ABSTRACT
The association between hyperuricemia and metabolic syndrome (MS) has been reported in many studies. The authors performed this cross-sectional study to determine the association between hyperuricemia and the MS among diabetic patients in Dakar. Type 2 diabetic patients received as part of their follow-up at the Marc Sankalé Center of Abass Ndao Hospital in Dakar were enrolled. For each patient, blood samples and 24 h urine collection were performed. Hyperuricemia was defined for uric acid concentrations > 416 µmol/l in men and > 357 µmol/l in women and the MS was evaluated according to WHO criteria. Statistical analysis was done using the XLSTAT 2019 software. A total of 153 type 2 diabetic patients were included with an average age of 56.63 years. Thirty-one percent (31%) of patients had metabolic syndrome and 32% of them had hyperuricemia. Significant correlations were found between serum uric acid and some components of the MS including triglyceride levels (r = 0.25, p = 0.002), microalbuminuria (r = 0.19, p = 0.018), and fasting glucose (r = - 0.22, p = 0.005). The authors found that hyperuricemia is frequent in patients with MS and this could be considered as a biomarker associated with the presence of this syndrome.
Key words: Hyperuricemia, metabolic syndrome, type 2 diabetes, uric acid.
Metabolic syndrome (MS) is a known risk factor for many chronic diseases including type 2 diabetes mellitus, cardiovascular diseases (CVD), chronic kidney diseases (CKD), among others (Lee and Sanders, 2012).
The World Health Organization (WHO) defines MS by the presence of insulin resistance [e.g. type 2 diabetes (T2D) or indications of abnormal glucose metabolism], together with at least two of the following factors: use of anti-hypertensive medication and/or high blood pressure (BP) ≥ 140 mmHg systolic or ≥ 90 mmHg diastolic], plasma triglycerides >150 mg/dL, HDL cholesterol < 35 mg/dL in men or < 39 mg/dL in woman, body mass index (BMI) > 30 kg/m2 and/or waist-hip ratio >0.9 in men, > 0.85 in women, and urinary albumin excretion rate ≥ 20 µg/min or albumin creatinine ratio (UACR) ≥ 3.4 mg/mmol (Alberti and Zimmet, 1998). It is a real public health problem around the world, with a frequency and a prevalence increasing in both developing and developed countries (ViswanathanI and Deepa, 2006). Serum uric acid (SUA) is the end product of purine metabolism in humans and many studies have reported the association between hyperuricemia and the various components of the MS, in particular obesity, blood pressure, hyperlipidemia as well as glucose intolerance (Ames et al., 1981; Wilson et al., 2005; Lorenzo et al., 2007; Fabbrini et al., 2014; Zhang et al., 2016; Cheserek et al., 2018; Huang et al., 2020).
Indeed, epidemiological studies have suggested that uric acid is a risk factor for cardiovascular disease and in the MS a high frequency of hyperuricemia is found which would be a compensatory mechanism to counteract the oxidative stress found in the circumstances of this syndrome (Hansel et al., 2004; Sung et al., 2004; Ishizaka et al., 2005; Ismail et al., 2018). Thus, the authors carried out this study with the main objective of determining the association between uricemia and metabolic syndrome in a population type 2 diabetics.
Study design and subjects
It was a cross-sectional and prospective study conducted over 7 months from March to September 2018. This study was carried out on type 2 diabetics received in consultation as part of their follow-up at the Marc Sankalé Center of Abass Ndao Hospital in Dakar.
The study was approved by the Scientific Ethics Committee of the Faculty of Medicine, Pharmacy and Odontology of the Cheikh Anta Diop University of Dakar and informed consent was also obtained from patients.
Patients with conditions or taking drugs that could interfere with uric acid levels as well as those who did not express their consent to participate in the study were not included. In this study, the MS was assessed according to the WHO criteria (Alberti and Zimmet, 1998).
