Full Length Research Paper

ABSTRACT
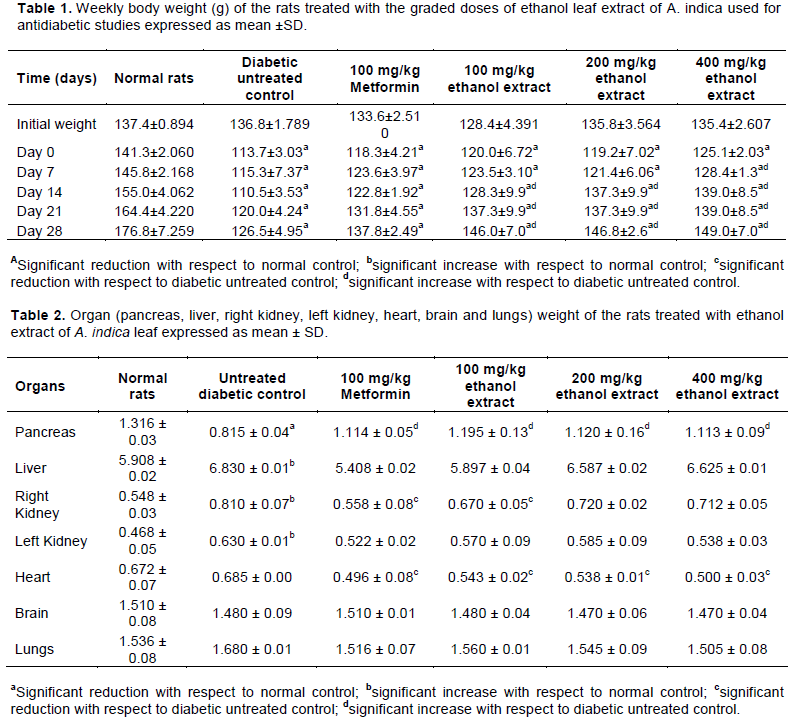
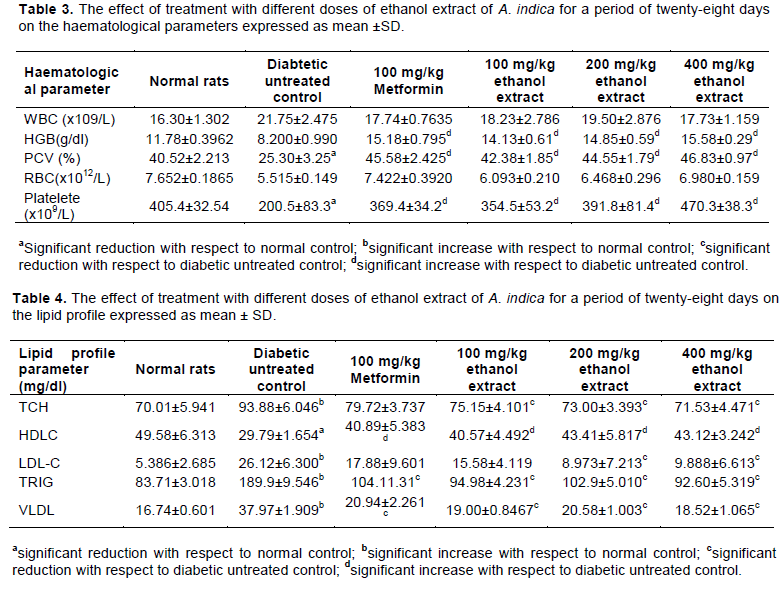
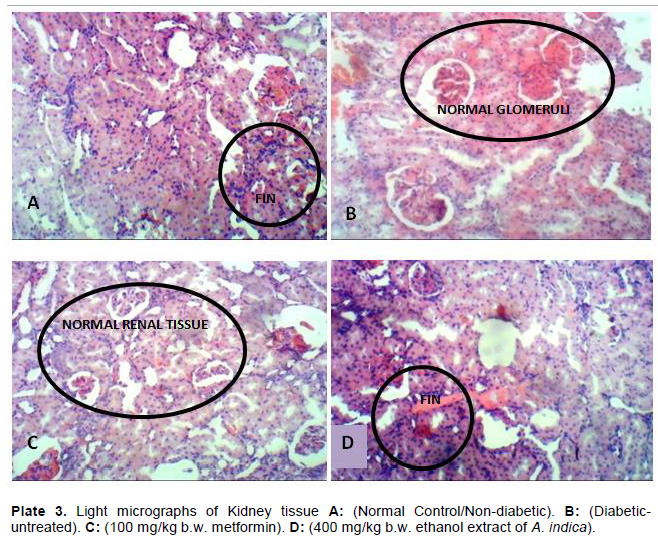
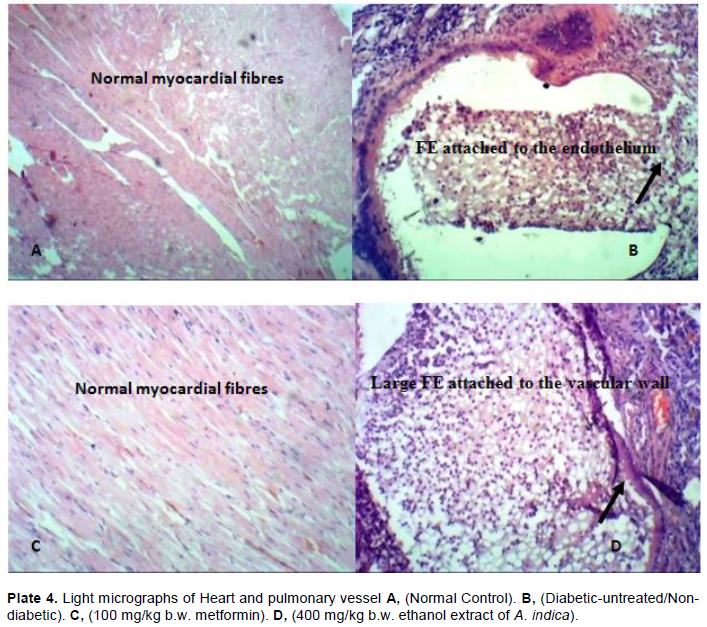
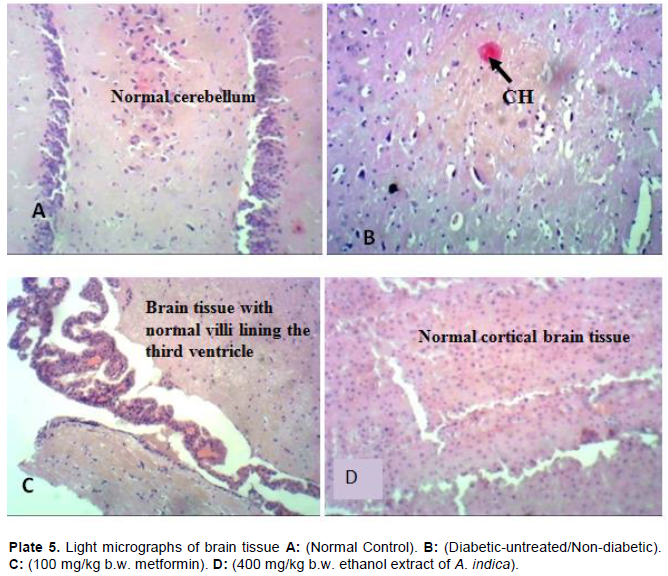
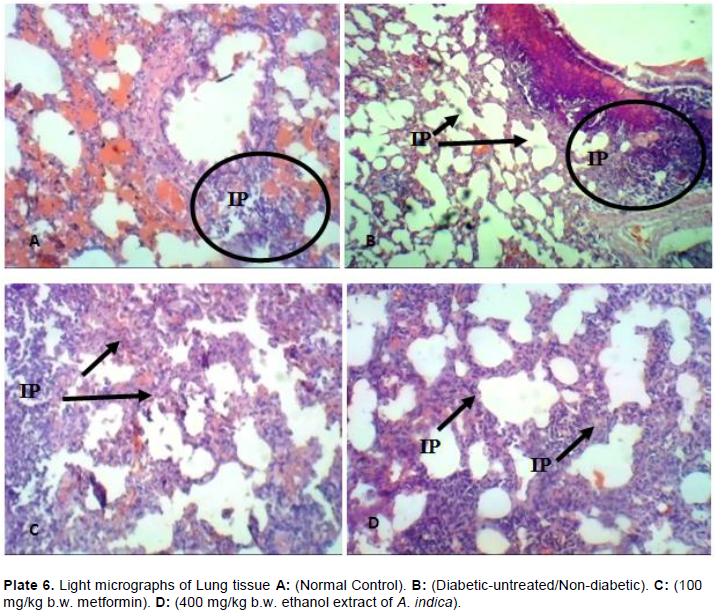
This study was carried out to evaluate the effects of ethanol extract of Azadirachta indica leaf on haematological parameters, lipid profile, body weight, organ weight and histopathological functions of streptozotocin-induced diabetic rats. Diabetes was induced by a single intraperitoneal administration of streptozotocin (50 mg/kg bw.). The haematological parameters, lipid profile and histopathological investigations were performed using standard methods. Continuous administration of ethanol extract of A. indica leaf for a period of four weeks significantly (p<0.05) increased the bodyweight of the streptozotocin-induced diabetic rats compared with the diabetic-untreated control. There was a significant (p<0.05) increase in the haemoglobin concentration, packed cell volume, red blood cells, platelet count and a significant (p<0.05) reduction in the total serum cholesterol, low-density lipoprotein, triglycerides and very-low-density lipoprotein of the groups treated with ethanol extract of A. indica compared with the diabetic-untreated control. The result of the histopathological studies showed regeneration of the organs for the groups treated with 400 mg/kg bw of the extract compared with the diabetic-untreated control. These results suggest that the ethanol extract of A. indica can be considered as an excellent remedy for diabetes and an alternative to antidiabetic drugs in reducing the complications associated with type II diabetes mellitus.
Key words: Diabetes, Azadirachta indica, haematological parameters, Lipid profile, Bodyweight, Histopathological functions.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
CONCLUSION
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
ETHICAL APPROVAL
REFERENCES
|
Adekunle AS, Adelusi TI, Kamdem J, Ishmael A, Akintade BB (2016). Insulinomimetic, Antihyperlipidemic and Antioxidative Properties of Azadirachta indica. Possible Mechanism of Action. British Journal of Medicine and Medical Research 17(5):1-11. |
|
|
Adeloye D, Ige JO, Aderemi AV, Adeleye N, Amoo E,Auta A, Oni G (2017). Estimating the prevalence, hospitalisation and mortality from type 2 diabetes mellitus in Nigeria: a systematic review and meta-analysis. BMJ Open 7(5). |
