Full Length Research Paper

ABSTRACT
Measles is a highly contagious viral disease caused by morbillivirus, a member of the Paramyxoviridae family, of which humans are the only reservoirs. Person-to-person transmission occurs via aerosolized droplets and infected people's throat secretions. The aim of study is to identify major gaps and assess the trend of reporting measles disease, the positivity rate of measles samples, identify the age group most affected, and provide evidence for decision-makers. Retrospective record data from 2013 to 2017 was extracted from Ethiopian Public Health Institute and reviewed. Cross-sectional descriptive data analysis was performed by time, place, and person variables using Microsoft Excel, and the result were presented in tables and graphs. If there are more than three confirmed measles, there is an outbreak, if there are five or more suspected cases, there is a suspected outbreak based on case definition. Between 2013 and 2017, a total of 400 cases were reported throughout the region. 52.2% (209) were male, and the median age was 6 years old, 222 (55.5%) were laboratory-confirmed measles cases. 317 (79.25%) had no information about their vaccination status, 27 (6.75%) were vaccinated, and the remaining 56 (14% were not vaccinated). The highest positivity rate was observed in the age group 5-15years old 30 (51%) during 2013. Measles remains a major public health concern, primarily affecting children aged 5 to 14 in the Afar region’s districts. The number of laboratory-confirmed measles cases varies by year and season. The surveillance system should be strengthened through training, particularly among data managers and laboratory health personnel.
Key words: Measles, public health surveillance, data analysis, Ethiopia.
INTRODUCTION
Measles is a highly contagious viral disease caused by morbillivirus, a member of the Paramyxoviridae family, of which humans are the only reservoirs. Person-to-person transmission occurs primarily through aerosolized droplets or direct contact with infected people's nasal and throat secretions. When the measles virus infects a non-immune population, nearly everyone becomes infected and develops clinical illness. Malnourished children are more likely to develop complications and die from this infection (WHO, 2015).
Measles has an incubation period of 10 to 12 days (Okonko et al., 2009). Measles is still one of the vaccine-preventable diseases that cause significant mortality and morbidity in developing countries. Infants and adults are more severely affected than children, and viral replication or bacterial supper infection complications include otitis media, pneumonia, larygotracheobronchitis, diarrhea and blindness (Goitom et al., 2022).
Global measles control has been extremely effective. Following the implementation of the 2001 World Health Organization (WHO) member states goal of 50% measles mortality reduction by 2005, an estimated 60% reduction in measles-associated mortality was achieved worldwide, with a 75% reduction in the African region (Masresha et al., 2009; Goodson et al., 2011; Getahun et al., 2017; Asmare et al., 2022). Before the introduction of measles vaccination in Africa, measles was primarily a disease affecting young children, and 1 million cases were reported annually. In urban areas, measles epidemics occurred every 1 to 2 years, and the median age of cases was 1.5 to 2.5 years; in rural areas, outbreaks occurred less frequently, and the median age was 2.5 to 5.0 years (Goodson et al., 2011).
Ethiopia included measles vaccination in its routine extended program of immunization (EPI) in 1980, with the first dose administered at 9 months of age (Getahun et al., 2017). The overall immunization coverage in Ethiopia was 38.7, 36.55, 51.8, 67.1 and 66.9% for 2000, 2005, 2011, 2016 and 2019, respectively (Asmare et al., 2022). In 2013, an estimated 21.5 million children were not immunized against measles at the age of nine months. More than 60% were from India (6.4 million), Nigeria (2.7 million), Pakistan (1.7 million), Ethiopia (1.1 million), Indonesia (0.7 million), and the Democratic Republic of the Congo (0.7 million). More than 70% of global measles-related deaths occurred in these six countries in 2013, indicating that developing countries were the most affected (Wolters et al., 2017). Although vaccination coverage in Ethiopia is increasing year after year, the country continues to report a higher number of measles cases and outbreaks in all regional states and city administrations.
According to the WHO, Ethiopia is experiencing an ongoing measles outbreak, having reported over 14,000 confirmed cases in 2014 alone (World Health Assembly, 65. (2012), and being one of the world countries that experienced large outbreaks in 2009 and 2010, according to the CDC report (Minal et al, 2016). Measles is one of Ethiopia's nationally immediately notifiable diseases (Munira et al., 2018), and all health facilities (private and public) are required to report cases to the next level public health agency using the case definitions outlined earlier. Clinicians (internists, general practitioners, nurses, and health officers) reported suspected measles cases to the Ethiopian Public Health Institute for laboratory analysis using a case-based reporting form (Masresha et al., 2009).