This definition includes a state of diabetes mellitus or a fasting blood sugar ≥ 110 mg/dl (6.10 mmol/l) in addition to two of the following features:
1) A waist / hip ratio > 0.90 for men and > 0.85 for women or a BMI ≥ 30 Kg /m2;
2) A triglyceride level > 150 mg/dl (1.7 mmol/l) and / or HDL-C < 35 mg/l (0.9 mmol/ l) for men and < 39 mg/dl (1.0 mmol/l) for women;
3) A blood pressure > 140/90 mm Hg or an antihypertensive treatment;
4) and microalbuminuria > 30 mg/24h.
Data collection
The epidemiological data were collected using a questionnaire and for each patient, blood samples were taken after 12 h of overnight fasting by venipuncture at the bend of the elbow. A 24 h urine collection was also performed for the determination of microalbuminuria.
The blood samples were centrifuged at 3000 revolutions/min for 5 min and were immediately processed or stored at -20ºC until use. All biochemical variables, except HbA1c, were measured using Cobas 6000 / c501® analyzer (Roche, Hitachi, Germany) following the protocol provided by the reagent manufacturer and glycated hemoglobin (HbA1c) was measured using D-10® system (BioRad, USA).
Uric acid was determined by the uricase enzymatic method with quantification of the hydrogen peroxide formed by a Trinder reaction.
The body mass index (BMI) was defined as weight in kilograms divided by the square of the height in meters. The blood pressure (BP) was measured in a sitting position by using a standardized automatic electronic sphygmomanometer.
Hyperuricemia has been defined for uric acid concentrations > 416 µmol/L in men and > 357 µmol/L in women (Hochberg et al., 2003).
Statistical analysis
Statistical analysis was performed using XLSTAT 2019 software. Data were presented as frequencies and percentages for categorical variables and as the mean ± SD for continuous variables. All continuous variables were tested for normal distribution by Shapiro–Wilk test, and the significance of differences between groups was tested with an unpaired t-test and/or Mann–Whitney U-test. Categorical variables were compared using the Chi-squared test and the association between the variables was evaluated using the Spearman correlation test. A p value less than 0.05 were considered significant.
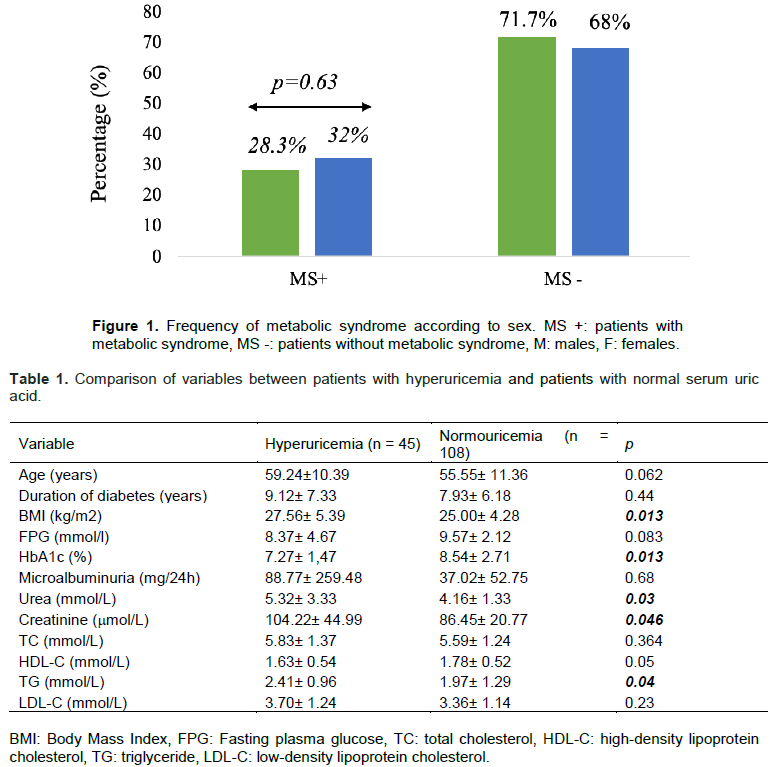
A total of 153 type 2 diabetic patients including women (65%) and 54 men (35%) were enrolled. Patients were aged between 21 and 87 years with an average of 56.63 years. The mean duration of diabetes was 8.28 ± 6.54 years. In the study population, 31% of patients had metabolic syndrome and were characterized by a predominance of women (Figure 1).