|
|
Akbarzadeh A, Norouzian D, Mehrabi MR., Jamshidi SH., Farhangi A, Allah VA, Mofidian SMA, Lame RB (2007). Induction of diabetes by streptozotocin in rats. Indian Journal of Clinical Biochemistry. 22(2):60-64. |
|
|
Alese MO, Adewole SO, Ijomone MO, Ajayi SA, Omonisi A (2013). Histological studies of pancreatic β-cells of streptozotocin-induced diabetic wistar rats treated with methanolic extract of Sphenocentrum jollyanum. Journal of Pharmaceutical Science and Innovation 2(2):8-12. |
|
|
American Diabetes Association (ADA) (2019) "Classification and diagnosis of diabetes: standards of medical care in diabetes." Diabetes Care 42(5):13-28. |
|
|
Anjali K, Ritesh K, Sudarshan M, Jaipal SC, Kumar S (2013). Antifungal efficacy of aqueous extracts of neem cake, karanj cake and vermicompost against some phytopathogenic fungi. The Bioscan 8:671-674. |
|
|
Bandyopadhyay U, Biswas K, Sengupta A (2004). Clinical studies on the effect of Neem (Azadirachta indica) bark extract on gastric secretion and gastroduodenal ulcer. Life Sciences 75(24):2867-2878. |
|
|
Bellamy L, Casas JP, Hingorani AD, Williams D (2009). Type 2 diabetes mellitus after gestational diabetes: A systematic review and meta-analysis. Lancet 373:1773-1779. |
|
|
Biney EE, Nkoom M, Darkwah WK, Puplampu JB (2020). High-performance liquid chromatography analysis and antioxidant activities of extract of Azadirachta indica (neem) leaves. Pharmacognosy Research 12(1):29-34. |
|
|
Bodduluru LN, Sistla R (2014). Chemopreventive and therapeutic effects of nimbolide in cancer: The underlying mechanisms. Toxicology In Vitro 28(5):1026-1035. |
|
|
Bruno V (2015). Pathophysiology of diabetic dyslipidaemia: Where are we? Diabetologia 58(5):886-899. |
|
|
Chiha M, Njeim M, Chedrawy EG (2012). Diabetes and coronary heart disease: A risk factor for the global epidemic. International Journal of Hypertension. Article ID 697240:7. |
|
|
Coustan DR (2013). Gestational diabetes mellitus. Clinical Chemistry 59:1310-1321. |
|
|
Das AR, Mostofa M, Hoque ME, Das S, Sarkar AK (2010). Comparative efficacy of neem (Azadirachta indica) and metformin hydrochloride (comet®) in streptozotocin induced diabetes melitus in rats. Bangladesh Journal of Veterinary Medicine 8(1):75-80. |
|
|
Daye C, Bin L, Yunhui L (2013). Antihyperglycemic Effect of Ginkgo biloba Extract in Streptozotocin-Induced Diabetes in Rats. BioMed Research International. Article ID 162724:7. |
|
|
