ABSTRACT
The aim of this study was to determine the correlation between glycated hemoglobin and blood sugar levels in diabetic subjects carried out in Abidjan. This cross-sectional study included 100 patients with diabetes monitored, for three months, for whom glycated blood glucose and hemoglobin were performed, this after informed consent of the patients. Pearson and Spearman correlation tests were used, at the 5% threshold. The patients with normal HbA1C and normal blood glucose accounted for 55.34 and 32%, respectively. A sedentary lifestyle and body mass index > 25 kg/m² were associated with a significant increase in the risk of increased blood glucose and HbA1C. The presence of a complication was associated with a 3.06-fold higher risk of high glycated hemoglobin (p= 0.0073), while blood glucose was not significantly associated with the onset of complications. Glycated hemoglobin was significantly correlated with blood glucose with a correlation coefficient of 0.4412 (p 0.0001). In multivariate analysis, hyperglycemia was significantly associated with alcohol consumption and non-compliance with antidiabetic treatment. Poor compliance was significantly associated with increased glycated hemoglobin (>7%) and tobacco consumption. The glycated hemoglobin was highly correlated with blood sugar, and was found to be a better predictor of diabetes complications than glycemia.
Key words: Diabetes mellitus, glycated hemoglobin, blood sugar, Abidjan, Côte d’Ivoire.
The complications of diabetes are influenced not only by the duration of diabetes but also by the average level of chronic glycemia which is measured most reliably with glycated hemoglobin (HbA1C) assay (Lenters-Westra and Slingerland, 2008; ADA, 2009). The most common type of diabetes is type 2, long-asymptomatic, which usually occurs after a long period of insulin resistance and metabolic disorders (Colette and Monnier, 2010).
In 2010, in sub-Saharan Africa, more than 12 million people were living with diabetes and 330,000 people died from related complications (ADA, 2009, 2011). In diabetes, dietary measures, most of which are associated with drug treatments, are essential for a good patient balance (Colette and Monnier, 2010). The aim of these measures is to reduce insulin resistance, glycemic, lipid and blood pressure disturbances, and to prevent the disease from worsening (Verma et al., 2006; Colette and Monnier, 2010). The simple determination of blood glucose levels on a periodic basis at the time of checkups prior to visits to the medical practitioner cannot provide a correct picture of the long-term control of diabetic disease. To overcome this deficit, biochemical markers, including HbA1C, are used to help assess the glycemic balance of patients (Shubrook, 2010).
The HbA1C assay is used to estimate the mean level of blood sugar in the two months preceding the baseline (Kilpatrick, 2008). The study of HbA1C and blood glucose was carried out in numerous studies in both Caucasian and Black subjects (Kilpatrick, 2008; Shubrook, 2010; Ercan, 2014; Zendjabil, 2015). Thus, Gillery (2013) in France and Selvin et al. (2010) in the United States, made it possible to study cardiovascular risk in diabetic subjects and even to propose new diagnostic methods for diabetes. In North Africa, Zendjabil (2015) assessed cardiovascular risk in diabetic patients using the HbA1C assay. However, very few studies on HbA1C and glycaemia were carried out in Côte d'Ivoire. The objective of this work was to study the correlation between HbA1C and glycemia in diabetic subjects in a private health facility in the municipality of Yopougon.
This is a descriptive and analytical cross-sectional study involving 100 patients, recruited for diabetology consultation at a private health facility in Yopougon (Abidjan), which lasted 3 months. Patients with diabetes, regardless of gender, with an age ≥18 years, who accepted the sample and gave informed consent, were selected for blood glucose and HbA1C. Patients with other associated conditions such as high blood pressure were not selected. A questionnaire was used to study certain epidemiological and clinical parameters such as, sedentary behaviour, body mass index (BMI), smoking and alcohol consumption, regularity of treatment follow-up, type of treatment, the quality of adherence to treatment, and the occurrence or non-occurrence of complications. Measurements of weight and height were made according to the WHO (2006) standard, in indoor garment, without footwear. The weight was obtained using a mechanical person’s scale (make “SEVERIN PW 7010-Tasteful Technology”), with an accuracy of 0.1 kg.