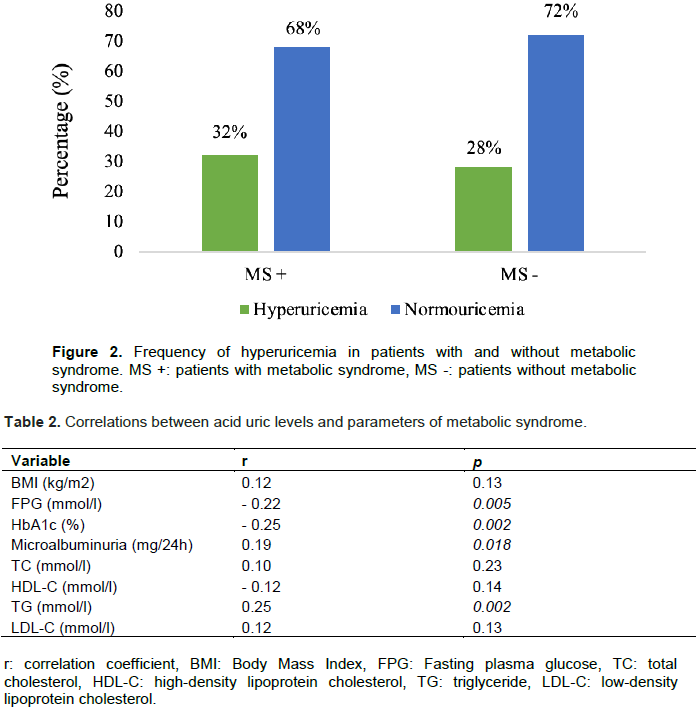
The general characteristics of the study population according to the serum uric acid concentrations are illustrated in Table 1. They found that 32% of patients with metabolic syndrome had hyperuricemia (Figure 2).
The study of the correlations between uricemia and the various components of metabolic syndrome revealed significant positive correlations between serum uric acid and various parameters such as triglyceride (r = 0.25; p = 0.002) and microalbuminuria (r = 0.19; p = 0.018). The authors also found significant negative correlations between uricemia and blood sugar as well as glycated hemoglobin levels with respectively (r = - 0.22; p = 0.005) and (r = - 0.25; 0.002). No significant correlations were found for the other parameters (p > 0.05) (Table 2).
Metabolic syndrome consists of the association in the same individual of several metabolic abnormalities which predispose the occurrence of many cardiovascular complications (Vladimír et al., 2017). In this study, we assessed the association between uricemia and metabolic syndrome in our population.
Most patients were women (sex ratio = 0.54) with an average age of 56.63 years and extremes of 21 and 87 years. Similar results have been reported in many studies (Jeandel and Kouda Zeh, 1987; Siko, 1989; Wanvoegbe et al., 2017), which once again confirms that the prevalence of type 2 diabetes increases with age (Jeandel and Kouda Zeh, 1987; Siko 1989; Diouf et al., 2013).
The predominance of women is mainly linked to the high rate of physical inactivity of women in our society, which is a risk factor for obesity and cardiovascular disease (Bouzid et al., 2011). The mean duration of diabetes was 8.28 ± 6.54 years. This long duration, which indicates a prolonged evolution of the disease, exposes patients more to the occurrence of metabolic abnormalities. The frequency of metabolic syndrome in this study was 31%. Similar results have been reported in other studies where this frequency was 21, 24.3, 33.9, 34.7, 36.3 and 37% respectively in Saudi Arabia, Tunisia, in Iran, Turkey, Jordan and Palestine (El Bilbeisi et al., 2017). These variations, although close, are mainly explained by the differences in the criteria for defining the metabolic syndrome used across the different studies.
The WHO definition criteria used in this study was the best suited to the study population composed of type 2 diabetics. This relatively high frequency of metabolic syndrome could be linked to poor food hygiene as well as a high rate of physical inactivity, which are the main risk factors.