DeWitt DE, Hirsch IB (2003). Outpatient insulin therapy in type 1 and type 2 diabetes mellitus: scientific review. Journal of the American Medical Association 289(17):2254-2264. |
|
|
Debrah A, Godfrey OM, Ritah K (2020). Prevalence and Risk Factors Associated with Type 2 Diabetes in Elderly Patients Aged 45-80 Years at Kanungu District Hindawi Journal of Diabetes Research Volume 2020, Article ID 5152146:5. |
|
|
Diaz-Valencia PA, Bougneres P, Valleron AJ (2015). Global epidemiology of type 1 diabetes in young adults and adults: A systematic review. BMC Public Health 15:255. |
|
|
Donahoe SM, Stewart GC, McCabe CH, Mohanavelu S, Murphy SA, Cannon CP, Antman EM (2007). Diabetes and mortality following acute coronary syndromes. Journal of the American Medical Association 298:765-775. |
|
|
Ebaid H, Bashandy SAE, Alhazza IM, Hassan I, Al-Tamimi J (2019). Efficacy of a Methanolic Extract of Adansonia digitata Leaf in Alleviating Hyperglycemia, Hyperlipidemia, and Oxidative Stress of Diabetic Rats. Biomedical Research International. Article ID 2835152:10. |
|
|
Erukainure OL, Ebuehi OAT, Adeboyejo FO, Aliyu M, Elemo GN (2013). Haematological and biochemical changes in diabetic rats fed with fiber-enriched cake. Journal of Acute Medicine 3(2):39-44. |
|
|
Ezeigwe OC, Ononamadu CJ, Enemchukwu BN, Umeoguaju UF, Okoro JC (2015). Antidiabetic and antidiabetogenic properties of the aqueous extracts of Azadirachta indica leaves on alloxan induced diabetic wistar rats. International Journal of Biosciences 7:116-126. |
|
|
Ezeigwe OC, Ezeonu FC, Igwilo IO (2020). Antidiabetic property and antioxidant potentials of ethanol extract of Azadirachta indica leaves in streptozotocin-induced diabetic rats. The Bioscientist 8(1):1-11. |
|
|
Femlak M, Gluba A, Cialkowska-Rysz A, Rysz J (2017). The role and function of HDL in patients with diabetes mellitus and the related cardiovascular risk. Lipid in Health and Disease. 16.10.1186/s12944-017-0594-3. |
|
|
Friedewald WT, Levy RI, Fredrickson DS (1972). "Estimation of the concentration of low-density lipoprotein cholesterol in plasma, without use of preparative ultracentrifuge. Clinical Chemistry 18:499-02. |
|
|
Govindachari TR, Suresh G, Gopalakrishnan G, Banumathy B, Masilamani S (1998). Identification of antifungal compounds from the seed oil of Azadirachta indica. Phytoparasitical 26(2):109-116. |
|
|
Gupta NK, Srivastva N, Bubber P, Garg S, Mohammad O (2017). Protective potential of Azadirachta Indica leaf extract in diabetic rat liver. International Journal of Pharmacognosy and Phytochemical Research 9(2):174-180. |