Height was measured using a height gauge (make “SECA 206”) with an accuracy of 0.1 cm. Overweight and obesity were determined by calculating the BMI [BMI (kg/m2) = Weight/Size 2], which are defined respectively by BMI > 25 and 30 kg/m2. The samples were taken from people with diabetes on an empty stomach the day before. The blood was collected in two tubes: one containing both an anti-glycolytic and an anticoagulant, and another containing ethylene diamine tetra-acetic acid (EDTA). Each tube contained 5 mL of blood collected. Glycated haemoglobin was determined by immunoturbidimetry method and blood glucose, by classical glucose-oxidase-peroxidase enzymatic method on a Cobas E 400 automaton. The reference values for HbA1C were 6.5% and for fasting blood glucose between 0.60 and 1.10 g/L (ADA, 2011). The samples were taken with informed consent from the patients. This study was approved by the Ivoirian Ethics Committee for Clinical Research (Approval number: 141/MSHP/CNER/01/2017). The analysis of the variables was done by the Pearson and Spearman correlation tests, with a significance threshold of 5%.
The sex ratio was 1.17 (1.17 men for a woman; that is, 54 men for 46 women). The proportion of type 2 diabetics was the highest at 96% and that of type 1 diabetic was weak at 4%.
Overweight patients accounted for 33% and obese subjects 41% of patients. The proportion of overweight and obese subjects was therefore 74%. Sedentary lifestyle was one of the most important risk factors and was observed in 59% of patients. Alcohol consumption was observed in 44% of patients and we recorded 19% of patients consuming tobacco. The healthy diet was part of the treatment of almost all patients (99% of cases). The treatment was regularly followed in 94% of the diabetic patients.
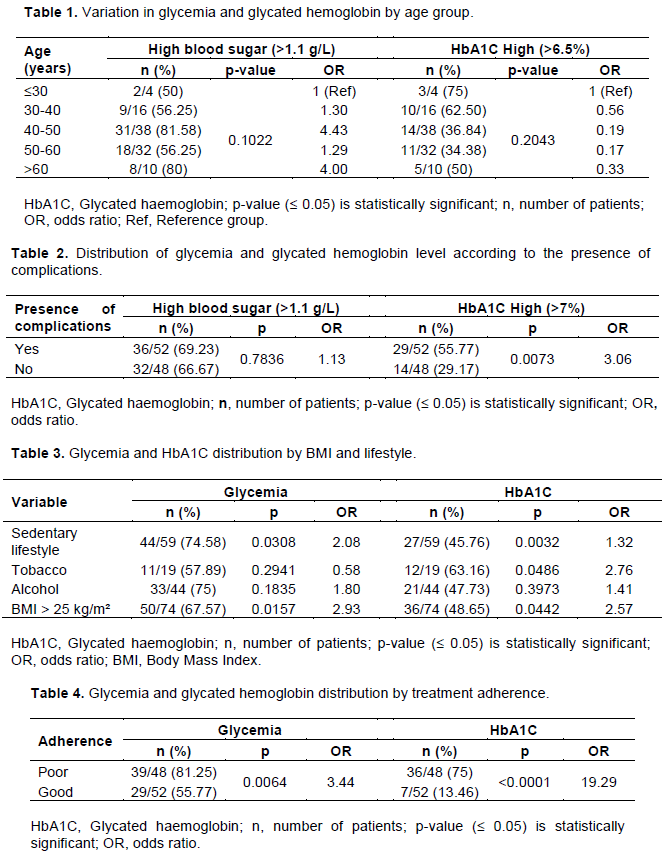
Table 1 shows that patients had an average age of 49.2±10.96 years with extremes of 13 and 82 years. The high prevalence of age was between 40 and 50 years (81.58%).
Table 2 shows the distribution of blood glucose and HbA1C by presence of complications. Blood glucose was not significantly associated with the occurrence of complications. The presence of a complication was associated with a 3.06 times higher risk of high HbA1C (Table 2).
The correlation curve between HbA1C and glycemia is as shown in Figure 1. HbA1C was significantly correlated with blood glucose. The correlation coefficient r was 0.4412 and a p0.0001.
Table 3 shows the distribution of blood glucose and HbA1C by BMI and lifestyle. A sedentary lifestyle and BMI > 25 kg/m² were associated with a significant increase in the risk of increased blood glucose and HbA1C.