It found that 32% of patients with metabolic syndrome had hyperuricemia. Much higher frequencies have been found in other studies (Ismail et al., 2018). Hyperuricemia is frequently observed in diabetes as well as in metabolic syndrome and this is mainly linked to the increase in renal reabsorption of uric acid secondary to hyperinsulinemia (Quinones et al., 1995; Muscelli et al., 1996; Matsuura et al., 1998).
The study of the correlations between uricemia and the components of metabolic syndrome revealed a significant positive correlation with triglyceride level (r = 0.25, p = 0.002). The association between uricemia and triglyceridemia has also been demonstrated in other similar studies (Conen et al., 2004).
Indeed, it has been reported that the association between insulin resistance, hyperuricemia and hypertriglyceridemia is linked to a deficit in glyceraldehyde-3-phosphate dehydrogenase and to a loss of its sensitivity to insulin where the increase in triglycerides is due to an accumulation of glycerol-3-phosphate (Leyva et al., 1998).
We also found a significantly higher mean BMI value in patients with hyperuricemia (p = 0.013) although the weakly positive correlation found between uricemia and BMI was not significant (r = 0.12; p = 0.13).
Likewise for total cholesterol level, a weak positive but not significant correlation was found (r= 0.10; p = 0.23).
Indeed, several epidemiological and clinical studies have shown a close correlation between hyperuricemia and obesity. In the study conducted by Masuo et al. it was shown that high concentrations of uric acid predispose to weight gain (Masuo et al., 2003).
It has also been suggested that hyperuricemia induces an alteration in the redox signaling pathways responsible for oxidative stress in adipocytes (Sautin et al., 2007) and this oxidative stress in adipose tissue is today recognized as being responsible for insulin resistance and cardiovascular disease. Finally, hyperuricemia can induce insulin resistance by causing vasodilation and an increase in blood flow, thus interfering with the action of nitric oxide which promotes glucose absorption (Khosla et al., 2005). It has also been suggested that hyperuricemia is linked to hyperinsulinemia by increased renal reabsorption of uric acid (Yoo et al., 2005; Lee et al., 2013). In contrast to these studies, the authors found negative correlation between fasting blood glucose and serum uric acid as well as glycated hemoglobin with respectively (r = - 0.22; p = 0.005) and (r = - 0.25; p= 0.002).
The association between hyperuricemia and metabolic syndrome has been demonstrated in many epidemiological studies and this hyperuricemia is considered by some authors to be a component of this syndrome. The authors have found a lower frequency of hyperuricemia in patients with metabolic syndrome than that reported in the literature.
Nevertheless, significant correlations have been highlighted between uricemia and some components of this syndrome, such as triglyceride level which is better correlated with serum uric acid concentrations compared to fasting blood sugar.
The authors have not declared any conflicts of interests.
The authors would like to thank the entire cohort of patients at Abass Ndao Hospital Center for their commitment to participate in this study, as well as the various services that helped them in the study of their patients including the Laboratory of Biochemistry of the University Hospital Fann.
REFERENCES
|
Alberti KGMM, Zimmet PZ (1998). For the WHO Consultation, definition, diagnosis and classification of diabetes mellitus and its complications; Part I: Diagnosis and classification of diabetes mellitus, Provisional report of a WHO consultation. Diabetic Medicine 15(7):539-553.
Crossref
|
|
|
|
Ames BN, Cathcart R, Schwiers E, Hochstein P (1981). Uric acid provides an antioxidant defense in humans against oxidant- and radical-caused aging and cancer: a hypothesis. Proceedings of the National Academy of Sciences 78(11):6858-6862.
Crossref
|
|
|
|
|
Bouzid C, Smida H, Kacem A, Turki Z, Salem B, Slama BC (2011). L'insuffisance rénale chez des diabétiques de type 2 Tunisiens hospitalisés: fréquence et facteurs associés. Tunisie Médicale 89(1):10-15.
|
|
|
|
|
Cheserek MJ, Shi Y, Le G (2018). Association of hyperuricemia with metabolic syndrome among university workers: sex and occupational differences. African Health Sciences 18(4):842-851.
