs should be put into consideration (Musenze et al., 2014).
Conceptual framework
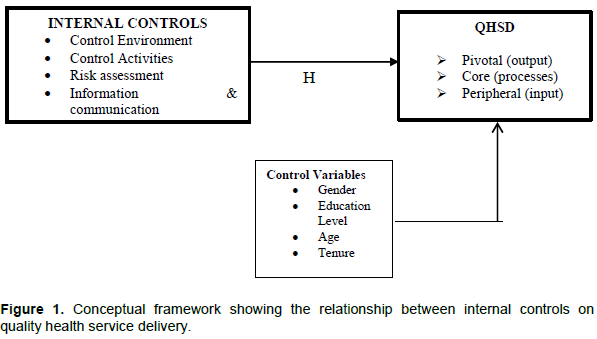
Ascending from reviewed literature and theories, the model shown in Figure 1 was proposed to guide this study.
Hypothesis development
Ascending from the reviewed literature and the model (Figure1), the following hypothesis was formulated:
H1: Internal control is positively linked to quality health service delivery in Greater Iganga Local Government.
Study design, sample and sampling technique
This study utilized cross-sectional research design. Data was collected from a sample size of 127 health facilities out of 205 health facilities from Ministry of Health, as advised by Krejcie and Morgan (1970) for determining sample size. As Greater Iganga Local Government (Mayuge, Bugiri, Namutumba, Luuka, Namayingo and Iganga districts), health sector is ranked along different tiers (HCIIs, HCIIIs, HVs and Referral Hospitals), stratified sampling technique was applied in selecting 1Referral Hospital, 4 HC IVs, 22 HC IIIs, and 100 HC IIs. Subsiquently, employing simple sampling technique, four bowls marked with layer’s name were provided. All designations of units of analysis (HCs) were labled on a paper and placed on those corresponding bowls as per the layer’s name, from which we draw the required samples without replacement until the sample size of 127 was attained. This sample size fulfilled the required threshold of 100 and above as recommended by Bailey (1994). Questionnaires were self-administered to 635 respodents. Given that the clients are in the best position to judge as to whether service delivered is of quality and met the intendent purpose (Philip and Hazlett, 1997), the QHSD part of the instrument was answered by 635 respondents who were registered through a convenient sampling technique. Clients departing from public health centres were intercepted, persuaded, and asked to take part in the study by answering the items in the instruments. All their responses were aggregated to the unit of analysis level (Health Centres). Conversely, the accounting managers, health managers, superintendent of health centers, health supervisors, health instructors, drug supervisors, laboratory officers, personnel managers and drug stock administrators formed the unit of inquiry on internal control.
Measurements of variables
Internal control
To unearth the realm of internal control, two internal control models were reviewed: COSO model (COSO, 2013) and Long and Jeremy (2013). According to COSO (2013), internal control is comprised five measurements: control environment, risk assessment, control activities, information and communication, and monitoring activities. On the other hand, Long and Jeremy extracted eight dimensions namely: control environment, monitoring and evaluation, arrival and customs clearing, transportations, receiving, storage distribution and people (Long and Jeremy, 2013). However, the emphasis was limited to pharmaceutical management systems and operationalization, but not other organizations. Therefore, to excavate the dimensions of effective internal control in health service organizations, this study zeroed down to COSO model. The items in the COSO model were adjusted to fit this study. For validation purposes, the items in the tool were acquiesced to 10 specialists comprising both local government practitioners and academicians. The content validity index was established to be above 0.80. This was beyond the suggested minimum of 0.70 (Nunnally, 1978). Items were anchored on a five-point Likert-like scale (1-5) ranging from Strongly Disagree to Strongly Agree. The adjusted questionnaire had 50 items.
Quality health service delivery
P-C-P model established by Philip and Hazlet (1997) was utilized. In this context, the QSD measurements encompassed output, process and input. The uniqueness with this model is that it holds the personnel and organization accountable for service delivery and the proof as to whether service delivered is of quality and met the intendent purpose depends on the client (Philip and Hazlett, 1997). For validation purposes, the items in the tool were acquiesced to 10 specialists comprising both local government practitioners and academicians. The content validity index was established to be above 0.80. This was beyond the suggested minimum of 0.70 (Nunnally, 1978). Items were anchored on a five-point Likert-like scale (1-5) ranging from Strongly Disagree to Strongly Agree. The adjusted questionnaire had 23 items.