|
|
Habluetzel A, Pinto B, Tapanelli S, Saviozzi M, Nkouangang J, Chianese G, Lopatriello A, Tenoh AR, Yerbanga RS, Taglialatela-Scafati O, Esposito F, Bruschi F (2019). Effects of Azadirachta indica seed kernel extracts on early erythrocytic schizogony of Plasmodium berghei and pro-inflammatory response in inbred mice. Malaria Journal 18(35). |
|
|
Heidari Z, Mahmoudzadeh-Sagheb H, Moudi BA (2008). Quantitative study of sodium tungstate protective effect on pancreatic beta cells in streptozotocin-induced diabetic rats. Micronutrients 39(8):1300-1305. |
|
|
Holman N, Young B, Gadsby R (2015). Current prevalence of type 1 and type 2 diabetes in adults and children in the UK. Diabetes Medicine 32:1119-1120. |
|
|
International Diabetes Federation (IDF) Diabetes Atlas (2019). ninth edition. |
|
|
Irfan HM, Asmawi MZ, Khan NA, Sadikun A (2016). Effect of ethanolic extract of Moringa oleifera lam. leaves on body weight and hyperglycemia of diabetic rats. Pakistan Journal of Nutrition 15(2):112. |
|
|
Iyare E, Obaji NN (2014). Effect of aqueous leaf extract of Azadirachindica on some haematological parameters and blood glucose level in female rats. Nigerian Journal of Experimental and Clinical Biosciences 2:54. |
|
|
Jain M (2012). Histopathological changes in diabetic kidney disease. Clinical Queries and Nephrology 102:127-133. |
|
|
Karamanou M, Protogerou A, Tsoucalas G, Androutsos G and Poulakou-Rebelakou E (2016). Milestones in the history of diabetes mellitus: the main contributors. World Journal of Diabetes 7:1-7. |
|
|
Katerji M, Filippova M, Duerksen-Hughes (2019). Approaches and method to measure oxidative stree in clinical samples: Research application in the cancer field. Oxidative Medicine and Cellular Longevity. Article ID127950 page 29. |
|
|
Kazi S (2014). Use of traditional plants in diabetes mellitus. International Journal of Pharmaceutics 4(4):283-9. |
|
|
Kim JD, Kang SM, Seo BI, Choi HY, Choi HS, Ku SK (2006). Anti-diabetic activity of SMK001, a poly herbal formula in streptozotocin-induced diabetic rats: therapeutic study. Biological and Pharmaceutical Bulletin 29(3):477-82. |
|
|
Kirigia JM, Sambo HB, Sambo LG (2009). Economic burden of diabetes mellitus in the WHO African region. BMC Int Health Hum Rights 9:6. |
|
|
