Full Length Research Paper

ABSTRACT
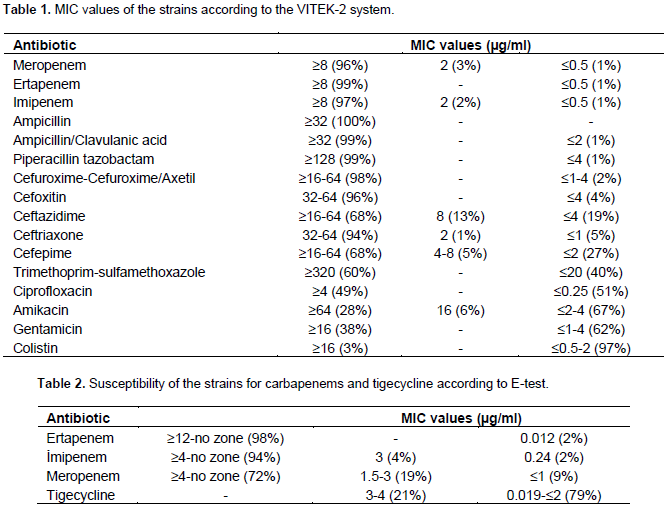
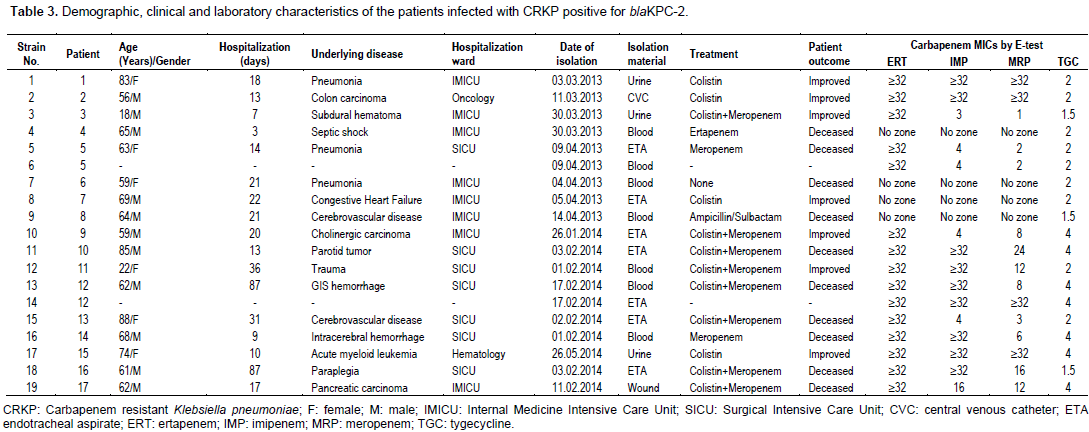
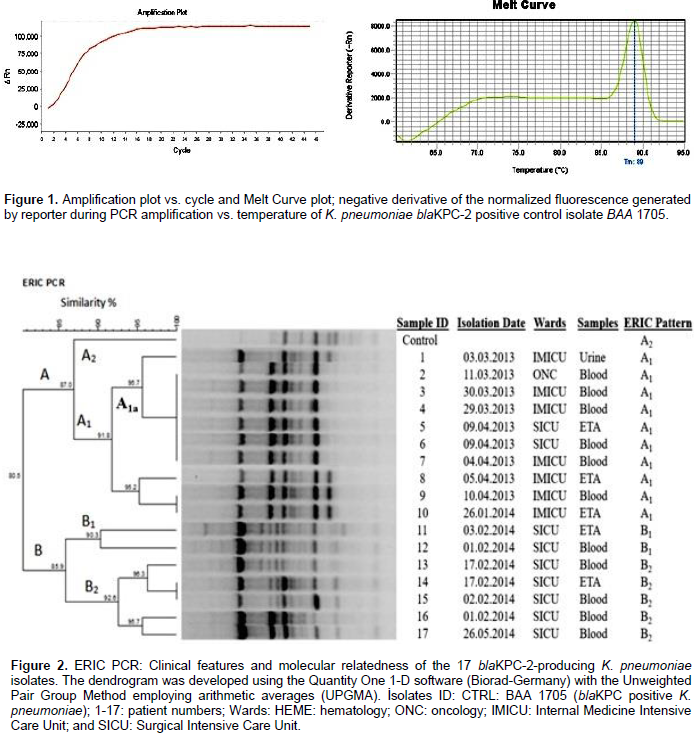
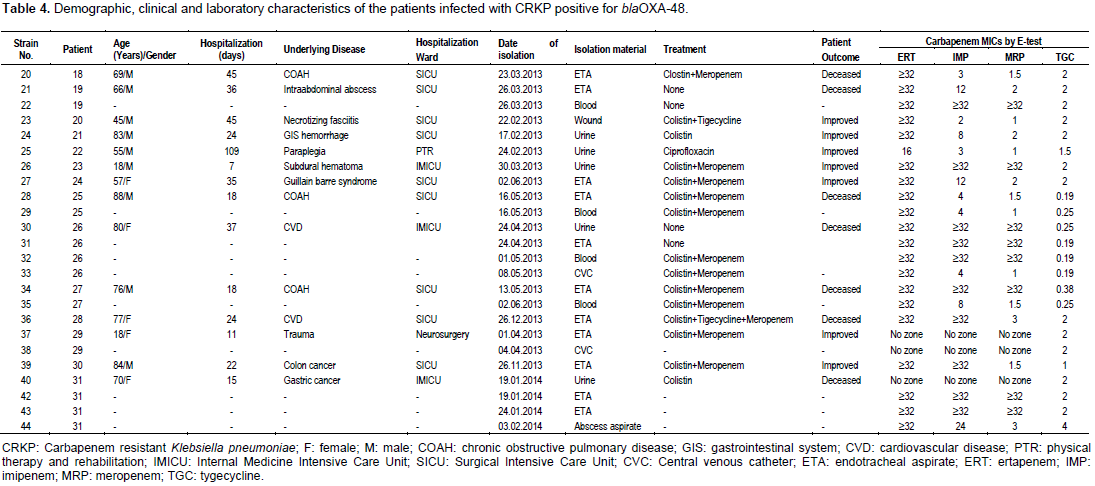
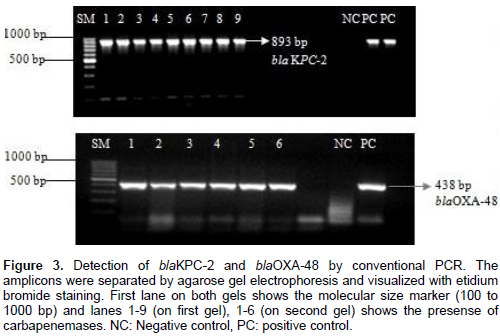
Carbapenem-resistant Klebsiella pneumoniae carrying blaKPC-2, blaOxa48, and other metallo-ï¢-lactamases (MBLs) are difficult to treat. This study was conducted to study the phenotypic and genotypic features of carbapenem resistance in isolates of K. pneumoniae isolated from a tertiary care hospital in the European region of Turkey. Isolates of K. pneumonia (n=100) resistant to at least one carbapenem (imipenem, meropenem, or ertapenem) were collected from 60 patients for 14 months. Carbapenem resistance was determined via the VITEK-2 system and the E-test confirmed this. The Modified Hodge Test (MHT) and Double Disc Synergy Test (DDST) were performed. Genes were analyzed by Sybr-Green real-time, multiplex and convensional polymerase chain reaction (PCR). Phylogenetic relatedness was analyzed by ERIC-PCR. The rate of resistance by E-test against ertapenem, imipenem, and meropenem were 98, 94, and 72%, respectively; 21% of isolates were somewhat susceptible to tygecycline. The MHT positivity was 98% and DDST was negative in all cases. There were 19 and 24% of isolates positive for blaKPC-2 and blaOxa-48, respectively. ERIC-PCR showed that all blaKPC-2-positive isolates were branched into two main clusters with 80.5% similarity. The results indicate that blaKPC-2 mediated carbapenem-resistant Klebsiella pneumoniae (CRKP) infection is spreading in Turkey and blaOXA-48 endemicity continues to be a serious problem. The molecular determination of carbapenemases will be useful for patients with concurrent carbapenem-resistant Enterobacteria¬ceae (CRE) infections. This could prevented outbreaks and complications.