Validity and reliability
For validation purposes, the items in the tool were acquiesced to 10 specialists comprising both local government practitioners and academicians. All study variables registered a content validity index which was established to be above 0.80. This was beyond the suggested minimum of 0.70 (Nunnally, 1978).
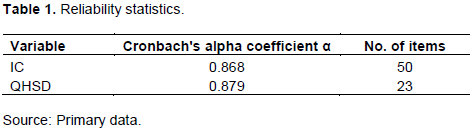
Similarly, the reliability scale of the two scales of internal control and QHSD were also established using Cronbach Alpha Coefficient as generated by Statistical Package for Social Scientists (SPSS). Cronbach Alpha coefficient for all the study variables were above 0.85. This was well above the recommended minimum requirement of 0.70 (Nunnally, 1978). Therefore, the scale for measuring Internal Control and Quality Health Service Delivery was reliable as demonstrated in Table 1.
Data processing and analysis
Quantitative technique was utilized in the analysis of data. Data obtained from the questionnaires were edited, coded, characterized and analysed using Statistical Package for Social Sciences (SPSS), computer software. Statistical analysis resulted from SPSS handling of data from questionnaire was presented for discussion.
Correlation and regression analysis
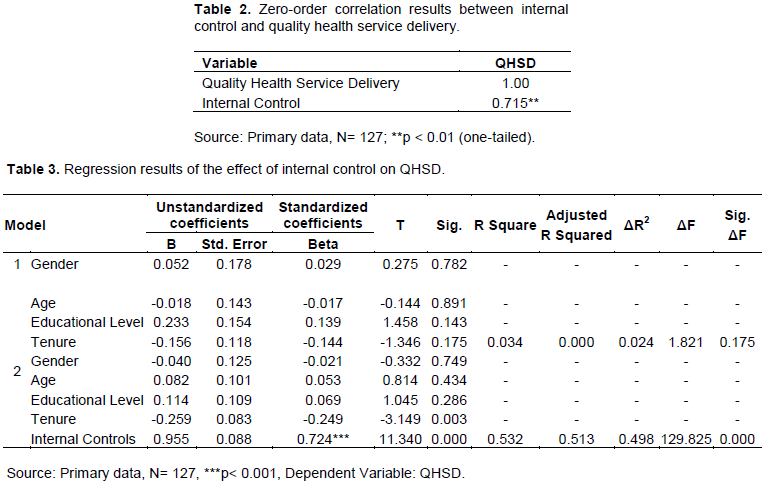
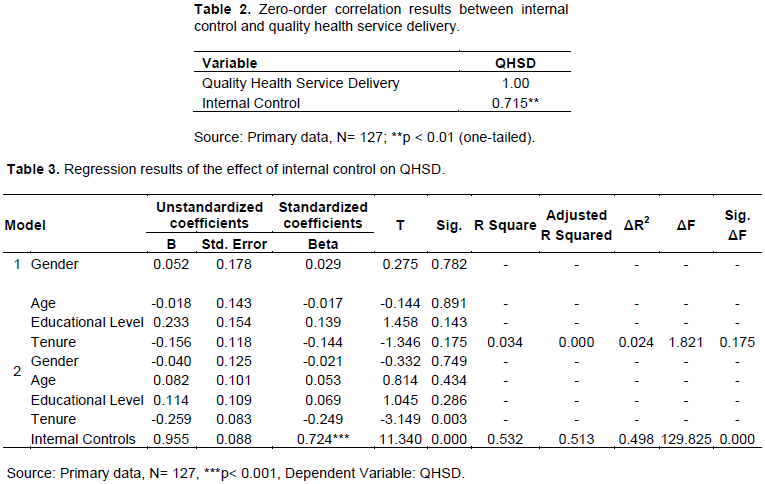
Pearson’s product moment correlation coefficient and regression analysis were used to assess the link between the study variables. The statistical results are shown in Table 2.
The generated correlation results displayed in Table 2, demonstrate a positive and significant (r = 0.715; p < 0.01) link between internal control and quality health service delivery. The model evaluation results exhibited in Table 3, point out that Model 1 is statistically insignificant (R2 = 0.034; p > 0.05). Given that demographic measurements have formerly remained utilized as control variables in studies (Min and Khoon, 2014; Al-Khali and Mahmoud, 2012), in Model 1, the control variables were controlled (gender, age, educational level and tenure). The findings show that control variables explained 3.4% of the overall variation in QHSD, suggesting that the support of demographic measurements to QHSD in Greater Iganga Local Government is statistically insignificant (R2 = 0.034; p > 0.05). Conversely, regression analysis outcome, showed in Table 3: Model 2, discovered that 53.2% of the overall variation in QHSD is illustrated by internal control (R2 = 0.532; p < 0.001). The regression coefficient of change in QHSD due to a change in internal control was significant (β = 0.724; t = 11.340; p < 0.001). Based on the correlation results (r = 0.715 p < 0.01), strengthened by regression analysis results (R2 = 0.532; p < 0.001), and regression coefficient (β = 0.724; t = 11.340; p < 0.001), hypothesis (H1) is upheld.