Table 4 shows the distribution of blood glucose and HbA1C by treatment adherence. Poor adherence to treatment was associated with an increased risk of high mean blood glucose and high HbA1C.
Table 5 shows analysis of hyperglycemia and HbA1C with BMI, lifestyle, treatment and complications. Hyperglycemia and HbA1C were significantly associated with poor adherence to antidiabetic treatment. The type of treatment and the degree of obesity did not influence changes in glycated blood glucose and hemoglobin.
Variation by age group
The present study is the first concerning correlation between HbA1C and glycemia in Abidjan. The age of most patients was between 40 and 50 years old, with an average of 49.2±10.96 years and extremes of 13 and 82 years (Table 1), and a sex ratio of 1.17. This distribution was comparable to that described by Qvist et al. (2008) which reported the mean age for all participants was 45.5. Mohammed et al. (2018) also showed that most affected age group by diabetes is between 45 and 55 years in a Tlemcen population in Algeria. The high proportion of subjects aged 40 to 50 justifies the recommendation of screening in subjects aged 45 and over (CDA, 2008). Our results showed that glycemia and HbA1C were not age-dependant. Several studies, including that of Verma et al. (2006) and Bouzid et al. (2011) previously reported in diabetic subjects that age was not associated with variation in HbA1C level, duration of diabetes, fasting blood glucose, glycated protein or glycated albumin. However, young age was cited as a factor associated with poor glycemic follow-up (Qvist et al., 2008), as well as old age (Wahba and Chang, 2007). According to the results of many longitudinal and cross-sectional studies, it has been demonstrated that the earliest detectable abnormality in non-insulin dependent diabetes mellitus (NIDDM) is impairment in the body’s ability to respond to insulin (Lenters-Westra and Slingerland, 2008).
Occurrence of complications
Glycation of proteins affords an index for glycemic control, and moreover, literatures reported that increased glycated proteins are linked to complications like nephropathy, cardiovascular diseases, and retinopathy among others (Megerssa and Tesfaye, 2015). In our study, glycated hemoglobin was found to be a good test for predicting complications (OR=3.06; p= 0.0073) (Table 2) and was reinforced by other work. Nakagami et al. (2017) have shown the risks of incident retinopathy and diabetic retinopathy were positively, continuously, and independently associated with HbA1C and fasting plasma glucose (FPG) levels in their cohort of Japanese participants without a previous history of diabetes. Furthermore, the adjusted hazard ratio for retinopathy were significantly higher in participants with an HbA1C level ≥6.5% or FPG level ≥7.0 mmol/L at baseline, relative to participants in the lowest categories of these variables (Nakagami et al., 2017). Also, Stratton et al. (2000) in the United Kingdom Prospective Diabetes Study Group (UKPDS) work on type 2 diabetes showed that the risk of myocardial infarction and microvascular complications decreased by 14 and 37%, respectively for any 1% decrease in HbA1C. Thus, the reduction of Hba1c, in the long term, led to a decrease in the risk of complications. Glycemia, on the other hand, showed no significant variation depending on whether or not complications occurred.
HbA1C and glycemia correlation
In the ADAG (HbA1C -Derived Average Glucose) study (Klonoff and Aimbe, 2014), conducted in type 1 and 2 diabetics and non-diabetic volunteers, the correlation between HbA1c and glycemia levels was higher (R 2 = 0.84) than the one found (R2 = 0.44) (Figure 1). Likewise, Mohammed et al. (2018) showed a moderate positive correlation (r = 0.68) between the values ​​of HbA1C and blood glucose in diabetic patients. This could be due to the fact that we performed a single dose of HbA1C and glycemia per patient, while in the ADAG cohort study, glycemia was measured before and after each meal and at bedtime.
This correlation seemed linear for all glycemia values. According to Bouzid et al. (2011) HbA1C values are correlated with fasting glycemia values and a 1% increase in HbA1c would approximate an increase of 18 mg/dl for fasting blood glucose found from the equation of the regression curve. Through irreversible formation and accumulation in red blood cells over 120 days of life, HbA1C accurately reflects changes in the glycemic balance over the previous three months. For example, glycated hemoglobin is the best diagnostic and follow-up parameter for diabetic disease, as it provides accurate information on long-term changes in glycemic balance, while venous and capillary glycemia measure the glycemic balance used in the short term and in emergency situations (Zafar et al., 2019). Thus, the correlation HbA1C/blood glucose level allows better control of glycemia (Mohammed et al., 2018).