Key words: Klebsiella pneumoniae, carbapenem resistance, blaKPC-2, blaOxa-48.
INTRODUCTION
MATERIALS AND METHODS
RESULTS

DISCUSSION
CONCLUSION
SUPPLEMENTARY DATA
CONFLICT OF INTERESTS
ACKNOWLEDGEMENTS
REFERENCES
|
Aktas Z, Kayacan CB, Schneider I, Can B, Midilli K, Bauernfeind A (2008). Carbapenem-hydrolyzing oxacillinase, OXA-48, persists in Klebsiella pneumoniae in Istanbul, Turkey. Chemotherapy 54(2):101-106. |
|
|
Al-Zahrani IA, Bander AA (2018). The emergence of carbapenem-resistant Klebsiella pneumoniae isolates producing OXA-48 and NDM in the Southern (Asir) province, Saudi Arabia. Saudi Med. J. 39(1):23-30. |
|
|
Andrade LN, Vitali L, Gaspar GG, Bellissimo-Rodrigues F, Martinez R, Darini AL (2014). Expansion and evolution of a virulent, extensively drug-resistant (polymyxin B-resistant), QnrS1-, CTX-M-2-, and KPC-2-producing Klebsiella pneumoniae ST11 international high-risk clone. J. Clin. Microbiol. 52(7):2530-2535. |
|
|
Azap O, Otlu B, Yesilkaya A, Yakupogullari Y (2013). Detection of OXA-48-like Carbapenemase-Producing Klebsiella pneumoniae in a Tertiary Care Center in Turkey: Molecular Characterization and Epidemiology. Balkan Med. J. 30(2):259-260. |
|
|
Band VI, Satola SW, Burd EM, Farley MM, Jacob JT, Weissb DS (2018). Carbapenem-resistant Klebsiella pneumoniae exhibiting clinically undetected colistin heteroresistance leads to treatment failure in a murine model of infection. M. Bio. 9(2):e02448-17. |
|
|
Baran I, Aksu N (2016). Phenotypic and genotypic characteristics of carbapenem-resistant Enterobacteriaceae in a tertiary-level reference hospital in Turkey. Ann. Clin. Microbiol. Antimicrob. 6:15-20. |
|
|
Barguigua A, Zerouali K, Katfy K, El Otmani F, Timinouni M, Elmdaghri N (2015). Occurrence of OXA-48 and NDM-1 carbapenemase-producing Klebsiella pneumoniae in a Moroccan university hospital in Casablanca, Morocco. Infect. Genet. Evol. 31:142-148. |
|
|
Bassetti M, Nicolini L, Esposito S, Righi E, Viscoli C (2009). Current status of newer carbapenems. Curr. Med. Chem. 16(5):564-575. |
|
|
Bathoorn E, Tsioutis C, da Silva Voorham JM, Scoulica EV, Ioannidou E, Zhou K, Rossen JW, Gikas A, Friedrich AW, Grundmann H (2016). Emergence of pan-resistance in KPC-2 carbapenemase-producing Klebsiella pneumoniae in Crete, Greece: a close call. J. Antimicrob. Chemother. 71(5):1207-1212. |
|
|
Benouda A, Touzani O, Khairallah MT, Araj GF, Matar GM (2010). First detection of oxacillinase-mediated resistance to carbapenems in Klebsiella pneumoniae from Morocco. Ann. Trop. Med. Parasitol. 104(4):327-330. |
|
|
Ulu AC, Kurtaran B, Inal AS, Kömür S, Kibar F, Çiçekdemir HY, Bozkurt S, Gürel D, Kılıç F, Yaman A, Aksu HS (2015). Risk factors of carbapenem-resistant Klebsiella pneumoniae infection: a serious threat in ICUs. Medical Science Monitor: Int. Med. J. Exp. Clin. Res. 17(21):219-224. |
|
|
Carrer A, Poirel L, Eraksoy H, Cagatay AA, Badur S, Nordmann P (2008). Spread of OXA-48-positive carbapenem-resistant Klebsiella pneumoniae isolates in Istanbul, Turkey. Antimicrob. Agents Chemother. 52(8):2950-2954. |
|
|