The study assessed the relationship between internal control and QHSD in Greater Iganga Local Government. The study established that the link between internal control and QHSD was positive and significant. This finding is in consonant with Synder et al. (1989), Pillai (2010), Ntongo (2012), Oppong et al. (2016) and Umar et al (2018), suggesting that as organizations enforce policies and procedures such as the presence of the frameworks that safeguard resource, compliance to the stipulated laws, better reporting systems, risk assessmement, proactive monitoring and evaluation and regular auditing exercises, the quality of healthcare is likely to recuperate as organizations (Lgs) aim to meet the requirements of their esteemed clients, they will quickly respond to arising issues proactively in an effort to realize exceptional outputs, processes and inputs.
The study examined the effect of internal control and QHSD in Greater Iganga Local Government. It was found out that the link between internal control and QHSD was positive and significant. Therefore, it is imperative to note that internal control plays a pivotal role to improve QHSD.
Given this deliberation, this study supplements to the service literature by positioning internal control as an important precursor to QHSD within the setting of Uganda in the perspective of GILG.
In spite of the fact that this study has demonstrated valuable comprehension to relevant stakeholders, it is also limited in the following ways:
(1) The findings resulted from cross-sectional study design, making it challenging to validate conclusion in relation to other study designs. Consequently, upcoming studies ought to think through the same study in respect to other research design perspectives such as longitudinal design among others.
(2) The study was done within the setting of Uganda Local Government. The findings maybe limited due to geographical location. Thus, it is suggested that the future studies ought to ponder on a similar study by testing this model in a local authority(s) elsewhere.
The authors have not declared any conflict of interests.
REFERENCES
|
Al-Khali A, Mahmoud AB (2012). The role of demographics in patients' perception towards the quality of health care services provided at public hospital in Damascus. European Journal of Economics, Finance and Administrative Sciences 48:113-121.
|
|
|
|
Australian Council of HealthCare Standards (ACHS) (2018). Report of the ACHS National Safety and Quality Health Service (NSQHS) Standards Survey 1:1-113.
|
|
|
|
|
Bailey KB (1994). Methods of Social Research (4th edition) New York: Macmillan.
|
|
|
|
|
Brent M (2010). Advantages and disadvantages of Internal Control. New Delhi: New Age International press.
|
|
|
|
|
Committee of Sponsoring Organizations of the Treadway Commission (COSO) (2013). Internal Controls: Integrated framework. KPMG LLP. a Swiss entity. Available at
View
|
|
|
|
|
Freeman RE (1984). Strategic Management: a Stakeholder Approach. Boston: Pitman.
|
|
|
|
|
Gronroos C (1984). A Service Quality Model and its Marketing Implications. European Journal of Marketing 18(4):36-45.
Crossref
|
|
|
|
|
Kimenyi MS (2013). Accountability and service delivery in Africa. Journal of African Development 15(1):11-17.
|
|
|
|
|
Krejcie RV, Morgan DW (1970). Determining Sample Size for Research Activities. Educational and psychological Measurement 30(6):607-610.
Crossref
|
|
|
|
|
Long B, Jeremy K (2013). Self-Assessment of Internal Control Health Sector - A Toolkit for Health Sector Managers. Health Finance and Governance. Available at:
View
|
|
|
|
|
Makanyeza C, Kwandanyi HP, Ikobe BN (2013). Strategies to Improve Service Delivery in Local Authorities. International Journal of Information Technology and Business Management 15(1):1-11.
|
|
|
|
|
McNeil M, Andre H, Sladjana C, Prism R (2009). Governance Working Paper Series: Citizen Review of Service Delivery and Local Governance in Bosnia and Herzegovina. World Bank, Washington, DC.
|
|
|
|
|
Min S, Khoon CC (2014). Demographic factors in the evaluation of service quality in higher education: A Structural Equation Model (SEM) approach. International Journal of Marketing Studies 6(1):90.