The Ethiopian Public Health Institute is mandated by ministerial council regulations to conduct surveillance and laboratory investigations on epidemic-prone diseases such as measles (Mitiku et al., 2011). The aim of the measles case-based surveillance report analysis is to assess the trend of reporting measles cases, measure the positivity rate of measles samples, identify the age group most affected, and provide evidence for decision-makers.
METHODOLOGY
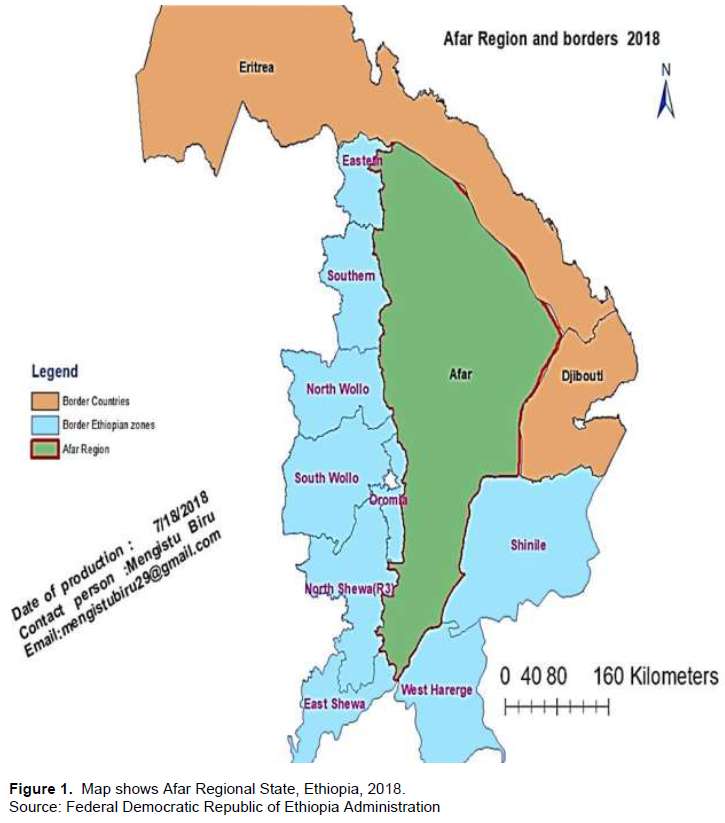
Measles surveillance data was analyzed from the Afar region. Afar is a regional state in Ethiopia. It is Ethiopia's lowest point and one of the lowest in Africa. Afar, the coordinates are 14° 7' 48" N latitude and 40° 8' 24" E longitude.
The region is 1600 m above sea level, has a total area of 72,053 km2, and is divided into five zones. Afar Regional State is in northeast Ethiopia, bordered by Eritrea to the north and northeast and Djibouti to the east (Figure 1). The total population of the Afar region was estimated to be 1.812 million (2017), with 811,776 females and 1009,284 males. Afar is one of four classified regions. Arc Geographic Information System (GIS) version 10.2 was used to depict the study area.
A retrospective measles case-based surveillance data record review was conducted from 2013 to 2017, and the data were extracted from the national measles and polio laboratory. Microsoft Excel was used for cross-sectional descriptive data analysis by time, place, and person variables and the result were presented in tables and graphs.