Klein R, Klein BE, Moss SE, Wong TY (2006). The relationship of retinopathy in persons without diabetes to the 15-year incidence of diabetes and hypertension: Beaver dam eye study. Transactions of the American Ophthalmological Society 104:98-107. |
|
|
Kumar BR, Praveen TK, Nanjan MJ, Karvekar MD, Suresh B (2007). Serum glucose and triglyceride lowering activity of some novel glitazones against dexamethasone-induced hyperlipidemia and insulin resistanance. Indian Journal of Pharmacology 39:299-302. |
|
|
Lee WL, Cheung AM, Cape D, Zinman B (2000). Impact of diabetes on coronary artery disease in women and men: A meta-analysis of prospective studies. Diabetes Care 23:962-968. |
|
|
Mbanya JC, Motala AA, Sobngwi E (2010). Diabetes in sub-Saharan Africa. Lancet 375:2254-2266. |
|
|
Nathan SS, Kalaivani K, Murugan K (2005). Effects of neem limonoids on the malaria vector Anopheles stephensi Liston (Diptera: Culicidae). Acta Tropica 96(1):47-55. |
|
|
Oh PS, Lee SJ, Lim KT (2006). Hypolipidemic and antioxidative effects of the plant glycoprotein (36 kDa) from Rhus verniciflua stokes fruit in Triton WR-1339-induced hyperlipidemic mice. Biosciences Biotechnology and Biochemistry 70:447-56. |
|
|
Piero MN, Nzaro GM, Njagi JM (2015). Diabetes mellitus - A devastating metabolic disorder. Asian Journal of Biomedical and Pharmaceutical Sciences 5:1. |
|
|
Raja SB, Murali MR, Kumar NK and Devaraj SN (2011). Isolation and partial characterisation of a novel lectin from Aegle marmelos fruit and its effect on adherence and invasion of Shigellae to HT29 cells. PloS One 6:e16231. |
|
|
Ray A, Banerjee BD, Sen P (1996). Modulation of humoral and cell-mediated immune responses by Azadirachta indica (Neem) in mice. Indian Journal of Experimental Biology 34:698-701. |
|
|
Robert DK (2019) the deadly cost of insulin. American Journal of Managed Care Volume 25. |
|
|
Said G (2007). Diabetic neuropathy-A review. Nature Clinical Practice Neurology 3:331-340. |
|
|
Schellenberg ES, Dryden DM, Vandermeer B, Ha C, Korownyk C (2013). Lifestyle interventions for patients with and at risk for type 2 diabetes: A systematic review and meta-analysis. Annals of Internal Medicine 159:543-551. |
|
|
Sen P, Medira PK, Ray A (1992). Effects of Azadirachta indica A Juss on some biochemical, immunological and viscera parameters in normal and stressed rats. Indian Journal of Experimental Biology 30:1170-5. |
|
|
Shailey S, Basir SF (2012). Strengthening of antioxidant defense by Azadirachta indica in alloxan-diabetic rat tissues. Journal of Ayurveda Integrated Medicine 3(3):130-135. |