Crossref
|
|
|
|
|
Ministry of Health (MOH) (2013). Ministry of Health- Republic of Uganda. Annual health sector performance report. Available at:
View
|
|
|
|
|
Ministry of Water and Environment (Republic of Uganda) (2018). Administrative Guidelines on the Internal Control Framework and Internal Audit Standards: Integrated Internal Controls System (COSO).
|
|
|
|
|
Musenze IA, Munene JC, Ntayi JM (2013). Communication Practices and Quality Service Delivery Tradition: Uganda's Local Government Perspective. International Journal of Innovation and Applied Studies 4(2):413-423.
|
|
|
|
|
Musenze IA, Munene JC, Ntayi JM, Waiswa B (2014). Communication and quality Service delivery in Uganda's local government: The mediating influence of total quality Management. African Journal of Science, Technology, Innovation and Development 6(2):93-103.
Crossref
|
|
|
|
|
Mwazo EM, Weda C, Omondi MM, Njenga AN (2017). Role of internal control system on service delivery in the national treasury of Taita-Taveta County, Kenya. International Journal of Economics, Commerce and Management 5(8):431-447.
|
|
|
|
|
Nabukeera M (2016). Challenges and Barriers to the Health Service Delivery System in Uganda. Journal of Nursing and Health Sciences 5(2):30-38.
|
|
|
|
|
Ntongo V (2012). Internal controls, financial accountability and service delivery in private health providers of Kampala District. (Unpublished thesis) Makerere University.
|
|
|
|
|
Nunnally JC (1978). Psychometric theory (2nd edition). New York, McGraw-Hill.
|
|
|
|
|
Office of the Auditor General (Republic of Uganda) (2016). Local Authorities: Annual Report of the Auditor General on the Financial Statements for the Year Ended 30th June, 2016.
|
|
|
|
|
Oppong M, Owiredu A, Abedana VN, Asante E (2016). The impact of internal control on performance of Faith Based NGOs in Accra. Research Journal of Finance and Accounting 7(12):110-125.
|
|
|
|
|
Parasuraman A, Valarie A, Zeithmal, Berry LL (1985). A conceptual model of service quality and its implications for future Research. Journal of Marketing 49(1):41-50.
Crossref
|
|
|
|
|
Parasuraman A, Valarie A, Zeithmal, Berry LL (1988). Consumer perceptions of service quality. Journal of Retailing 64(1):12-40.
|
|
|
|
|
Philip G, Hazlett SA (1997). The measurement of service quality: A new P-C-P attributes model. International Journal of quality and reliability management 14(3):260-286.
Crossref
|
|
|
|
|
Pillai NR (2010). Inventory management performance in machine tool SMEs: What factors do influence them. Journal of industrial Engineering 3(3):542-560.
Crossref
|
|
|
|
|
Rossi PH (1993). Evolution: A Symmetric Approach. Thousand Oaks. Calf: Sage Publications.
|
|
|
|
|
Shao G (2010). The effect of Board Structure on Media Companies' performance: A stakeholder perspective. Journal of Media Business Studies 7(3):1-47.
Crossref
|
|
|
|
|
Sudhahar CJ, Selvam M (2008). Service quality perception in the health care services: A case study of hospital services. International Journal of Biosciences and Technology 1(1):25-31.
|
|
|
|
|
Synder NH, Broome OW, Zimmerman K (1989). Using Internal Controls to Reduce Employee Theft in Small Businesses. Journal of Small Business Management 8(1):48-55.
|
|
|
|
|
Uganda National Health Consumer's Organisation (UNHCO) (2014). Health Annual Report. Available at:
View
|
|
|
|
|
Umar H, Dikko MU (2018). The effect of internal control on performance of commercial banks in Nigeria. International Journal of Management Research and Review 8(6):13-32.
|
|
|
|
|
Wane W, Gayle M (2013). Education and health services in Uganda: Data for results and accountabilty. World Bank, Washington, DC.
|
|
|
|
|
Woodall WH, Fogel SL, Steiner SH (2015). The Monitring and Improvement of Surgical-Outcome Quality. Journal of Quality Technology 47(4):383-399.
Crossref
|
|
|
|
|
World Health Organisation (WHO) (2015). World Health Organisation: Accountability frameworks.
|
|
|
|
|
World Meteorological Organization (WMO) (2014). The World Meteorological Organization strategy for service and its implementation plan. Switzerland.
|
|
|
|
|
Zeithmal VA, Parasuraman A, Berry LL (1990). Delivery quality service: Balancing customer perceptions and expectations. New York: The Free Press. Available at:
View
|
|