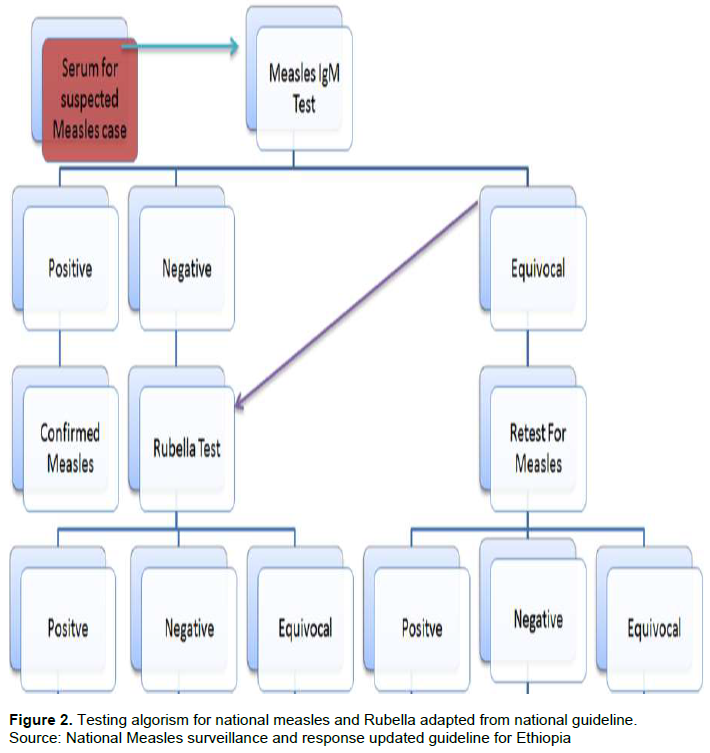
Data was cleared and checked for duplication using the patient's name, gender, age, residence area, date of onset, date seen at the health facility, and date of sample collection. Age, gender, year of the report, IgM result, and vaccination status analysis were used to categorize the data. Suspected measles case was tested according to the testing algorism for measles and rubella suspected cases as shown in Figure 2. A positive RT-PCR result or positive IgM result in patients with rash and with a history of travel in a measles endemic area or with an epidemiological link to a confirmed case are diagnostic for measles infection. Sero conversion, or a fourfold increase of measles IgM in a patient with rash and no history of recent MMR vaccination, is also diagnostic for measles. Negative results by RT-PCR and negative IgM-class antibody detection may not be sufficient to rule out measles infection in some cases, particularly if the specimen for PCR was collected later than 7 days after symptom onset (Fatiregun et al, 2015).
Suspected measles is defined as any person with fever and a maculopapular (no vesicular) generalized rash and cough, coryza or conjunctivitis (red eyes) or any person in whom a clinician suspects measles: According to the national guideline (Munira et al., 2018), we further classified the suspected measles cases collected through surveillance into the following categories.
Laboratory confirmed cases are suspected measles cases with laboratory results that show measles IgM positivity. Those who live in the same or a nearby district as a laboratory-confirmed case where there is a likelihood of transmission; the onset of the rash of the two cases occurring within 30 days of one another; and are linked (in place, person, and time) to the laboratory-confirmed case are considered to be epidemiologically linked cases of measles.
A discarded measles case is a suspected measles case that lacks serologic evidence of a measles virus infection after an adequate investigation that includes a blood specimen collected within the appropriate time frame. A person who has received one dose of MCV1 is considered to be immunized against measles antigen.
If there are three or more measles laboratory-confirmed cases, there is an outbreak of measles; and if there are five or more suspected measles cases, there is a suspected outbreak of measles for a particular district for the last four weeks, according to the national measles guideline.
RESULTS
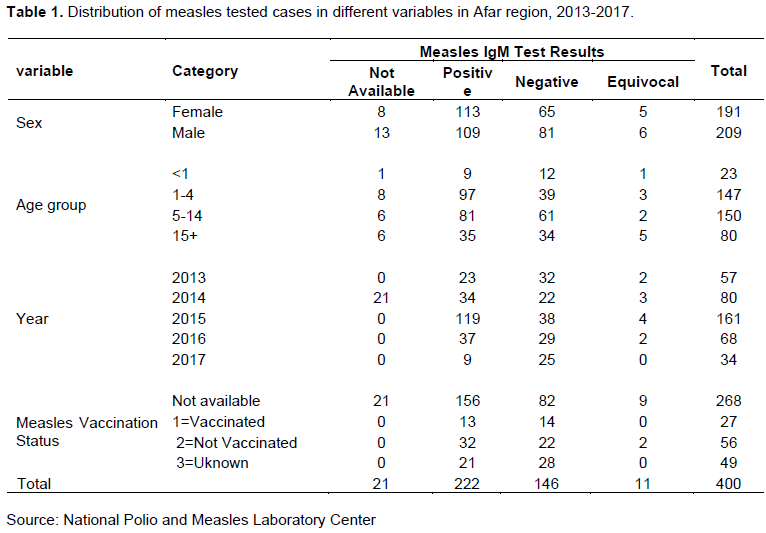
In the period between 2013 and 2017, a total of 400 cases of measles were documented throughout the region, according to case-based laboratory data for surveillance. Male and female measles cases were nearly equally distributed; 52.2% (209) of them were men, and 47.8% (191) were women. The median age of the cases was 6 years old, with ages ranging from 1 month to 60 years old.