Carrer A, Poirel L, Yilmaz M, Akan OA, Feriha C, Cuzon G, Matar G, Honderlick P, Nordmann P (2010). Spread of OXA-48-encoding plasmid in Turkey and beyond. Antimicrob. Agents Chemother. 54(3):1369-1373. |
|
|
Centers for Disease Control and Prevention (CDC) (2017). Healthcare-associated Infections: Tracking CRE. Available at http://www.cdc.gov/hai/organisms/cre/TrackingCRE.html. Accessed 11 April 2018. |
|
|
Chiu SK, Chan MC, Huang LY, Lin YT, Lin JC, Lu PL, Siu LK, Chang FY, Yeh KM (2017). Tigecycline resistance among carbapenem-resistant Klebsiella pneumoniae: Clinical characteristics and expression levels of efflux pump genes. PLoS One. 12(4):e0175140. |
|
|
Cizmeci Z, Aktas E, Otlu B, Acikgoz O, Ordekci S (2017). Molecular characterization of carbapenem- resistant Enterobacteriaceae yields increasing rates of NDM-1 carbapenemases and colistin resistance in an OXA-48- endemic area. J. Chemother. 29(6):344-350. |
|
|
Cuzon G, Naas T, Bogaerts P, Glupczynski Y, Huang TD, Nordmann P (2008). Plasmid-encoded carbapenem-hydrolyzing beta-lactamase OXA-48 in an imipenem-susceptible Klebsiella pneumoniae isolate from Belgium. Antimicrob. Agents Chemother. 52(9):3463-3464. |
|
|
Daikos GL, Markogiannakis A (2011). Carbapenemase-producing Klebsiella pneumoniae: (when) might we still consider treating with carbapenems? Clin. Microbiol. Infect. 17(8):1135-1141. |
|
|
Dortet L, Cuzon G, Ponties V, Nordmann P (2017). Trends in carbapenemase-producing Enterobacteriaceae, France, 2012 to 2014. Euro Surveill. 22(6):1-9. |
|
|
Fattouh R, Tijet N, McGeer A, Poutanen SM, Melano RG, Patela SN (2016). What Is the Appropriate Meropenem MIC for Screening of Carbapenemase-Producing Enterobacteriaceae in Low-Prevalence Settings? Antimicrob. Agents Chemother. 60(3):1556-1560. |
|
|
Fursova NK, Astashkin EI, Knyazeva AI, Kartsev NN, Leonova ES, Ershova ON, Alexandrova IA, Kurdyumova NV, Sazikina YS, Volozhantsev NV, Svetoch EA, Dyatlov IA (2015). The spread The spread of blaOXA-48 and blaOXA-244 carbapenemase genes among Klebsiella pneumoniae, Proteus mirabilis and Enterobacter spp. isolated in Moscow, Russia. Ann. Clin. Microbiol. Antimicrob. 14(46):1-9. |
|
|
Goren MG, Chmelnitsky I, Carmeli Y, Navon-Venezia S (2011). Plasmid-encoded OXA-48 in Escherichia coli from Israel. J. Antimicrob. Chemother. 66(3):672-673. |
|
|
Gulmez D, Woodford N, Palepou MF, Mushtaq S, Metan G, Yakupogullari Y, Kocagoz S, Uzun O, Hascelik G, Livermore DM (2008). Carbapenem-resistant Escherichia coli and Klebsiella pneumoniae isolates from Turkey with OXA-48-like carbapenemases and outer membrane protein loss. Int. J. Antimicrob. Agents 31(6):523-526. |
|
|
Hammoudi D, Ayoub Moubareck C, Aires J, Adaime A, Barakat A, Fayad N, Hakime N, Houmani M, Itani T, Najjar Z, Suleiman M, Sarraf R, Karam Sarkis D (2014). Countrywide spread of OXA-48 carbapenemase in Lebanon: surveillance and genetic characterization of carbapenem-non-susceptible Enterobacteriaceae in 10 hospitals over a one-year period. Int. J. Infect. Dis. 29:139-144. |
|
|
