ABSTRACT
Surgical site infections (SSI) caused by rapidly growing mycobacterial (RGM) have become increasingly frequent. The aim of this study is to describe the epidemiological, clinical aspects and factors associated with RGM infections related to plastic surgery. Notifications of SSI from 86 health care facilities of the capital of a Brazilian state within nine years, approximately, were assessed. RGM, predominantly M. fortuitum (39.0%), was isolated from 66 cases of infection folowing plastic surgery, mainly mammoplasty. All the cases were woman, with an average of 32.9 years. Amikacin/clarithomycin was the prevalent therapeutic regimen, and most of the isolates showed resistance to ciprofloxacin. There was an association of infection by M. abscessus and use of surgical instruments that were not exclusive to the institution (P=0.048). Thus, these findings emphasize the importance of SSI notifications and strict monitoring of surgical instruments reprocessing.
Key words: Surgical site infection, plastic surgery, non-tuberculous mycobacteria.
Surgical site infections (SSI) caused by non-tuberculous rapidly growing mycobacteria (NTRGM) have been reported, including after plastic surgery, mainly liposuction and mammoplasty (Sharma et al., 2016; Romero et al., 2017). Outbreaks have occurred in geographically distant locations (Leão et al., 2010) in Brazil since 2000. The greatest occurred in the Southeastern region (172 cases), where 38 hospitals had cases confirmed by culture, with Mycobacterium massiliense isolates belonging to a single clone (BRA100), which showed
consistent tolerance to the 2% glutaraldehyde solution (Duarte et al., 2009).
Thus, health authorities concluded failures in the reprocessing of surgical instruments closely related to the inappropriate use of chemical sanitizers and, therefore, suspended sterilization in liquid media across the country in 2009 (Agência Nacional de Vigilância Sanitária, 2009). However, cases of post-surgical mycobacteriosis continued to be reported across the country. In the Goiás State, 44 cases were reported between 2014 to 2018 (Agência Nacional de Vigilância Sanitária, 2019). Given the complexity of SSIs, especially by mycobacteria, this study aimed to describe the epidemiology, clinical aspects and factors associated with NTRGM infections related to plastic surgery.
After ethical approval (Protocol n. 1269485/2015), a retrospective study was performed on infection notifications of the official data base of the Public Health System (composed of 86 public and private hospitals) of a city in the Brazilian Midwest region. The data ranged from the first case and infection related to plastic surgery notified in 2007 (when the notification was due to spontaneous demand) until December 2015 (notifications became mandatory in 2008). Notifications of post-surgical mycobacterioses have become mandatory in Brazil since 2008. Before that, the municipal services used to investigate notifications of cases by spontaneous demand. National compulsory notifications are made through a computerized system called FormSUS, a form that interconnects the municipal, state and federal health departments. A case was considered: any patient who presented SSI, after a plastic surgery, notified with a positive culture result for NTRGM (from surgical wound or adjacent tissues). The resistance profile of the isolates was determined by minimum inhibitory concentration (MIC) (Clinical and Laboratory Standards Institute, 2011).
Data were collected by the reseachers following a check list, and analyzed using SPSS software version 24.0. NTRGM infections were considered as the outcome variable and as predictors: year of notification, type of institution, underlying disease, age, type of surgery, number of surgeries, surgical method, use of loaner surgical instruments/devices, reprocessing of surgical instruments in the healthcare facility, and surgical instruments exclusive of the healthcare facility. Poisson's bivariate analysis was performed, and statistical significance was established by Wald's chi-square test. To compare proportions, Fisher's exact test was used. Values of P<0.05 were considered statistically significant.