Blood glycemia and HbA1C distribution by BMI and lifestyle
The vast majority of patients were physically inactive and had a higher than normal BMI, very often obese (Table 3). Our results showed that lack of physical activity increased the risk of obesity, hyperglycemia and HbA1C by more than 7% (Table 3). According to Rey-Lopez et al. (2008), a sedentary lifestyle is a factor of obesity. Physical inactivity and overweight may be responsible for significant changes in blood glucose and HbA1C. Studies showed that physical activity is significantly associated with a reduction in the risk of type 2 diabetes and that type 2 diabetes gradually settles in obese subjects (BMI 30) over the years (Gill and Cooper, 2008; Rey-Lopez et al., 2008).
It would be useful to advise diabetic patients to have a better quality of life compliance with lifestyle factors and diabetes self-management (Bennich et al., 2019). Thus, the practice of a regular physical activity, when combined with a hygienic-dietetic diet, would be effective in combating obesity, diabetes and its complications (Rey-Lopez et al., 2008; Adam et al., 2018; Seuring et al., 2019).
Multivariate analysis
Poor adherence to treatment was associated with an increased risk of high mean blood glucose and high HbA1C (Table 4).
Tobacco use was an independent predictor of increased HbA1C. Alcohol consumption was associated with a significant increase in the risk of hyperglycemia (Table 5). The relationship between alcohol consumption and insulin resistance results in a U-shaped curve. Another hypothesis is that smoking could influence the formation of HbA1c indirectly, independent of its effect resulting in elevated HbA1c levels (Jae et al., 2015). Our results could be attributed to alcohol consumption, a lifestyle parameter as important as smoking, was independently and negatively correlated with HbA1c levels, consistent with previous reports. Previous studies suggested that moderate alcohol intake might have protective effects on glucose metabolism by lowering insulin resistance (Greenfield et al., 2004; Bonnet et al., 2012). We recorded 48% of patients with poor adherence to treatment. The risk of hyperglycemia was 3.44 times higher with treatment non-compliance. Poor adherence to treatment was associated with a higher risk of high glycated hemoglobin (>7%). Poor adherence to treatment was also an independent predictor of hyperglycemia and an increase in HbA1C. The risk was even higher for glycated hemoglobin compared to blood glucose (103.02 vs. 5.79). Our results were consistent with those of Kumar et al. (2010) which reported that HbA1C had better specificity but less sensitivity to glycemia. This would justify some authors advocating reducing HbA1C to 6.1% instead of 6.5%. We can suggest as Razi et al. (2018) the necessity of determining the HbA1C cutoffs for detecting diabetes or prediabetes in the population, likewise the combination of these HbA1C cutoffs with fasting glycemia levels are required to determine diabetes and prediabetes more accurately, in a preventive purpose. Apart from diabetes, glycated hemoglobin has also proven to be a real marker of cardiovascular risk, since it has been associated with determination of serum sialic acid as risk factors in patients with myocardial infarction, who are non-diabetic (Basha and Kasi, 2019).
Our study showed that HbA1C was highly correlated with glycemia. Moreover, HbA1C was shown to be a better predictor of diabetes complications than glycemia. Thus, we recommend that the measurement of HbA1C should be integrated in health check of any person aged 40 or over, likewise organize awareness campaigns, screening and information of populations on metabolic diseases, especially diabetes. Future studies are needed with a larger sample of subjects to allow the use of this marker in the prevention of diabetes complications.
The authors have not declared any conflict of interests.
The authors thank the team of Endocrinology and Diabetology Department of Teaching Hospital of Yopougon, in Abidjan.
REFERENCES
|
ADA (2009). Diagnosis and classification of diabetes mellitus. Diabetes Care 32(1):S62-67.
Crossref
|
|
|
|
ADA (2011). Diagnosing diabetes with glucose criteria: worshipping a false God. Diabetes Care 34:524-526.