Jin-Long Y, MSW, An-Chun C, Kang-Cheng P, Chuan-Feng L, Shu-Xuan D, (2008). A simple and rapid method for extracting bacterial DNA from intestinal microflora for ERIC-PCR detection. World J. Gastroenterol. 14(18):2872. |
|
|
Karabay O, Altindis M, Koroglu M, Karatuna O, Aydemir A, Erdem AF (2016). The carbapenem-resistant Enterobacteriaceae threat is growing: NDM-1 epidemic at a training hospital in Turkey. Ann. Clin. Microbiol. Antimicrob. 15:1-6. |
|
|
Kuskucu MA, Karakullukcu A, Ailiken M, Otlu B, Mete B, Aygun G (2016). Investigation of carbapenem resistance and the first identification of Klebsiella pneumoniae carbapenemase (KPC) enzyme among Escherichia coli isolates in Turkey: A prospective study. Travel Med. Infect. Dis. 14(6):572-576. |
|
|
Labarca J, Poirel L, Ozdamar M, Turkoglu S, Hakko E and Nordmann P (2014). KPC-producing Klebsiella pneumoniae, finally targeting Turkey. New Microbes and New Infections. 2(2):50-51. |
|
|
Li J, Zou MX, Wang HC, Dou QY, Hu YM, Yan Q, Liu WE (2016). An Outbreak of Infections Caused by a Klebsiella pneumoniae ST11 Clone Coproducing Klebsiella pneumoniae Carbapenemase-2 and RmtB in a Chinese Teaching Hospital. Chin. Med. J. (Engl). 129(17):2033-2039. |
|
|
Meletis G (2016). Carbapenem resistance: overview of the problem and future perspectives. Ther. Adv. Infect. Dis. 3(1):15-21. |
|
|
Munoz-Price LS, Poirel L, Bonomo RA, Schwaber MJ, Daikos GL, Cormican M, Cornaglia G, Garau J, Gniadkowski M, Hayden MK, Kumarasamy K, Livermore DM, Maya JJ, Nordmann P, Patel JB, Paterson DL, Villegas MV, Wang H, Woodford N, Quinn JP (2013). Clinical epidemiology of the global expansion of Klebsiella pneumoniae carbapenemases. The Lancet Infect. Dis. 13(9):785-796. |
|
|
Nazik H, Aydin S, Albayrak R, Bilgi EA, Yildiz I, Kuvat N, Kelesoglu FM, Pakasticali N, Yilmaz F and Öngen B (2014). Detection and Spread of Oxa-48-Producing Klebsiella oxytoca Isolates in Istanbul,Turkey. Southeast Asian J. Trop. Med. Public Health. 45(1):123-129. |
|
|
Pasteran F, Faccone D, Rapoport M, Veliz O, Guerriero L, Gomez S, Petroni A, Corso A (2012). Rapid dissemination of OXA-163 carbapenemase, an emerging OXA-48 variant, in species of Enterobacteriaceae in multiple hospitals from Argentina: multiples clones and detection issues. Abstr 22th Eur Congress Clin Microbiol Infect, London, United Kingdom. |
|
|
Patel G, Bonomo R 2013 "Stormy waters ahead": global emergence of carbapenemases. Frontiers in microbiology. 4:48. |
|
|
Patel G, Huprikar S, Factor SH, Jenkins SG, Calfee DP (2008). Outcomes of carbapenem-resistant Klebsiella pneumoniae infection and the impact of antimicrobial and adjunctive therapies. Infect. Control Hosp. Epidemiol. 29(12): 1099-1106. |
|
|
Poirel L. Heritier C, Tolun V, Nordmann P (2004). Emergence of oxacillinase-mediated resistance to imipenem in Klebsiella pneumoniae. Antimicrob. Agents Chemother. 48(1):15-22. |
|
|
Ramana KV, Rao R, Sharada ChV, Kareem M, Reddy LR, Ratna Mani M (2013). Modified Hodge test: A useful and the low-cost phenotypic method for detection of carbapenemase producers in Enterobacteriaceae members. J. Nat. Sci. Biol. Med. 4(2):346-348. |
|
|