|
|
Shin S, Hwang B, Muhammad K, Gho Y, Song J, Kim W, Kim G, Moon S (2019). Nimbolide Represses the Proliferation, Migration, and Invasion of Bladder Carcinoma Cells via Chk2-Mediated G2/M Phase Cell Cycle Arrest, Altered Signaling Pathways, and Reduced Transcription Factors-Associated MMP-9 Expression. Evidence-Based Complementary and Alternative Medicine. ID 3753587: 12 pages. |
|
|
Shrivastava DK, Swarnkar K (2014). Antifungal activity of leaf extract of neem (Azadirachta indica Linn) International Journal of Current Microbiology and Applied Sciences 3(5):305-308. |
|
|
Srinivasan-Rao BD, Saileela CH (2013). Anti-hyperlipidemic activity of methanolic extract of Rhinacanthus nasutus. International Journal of Research in Pharmacy and Chemistry 3:708-11. |
|
|
Subramani R, Gonzalez E, Arumugam A, Narayan M, Nandy S, Gonzalez V, Medel J, Camacho F, Ortega A, Bonkoungou S, Dwivedi AK, Lakshmanaswamy R (2016). Nimbolide inhibits pancreatic cancer growth and metastasis through ROS-mediated apoptosis and inhibition of epithelial-to-mesenchymal transition. Science and Reproduction 6:19819. |
|
|
Tietze NW, Finley PR, Pruden EL (1990). Clinical Guide to Laboratory Tests. 2nd Edition, WB. Saunders, Philadelphia, 304-306. |
|
|
Titford M (2009). Progress in the development of microscopical techniques for diagnostic pathology. Journal of Histotechnology 32:9-19. |
|
|
Trinder P (1969). Determination of glucose in blood using glucose oxidase with an alternative oxygen acceptor. Annals of Clinical Biochemistry 6:24-27. |
|
|
World Health Organization (WHO) (2019). Classification of Diabetes mellitus, pp. 13-14. ISBN 978-92-4-151570-2. |
|
|
Yan Z, Sylvia HL, Frank BH (2018). Global aetiology and epidemiology of type 2 diabetes mellitus and its complications. Europe PMC 14:88-98. |
|
|
Zafar M, Naqvi SN (2010). Effects of STZ-Induced diabetes on the relative weights of kidney, liver and pancreas in albino rats: A comparative study. International Journal of Morphology 28(1):135-142. |
|
|
Zhang C, Li J, Hu C, Wang J, Zhang J, Ren Z, Song X, Jia L (2017). Antihyperglycaemic and organic protective effects on pancreas, liver and kidney by polysaccharides from Hericium erinaceus SG-02 in streptozotocin-induced diabetic mice. Scientific Reports 7:10847. |
|
|
Ziegler R, Neu A (2018). Diabetes in childhood and adolescence. Deutsches Arzteblatt International 115(9):146-156. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