Crossref
|
|
|
|
|
Adam L, O'Connor C, Garcia AC (2018). Evaluating the impact of diabetes self-management education methods on knowledge, attitudes and behaviours of adult patients with type 2 diabetes mellitus. Canadian Journal of Diabetes 42(5):470-477.
Crossref
|
|
|
|
|
Basha SYC, Kasi HK (2019). Role of glycated hemoglobin and sialic acid in non-diabetics having a myocardial infarction: A case-control study in the people from north coastal Andhra Pradesh. Indian Journal of Medical Biochemistry 23(3):350-353.
Crossref
|
|
|
|
|
Bennich BB, Munch L, Egerod I, Konradsen H, Ladelund S, Knop FK, Vilsbøll T, Roder M, Overgaard D (2019). Patient assessment of family function, glycemic control and quality of life in adult patients with type 2 diabetes and incipient complications. Canadian journal of diabetes. 43(3):193-200.
|
|
|
|
|
Bonnet F, Disse E, Laville M, Mari A, Hojlund K, Anderwald CH, Piatti P, Balkau B; RISC Study Group (2012). Moderate alcohol consumption is associated with improved insulin sensitivity, reduced basal insulin secretion rate and lower fasting glucagon concentration in healthy women. Diabetologia 55(12):3228-3237.
Crossref
|
|
|
|
|
Bouzid K, Bahlous A, Hamdane Y, Chelbi A, Mohsni A, Zerelli L, Hamida B A, Abdelmoula J (2011). Dosage de l'hémoglobine glyquée dans une population tunisienne: valeurs de référence chez les non diabétiques et corrélations avec les glycémies à jeun chez les diabétiques. Immuno-analyse et Biologie Spécialisée 26:19-22.
Crossref
|
|
|
|
|
CDA (2008). Guidelines for the prevention and treatment of diabetes in Canada. Canadian Journal of Diabetes 32(1):S1-S200.
|
|
|
|
|
Colette C, Monnier L (2010). Diététique des états diabétiques. In : Monnier L. Diabétologie. Issy-les-moulineaux : Elsevier Masson SAS. p. 18.
Crossref
|
|
|
|
|
Ercan S, Yücel N, Orçun A (2014). The Comparison of Glycated Hemoglobin and Homeostasis Model Assessment Values to 30, 60 and 90-Min Glucose Levels During OGTT in Subjects with Normal Glucose Tolerance. Journal of Medical Biochemistry 33(3):237-244.
Crossref
|
|
|
|
|
Gill JM, Cooper AR (2008). Physical activity and prevention of type 2 diabetes mellitus. Sports Medicine 38(10):807-824.
Crossref
|
|
|
|
|
Gillery P (2013). Le dosage de l'hémoglobine A1C en 2013. Medecine des maladies métaboliques 7(3):256-261.
Crossref
|
|
|
|
|
Greenfield JR, Samaras K, Hayward CS, Chisholm DJ, Campbell LV (2004). Beneficial postprandial effect of a small amount of alcohol on diabetes and cardiovascular risk factors: modification by insulin resistance. The Journal of Clinical Endocrinology and Metabolism 90(2):661-672.
Crossref
|
|
|
|
|
Jae WH, Cheol RK, Jung HN, Kyun SK, Byoung DR, Dong JK (2015). Association between Self- Report Smoking and Hemoglobin A1c in a Korean Population without Diabetes: The 2011-2012 Korean National Heath and Nutrition Examination Survey. PLoS ONE 10(5):e0126746.
Crossref
|
|
|
|
|
Kilpatrick ES (2008). Haemoglobin A1C in the diagnosis and monitoring of diabetes mellitus. Journal of Clinical Pathology 61(9):977-982.
Crossref
|
|
|
|
|
Klonoff DC, Aimbe F (2014). ADAG study group data links A1C levels with empirically measured blood glucose values - New treatment guidelines will now be needed. Journal of Diabetes Science and Technology 8(3):439-443.
Crossref
|
|
|
|
|
Kumar PR, Bhansali A, Ravikiran M (2010). Utility of glycated hemoglobin in diagnosing type 2 diabetes mellitus: a community-based study. The Journal of Clinical Endocrinology and Metabolism 95(6):2832-2835.