Crossref
|
|
|
|
|
Conen D, Wietlisbach V, Bovet P, Shamlaye C, Riesen W, Paccaud F, Burnier M (2004). Prevalence of hyperuricemia and relation of serum uric acid with cardiovascular risk factors in a developing country. BMC Public Health 4(1):1-9.
Crossref
|
|
|
|
|
Diouf NN, Boye O, Soumboundou M, Gueye MW, Sawaré E, Sylla-Niang M (2013). Evaluation de l'équilibre glycémique chez les sujets âgés présentant un diabète de type 2. Revue Médicale de Madagascar 3(2):269-272.
|
|
|
|
|
El Bilbeisi A, Shab-Bidar S, Jackson D, Djafarian K (2017). The Prevalence of Metabolic Syndrome and Its Related Factors among Adults in Palestine: A MetaAnalysis. Ethiopian Journal of Health Science 27(1):77-84.
Crossref
|
|
|
|
|
Fabbrini E, Serafini M, Baric IC, Hazen SL, Klein S (2014). Effect of plasma uric acid on antioxidant capacity, oxidative stress, and insulin sensitivity in obese subjects. Diabetes 63(3):976-981.
Crossref
|
|
|
|
|
Hansel B, Giral P, Nobecourt E, Chantepie S, Bruckert E (2004). Metabolic syndrome is associated with elevated oxidative stress and dysfunctional dense high-density lipoprotein particles displaying impaired anti oxidative activity. The Journal of Clinical Endocrinololy and Metabolism 89(10):4963-4971.
Crossref
|
|
|
|
|
Hochberg MC, Smolen JS, Weinblatt ME, Weisman MH (2003). Rheumatology.3rd Ed.New York:Mosby.
|
|
|
|
|
Huang G, Xu J, Zhang T, Cai L, Liu H, Yu X, Wu J (2020). Hyperuricemia is associated with metabolic syndrome in the community very elderly in Chengdu. Scientific Reports 10(1):1-7.
Crossref
|
|
|
|
|
Ishizaka N, Ishizaka Y, Toda E, Nagai R, Yamakado M (2005). Association Between Serum Uric Acid, Metabolic Syndrome, and Carotid Atherosclerosis in Japanese Individuals. Arteriosclerosis Thrombosis and Vascular Biology 25(5):1038-1044.
Crossref
|
|
|
|
|
Ismail EM, Elbadawi N, Hassan D (2018). Uric Acid as a Biomarker of Metabolic Syndrome in Sudanese Adults. International Journal of Biochemistry and physiology 3(4):000137.
Crossref
|
|
|
|
|
Jeandel P, Kouda Zeh A (1987). Le diabète sucré au Cameroun. Etude prospective de 203 sujets. Médecine d'Afrique noire 34(10):861-873.
|
|
|
|
|
Khosla UM, Zharikov S, Finch JL, Nakagawa T, Roncal C, Mu W, Krotova K, Block ER, Prabhakar S, Johnson RJ (2005). Hyperuricemia induces endothelial dysfunction. Kidney International 67(5):1739-1742.
Crossref
|
|
|
|
|
Lee D, Choi WJ, Oh JS, Yi MK, Han SW, Yun JW, Han SH (2013). The relevance of hyperuricemia and metabolic syndrome and the effect of blood lead level on uricacid concentration in steel making workers. Annals of Occupational and Environmentalmedicine 25(1):1-7.
Crossref
|
|
|
|
|
Lee L, Sanders RA (2012). Metabolic Syndrome. Pediatrics in Review 33(10):459.
Crossref
|
|
|
|
|
Leyva F, Wingrove C, Godsland I, Stevenson J (1998). The glycolytic pathway to coronary heart disease: A hypothesis. Metabolism 47(6):657-662.
Crossref
|
|
|
|
|
Lorenzo C, Williams K, Hunt KJ, Haffner SM (2007). The National Cholesterol Education Program. Adult Treatment Panel III, International Diabetes Federation, and World Health Organization definitions of the metabolic syndrome as predictors of incident cardiovascular disease and diabetes. Diabetes Care 30(1):8-13.