Sahin K, Tekin A, Ozdas S, Akin D, Yapislar H, Dilek AR, Sonmez E (2015). Evaluation of carbapenem resistance using phenotypic and genotypic techniques in Enterobacteriaceae isolates. Ann. Clin. Microbiol. Antimicrob. 14:44-49. |
|
|
Saidani M, Hammami S, Kammoun A, Slim A, Boutiba-Ben Boubaker I (2012). Emergence of carbapenem-resistant OXA-48 carbapenemase-producing Enterobacteriaceae in Tunisia. J. Med. Microbiol. 61(12):1746-1749. |
|
|
Sheng JF, Li JJ, Tu S, Sheng ZK, Bi S, Zhu MH, Shen XM, Li LJ (2012). blaKPC and rmtB on a single plasmid in Enterobacter amnigenus and Klebsiella pneumoniae isolates from the same patient. Eur. J. Clin. Microbiol. Infect. Dis. 31(7):1585-1591. |
|
|
Skalova A, Chudejova K, Rotova V, Medvecky M, Studentova V, Chudackova E, Lavicka P, Tamara Bergerova T, Jakubu V, Zemlickova H, Papagiannitsis CC, Hrabak J (2017). Molecular Characterization of OXA-48- Like-Producing Enterobacteriaceae in the Czech Republic and Evidence for Horizontal Transfer of pOXA-48-Like Plasmids. Antimicrob. Agents Chemother. 61(2):e01889-16. |
|
|
Srinivasan R, Ellappan K, Narasimha HB (2015). Prevalence and characterization of NDM-1 and OXA-48 carbapenemase gene harboring Enterobacteriaceae in a tertiary care hospital, South India. Acad. J. 7(6):60-63. |
|
|
Thomas CP, Moore LS, Elamin N, Doumith M, Zhang J, Maharjan S, Warner M, Perry C, Turton JF, Johnstone C, Jepson A, Duncan ND, Holmes AH, Livermore DM, Woodford N (2013). Early (2008-2010) hospital outbreak of Klebsiella pneumoniae producing OXA-48 carbapenemase in the UK. Int. J. Antimicrob. Agents. 42(6):531-536. |
|
|
Tzouvelekis LS, Markogiannakis A, Psichogiou M, Tassios PT, Daikos GL (2012). Carbapenemases in Klebsiella pneumoniae and other Enterobacteriaceae: an evolving crisis of global dimensions. Clin. Microbiol. Rev. 25(4):682-707. |
|
|
US Food and Drug Administration (FDA). FDA Approved Drug Products. |
|
|
van Duin D, Cober E, Richter SS, Perez F, Kalayjian RC, Salata RA, Evans S, Fowler VG, Bonomo RA, Kaye KS (2015). Residence in Skilled Nursing Facilities Is Associated with Tigecycline Nonsusceptibility in Carbapenem-Resistant Klebsiella pneumoniae. Infect. Control Hosp. Epidemiol. 36(8):942-948. |
|
|
van Duin D, Doi Y (2017). The global epidemiology of carbapenemase-producing Enterobacteriaceae. Virulence 8(4):460-469. |
|
|
Wayne PA (2014). Clinical and Laboratory Standards Institute, Performance standards for antimicrobial susceptibility testing; twentyfourth informational supplement. CLSI document M100-24. |
|
|
Yigit H, Queenan AM, Anderson GJ, Domenech-Sanchez A, Biddle JW, Steward CD, Alberti S, Bush K, Tenover F (2001). Novel carbapenem-hydrolyzing beta-lactamase, KPC-1, from a carbapenem-resistant strain of Klebsiella pneumoniae. Antimicrob. Agents Chemother. 45(4):1151-1161. |
|
|
Yu F, Wang S, Lv J, Qi X, Guo Y, Tang YV, Kreiswirth BN, Wang L, Chen L (2017). Coexistence of Oxa-48-Producing Klebsiella pneumoniae and Escherichia coli in a Hospitalized Patient Who Returned from Europe to China. Antimicrob. Agents Chemother. 61(4):e02580-16. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