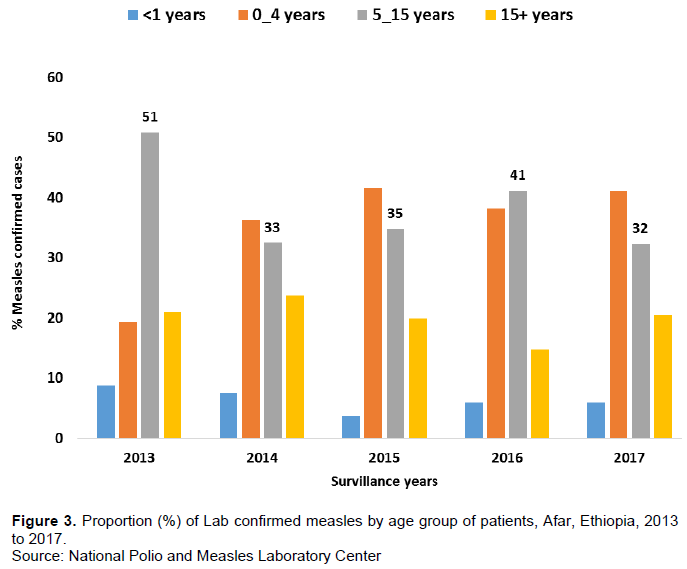
Among the total cases, 222 (55.5%) were laboratory-confirmed measles cases, 146 (36.5%) were negative for measles IgM, 11 (2.75%) were equivocal cases, and the remaining 22 (5.5%) had no lab results. It is difficult to find the result for rubella virus-specific IgM antibody, another rash febrile illness, among the total 157 measles IgM negatives and equivocal cases. Children 5-14 years old had the highest proportion of tested people (37.5%), followed by children 0-4 years old (36.8%). Measles confirmed cases increased up to the age of 15 years and then decreased after that (Figure 3).
Of the total number of measles case-based laboratory data, 317 (79.25%) lacked information on their immunization status, 27 (6.75%) were immunized, and the remaining 56 (14%) were not immunized (Table 1). Sample collection peaked in 2015 with 161 and in 2017 with 34. (Table 1). The year with the fewest positives (9) was in 2017, and the highest positive proportion (73.9%) was 2015 (Table 1).
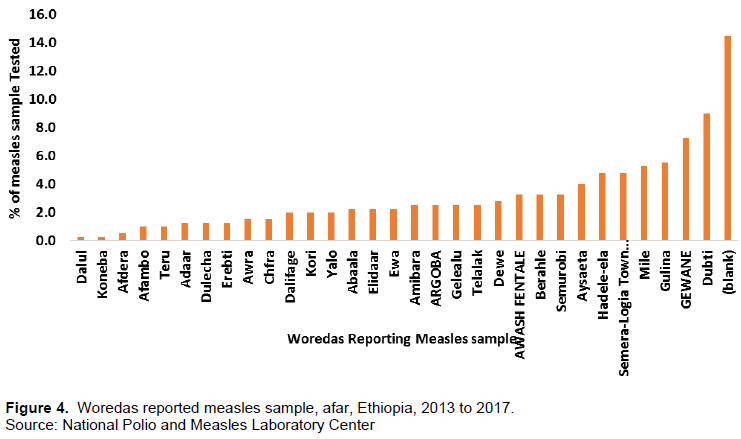
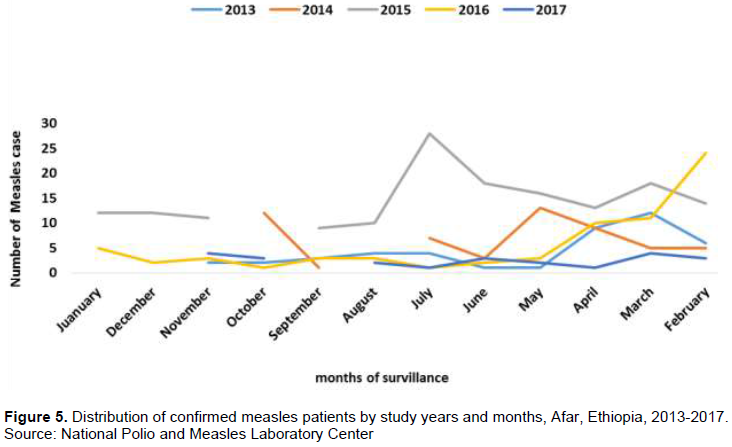
Out of all district case-based laboratory data, Dubti district has the highest 36 (9%), and Dalule and Koneba districts have the fewest sample numbers 1 (0.3%), each among 34 districts. In the last five years, 58 (14.5%) most districts were blank, as shown in Figure 4. The highest laboratory sample tested throughout 2015 was 161 (40.25%), and the highest sample tested in July was 28 (7%), as seen in Figure 5. As indicated in Table 1, the year 2017 had the smallest sample tested 34 (8.5%), among the samples recorded over the previous five years. In July, there was just one sample tested.