Crossref
|
|
|
|
|
Masuo K, Kawaguchi H, Mikami H, Ogihara T, Tuck Ml (2003). Serum uricacid and plasma norepinephrine concentrations predict subsequent weight gain and blood pressure elevation. Hypertension 42(4):474-480.
Crossref
|
|
|
|
|
Matsuura F, Yamashita S, Nakamura T, Nishida M, Nozaki S, Funahashi T, Matsuzawa Y (1998). Effect of visceral fat accumulation on uric acid metabolism in male obese subjects: visceral fat obesity is linked more closely to overproduction of uric acid than subcutaneous fat obesity. Metabolism 47(8):929-933.
Crossref
|
|
|
|
|
Muscelli E, Natali A, Bianchi S, Bigazzi R, Galvan AQ, Sironi AM, Frascerra S, Ciociaro D, Ferrannini E (1996). Effect of insulin on renal sodium and uricacid handling in essential hypertension. American Journal of Hypertension 9(8):746-752.
|
|
|
|
|
Quinones Galvan A, Natali A, Baldi SI, Frascerra SI, Sanna GI, Ciociaro DE, Ferrannini E (1995). Effect of insulin on uricacidexcretion in humans. American Journal of Physiology-Endocrinology and Metabolism 268(1):1-5.
Crossref
|
|
|
|
|
Sautin YY, Nakagawa T, Zharikov S, Johnson RJ (2007). Adverse effects of the classic antioxidant uric acid in adipocytes: NADPH oxidase-mediated oxidative/nitrosative stress. American Journal of Physiology-Cell Physiology 293:C584-C96.
Crossref
|
|
|
|
|
Siko A (1989). Prise en charge thérapeutique du diabète sucré chez l'adulte à l'hôpital Yalgado Ouédraogo : à propos de 65 cas [Thèse de doctorat en Médecine] Ouagadougou : Université de Ouagadougou Faculté de Médecine.
|
|
|
|
|
Sung KC, Kim BJ, Kim BS, Kang JH, Lee MH (2004). In normoglycemic Koreans, insulin resistance and adipocity are independently correlated with high blood pressure. Circulation Journal 68(10):898-902.
Crossref
|
|
|
|
|
ViswanathanI M, Deepa M (2006). Syndrome métabolique dans les pays en développement. Diabetes Voice;51 (Numéro spécial):15-17.
|
|
|
|
|
Vladimír K, Ružena S, Zuzana B, Tatiana S, Viktor B, Štefan B (2017). Monothérapie du syndrome métabolique expérimental : Etude des effets cardiovasculaires. Interdisciplinary Toxicology 10(3):86-92.
|
|
|
|
|
Wanvoegbe FA, Agbodande KA, Alassani A, Gninkoun J, Kerekou A, Azon-Kouanou A, Amoussou-Guenou D, Djrolo F, Zannou M, Houngbe F (2017). Hyperuricémie chez les diabétiques de type 2 à Cotonou: prévalence et facteurs associés. Journal de la Société de Biologie Clinique 27:5-9.
|
|
|
|
|
Wilson PW, D'Agostino RB, Parise H, Sullivan L, Meig JB (2005). Metabolic syndrome as a precursor of cardiovascular disease and type 2 diabetes mellitus. Circulation 112(20):3066-3072.
Crossref
|
|
|
|
|
Yoo TW, Sung KC, Shin HS, Kim BJ, Kim BS, Kang JH, Lee MH, Park JR, Kim H, Rhee EJ, Lee WY (2005). Relationship between serum uric acid concentration and insulin resistance and metabolic syndrome. Circulation Journal 69(8):928-933.
Crossref
|
|
|
|
|
Zhang C, Liu R, Yuan J, Cui J, Hu F, Yang W, Zhang Y, Yang C, Qiao S (2016). Gender-related differences in the association between serum uric acid and left ventricular mass index in patients with obstructive hypertrophic cardiomyopathy. Biology of Sex Differences 7(1):1-2.
Crossref
|
|