Crossref
|
|
|
|
|
Lenters-Westra E, Slingerland RJ (2008). Hemoglobin A1C determination in the A1C-Derived Average Glucose (ADAG) study. Clin.Chem. Lab. Med 46(11):1617-23.
Crossref
|
|
|
|
|
Megerssa YC, Tesfaye DY (2015). Glycated proteins: Clinical utility and analytical approaches. African Journal of Biochemistry Research 9(2):18-25.
Crossref
|
|
|
|
|
Mohammed-Nadjib R, Amine G, Amine HM (2018). Glycated hemoglobin assay in a Tlemcen population: Retrospective study. Diabetes and Metabolic Syndrome: Diabetes and Metabolic Syndrome 12(6):911-916.
Crossref
|
|
|
|
|
Nakagami T, Takahashi K, Suto C, Oya J, Tanaka Y, Kurita M, Isago C, Hasegawa Y, Ito A, Uchigata Y (2017). Diabetes diagnostic thresholds of the glycated hemoglobin A1c and fasting plasma glucose levels considering the 5-year incidence of retinopathy. Diabetes Research and Clinical Practice 124:20-29.
Crossref
|
|
|
|
|
Qvist R, Ismail IS, China K, Muniandy S (2008). Use of glycated hemoglobin (HbA1C) and impaired glucose tolerance in the screening of undiagnosed diabetes in the Malaysian population. Indian Journal of Clinical Biochemistry 23(3):246-249.
Crossref
|
|
|
|
|
Razi F, Khashayar P, Ghodssi-Ghassemabadi R, Mehrabzadeh M, Peimani M, Bandarian F, Nasli-Esfahani E (2018). Optimal glycated haemoglobin cut off point for diagnosis of type 2 diabetes in Iranian adults. Canadian Journal of Diabetes 42(6):582-587.
Crossref
|
|
|
|
|
Rey-Lopez JP, Vicente-Rodriguez G, Biosca M, Moreno LA (2008). Sedentary behavior and obesity development in children and adolescents. Nutrition, Metabolism and Cardiovascular Diseases 18(3):242-251.
Crossref
|
|
|
|
|
Selvin E, Steffes MW, Zhu HMK, Wagenknecht L, Pankow J, Coresh J, Brancati FL (2010). Glycated hemoglobin, diabetes, and cardiovascular risk in non diabetic adults. New England Journal of Medicine 362(9):800-811.
Crossref
|
|
|
|
|
Seuring T, Marthoenis, Rhode S, Rogge L, Rau H, Besançon S, Zufry H, Sofyan H, Vollmer S (2019). Using peer education to improve diabetes management and outcomes in a low-income setting: a randomized controlled trial. Trials 20(1):548.
Crossref
|
|
|
|
|
Shubrook J (2010). Risks and benefits of attaining HbA1C goals : examining the evidence. The Journal of the American Osteopathic Association 110(7):7-12.
|
|
|
|
|
Stratton IM, Adler AI, Neil HA, Matthews DR, Manley SE, Cull CA, Hadden D, Turner RC, Holman RR (2000). Association of glycaemia with macrovascular and microvascular complications of type 2 diabetes (UKPDS 35): prospective observational study. BMJ. 321(7258):405-412.
Crossref
|
|
|
|
|
Verma M, Paneri S, Badi E, Raman PG (2006). Effect of increasing duration of diabetes mellitus type 2 on glycated hemoglobin and insulin sensitivity. Indian Journal of Clinical Biochemistry 21(1):142-146.
Crossref
|
|
|
|
|
Wahba H, Chang Y (2007). Factors associated with glycemic control in patients with type 2 diabetes mellitus in rural areas of the United States. Insulin 2(3):134-141.
Crossref
|
|
|
|
|
World Health Organization (WHO) (2006). Child growth standards, methods and development.
|
|
|
|
|
Zafar MI, Mills KE, Zheng J, Regmi A, Hu SQ, Gou L, Chen LL (2019). Low-glycemic index diets as an intervention for diabetes: a systematic review and meta-analysis. The American Journal of Clinical Nutrition 110(4):891-902.
Crossref
|
|
|
|
|
Zendjabil M (2015). The glycated hemoglobin: indication, interpretation and limitations. In Annales Pharmaceutiques Françaises 73(5):336-339.
Crossref
|
|