DISCUSSION
According to an analysis of measles case-based surveillance laboratory data in the Afar region of Ethiopia from 2013 to 2017, 400 suspected cases were investigated, with an average of 80 blood samples collected and tested annually. This was significantly lower than the average number of annually notified cases of 2405 Southern Nation Nationalities of Peoples Region, Amhara regional state (Getahun et al., 2016), despite the fact that the population is nine times that of Afar region (Getahun et al., 2017).
Measles positivity rates were high in 2015 and 2013 in the region, and this could be due to the occurrence of an outbreak in the study area during this period. Most suspected measles cases were reported in July. This is not justified by this work since it is the opposite of the measles seasonality report; most of the cases occurred in the dry season (Geremew et al., 2021).
Among the total measles suspected tested samples, 55.5% were confirmed measles, indicating the presence of the virus in the community or improved case capturing due to case-sensitive surveillance in the region. This positivity rate was significantly higher than that found in SNNPR (Getahun et al., 2017), Gambia (Sowe et al., 2021), and South West Nigeria (Fatiregun et al., 2015). The number and the proportion of lab-confirmed measles cases fluctuated, but the incidence of confirmed measles (laboratory plus epi-linked) cases increased consistently from 2013 to 2015 (57, 80 and 161), respectively. The incidence of measles cases decreased as the age group increased (above 15 years), as measles infection results in life-long immunity.
According to the five-year measles laboratory case-based data of the afar region, only 6.75% of cases have a history of measles vaccination, which requires a review and emphasis on the region's expanded program of immunization. According to the WHO-Afro Measles and Rubella Surveillance Guidelines, measles suspected cases which were tested and found to be negative or equivocal will be tested for rubella virus-specific IgM, a rash febrile illness. This vaccination status is better as compared with the study conducted in Italy in 2011 (Filia et al., 2015).
Most of the laboratory-confirmed measles cases were under the age of 15 in the afar region from 2013 to 2017. This may be due to the reason that the routine immunization programs were weak, and unimmunized children of school age had risks of acquiring measles disease.
In this study, 44.5% of non-measles cases did not know their rubella virus status; however, the Southern Nation Nationalities of People’s Region study found that 17.3% of measles IgM negative samples were positive for rubella (Getahun et al., 2017).
The data analysis had the following limitations: first, the data was only related to laboratory-confirmed measles data, with little emphasis on clinically confirmed and epidemiologically linked cases detailed as laboratory data. Second, there is no information on the clinical signs and symptoms of the cases, such as fever, maculopapular rash, diarrhea, and vomiting, as well as complications such as ear and sinus infection, persistent diarrhea, and pneumonia. Third, there are no measles indicator variables by administrative, such as expected and reported non-measles febrile rash rate cases by zone and district, which are required for determining the incidence and annualized non-measles febrile rash rate. Finally, there is no information in the laboratory data on rubella IgM results for cases other than measles.
CONCLUSION
Measles is still a major health problem in this region, primarily affecting children aged 5 to 14. The number of laboratory-confirmed measles cases varies by year and season. Most children have unknown vaccination status, and the sample tested in different years is different, possibly due to health system improvement or a lack of sensitivity in the surveillance system in health facilities and district health offices. The names of health facilities and districts were inconsistent, and districts were not filled, as were measles indicators such as NMFRR, incident rate, the district expected and reported measles, total population, specimen condition, and week of report, all of which are critical indicators in the database system.
RECOMMENDATIONS
(1) To increase the region's measles vaccination rate, FMOH should execute supplemental immunization activity (SIA) in partnership with EPHI and other partners.
(2) The surveillance efforts need to be improved for the specificity of reporting suspected measles in all hierarchies, the completeness of variables, and the early detection of cases.
(3) Yearly review meeting that is held regularly to discuss vaccine-preventable disease
(4) Enhanced database administration for simpler analysis.
ACKNOWLEDGEMENT
The authors appreciate the contribution of the Ethiopian Public Health Institute vaccine preventable team for technical support of the National Measles Surveillance Program and all health care workers involved in case identification and sample collection, and patients who gave blood at all health institutions in Afar Region, Ethiopia.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Asmare K, Asmare M, Adugna C, Tezera N, Mulualem G, Tarik T (2022). Spatiotemporal distributions of immunization coverage in Ethiopia from 2000 to 2019. Vaccine 40(10):1413-1420. |
|
|
Ethiopian Health and Nutrition Research Institute, Federal Democratic Republic of Ethiopia (2012). Ethiopia: guideline on measles surveillance and outbreak management. |
|
|
Fatiregun AA, Adebowale AS, Fagbamigbe AF (2015). Epidemiology of measles in Southwest Nigeria?: an analysis of measles case-based surveillance data from 2007 to 2012. Transactions of the Royal Society of Tropical Medicine and Hygiene 108(3):133-140. |
|
|
Filia A, Bella A, Rota MC, Tavilla A, Magurano F, Baggieri M (2015). Analysis of national measles surveillance data in Italy from October 2010 to December 2011 and priorities for reaching the 2015 measles elimination goal. Eurosurveillance 18(20):20480. |
|
|
Getahun M, Beyene B, Ademe A, Teshome B, Tefera M, Afework A (2017). Epidemiology of laboratory confirmed measles virus cases in the southern nations of Ethiopia, 2007-2014. BMC infectious diseases 17(1):1-8. |
|
|
Getahun M, Beyene B, Ademe A, Teshome B, Tefera M, Asha A (2016). Epidemiology of laboratory confirmed measles virus cases in Amhara Regional State of Ethiopia, 2004 - 2014. BMC infectious diseases 16(1):1-7. |
|
|
Global Immunization Division Center for Global Health (2022). Ethiopia Moves Forward with Mass Measles Vaccination Campaign during COVID-19 Pandemic Protecting 14.5 Million Children. |
|
|
Goitom G. Weldegebriel, Alex Gasasira, Pauline Harvey, Balcha Masresha, James L. Goodson, Muhammad A. Pate, Emmanuel Abanida, and Ana Chevez (2008). Measles Resurgence Following a Nationwide Measles Vaccination Campaign in Nigeria, 2005-2008. Journal of Infectious Diseases Pages S226-S231. |
|
|
Goodson JL, Masresha BG, Wannemuehler K, Uzicanin A, Cochi S (2011). Changing Epidemiology of Measles in Africa 204(Suppl 1):205-214. |
|
|
Masresha BG, Fall A, Eshetu M, Sosler S, Alleman M, Goodson JL (2009). Measles Mortality Reduction and Pre- Elimination in the African Region 2001-2011. 204(Suppl 1). |
|
|
Minal K. Patel, MD; Marta Gacic- Dobo (2016). Progress Toward Regional Measles Elimination - Worldwide, 2000-2015. Morbidity and mortalyity report 65(44). |
|
|
Mitiku K, Bedada T, Masresha BG, Kegne W, Nafo-Traoré F, Tesfaye N, Yigzaw A (2011). Progress in measles mortality reduction in Ethiopia, 2002-2009. The Journal of infectious diseases 204(suppl_1):S232-S238. |
|
|
Munira NH , Abyot BW, Mekonen G, Berhane B, Lucy B, Ayesheshem A, Alemayehu B (2018). Epidemiology of measles in the metropolitan setting, Addis Ababa, Ethiopia, 2005-2014: a retrospective descriptive surveillance data analysis. BMC Infectious Diseases 18(1). |
|
|
Okonko IO, Nkang AO, Udeze AO, Adedeji AO, Ejembi J, Onoja BA (2009). Global eradication of measles: A highly contagious and vaccine preventable disease-what went wrong in Africa? 3(8):119-140. |
|
|
Sowe A, Njie M, Sowe D, Fofana S, Ceesay L, Camara Y, Tesfaye B, Bah S, Bah AK, Baldeh AK, Dampha BD (2021). Epidemiology of measles cases, vaccine effectiveness, and performance towards measles elimination in The Gambia. PLoS One 16(10):e0258961. |
|
|
Wolters K (2017). Elimination of measles from India: Challenges ahead and the way forward. Journal of postgraduate medicine 63(2):75-78. |
|
|
World Health Assembly (2012). Draft global vaccine action plan. 65th World Health Assembly pp. 21-26. |
|
|
World Health Assembly (2015). Weekly epidemiological record Relevé épidémiologique hebdomadaire. 50(04):29-31. |
|
|
WHO (2015). Office WHOR. African Regional Guidelines for Measles and Rubella Surveillance WHO Regional Office for Africa pp. 1-82. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