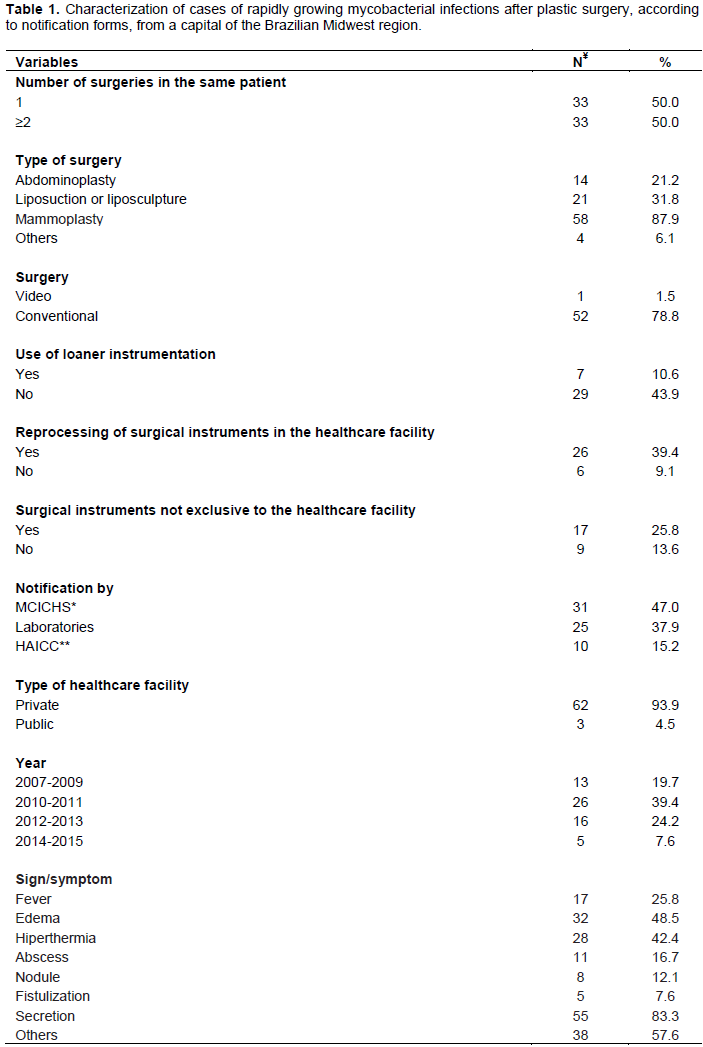
A total of 66 positive culture (95.7%; 95% CI: 88.0-98.5%) out of 69 notifications were identified, all in women.
The average of age was 32.9 years (SD: 8.6; median: 32; Minimum: 21; Maximum: 61). Half of them underwent more than one plastic procedure at the same day, and the majority (87.9%) underwent mammoplasty. Twenty hospitals were involved, with a predominance of private establishments (18/93.9%) (Table 1). Of these, two occurred in the same clinic. Regarding the clinical profile, the most common sign was the presence of secretion in the surgical wound (83.3%), followed by edema (48.5%) and hyperemia (42.2%) (Table 1). Surgical treatment with removal of prostheses was necessary in 37.8% of cases (Table 1). Two cases of physical sequelae were identified, resulting from infections with permanent scarring (breast and gluteus).
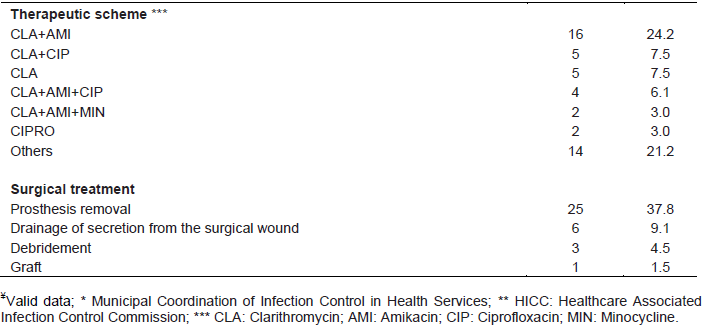
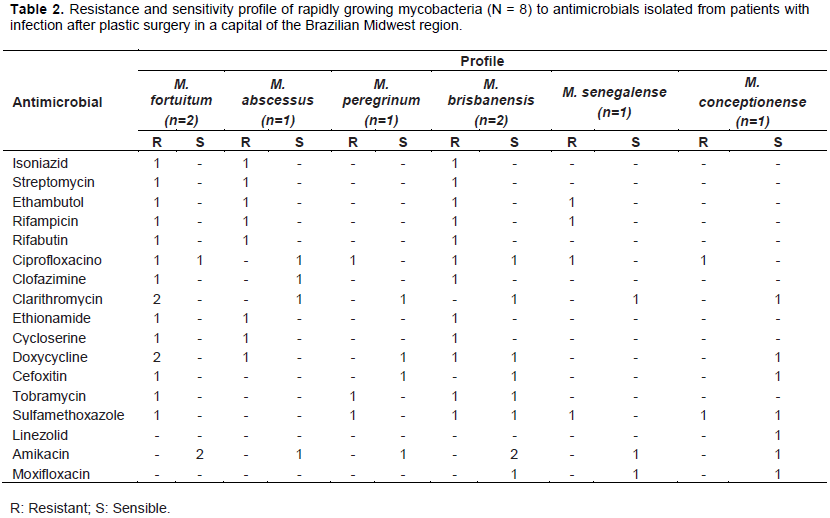
Of the 66 isolates, M. fortuitum (39%) predominated, followed by M. abscessus (18.0%), M. peregrinum (12.0%), M. brisbanensis (9.0%), and other species (M. mageritense, M. senegalense, M. wolinsky, M. conceptionense and M. chelonae). Five species were resistant to ciprofloxacin, but M. abscessus was sensible to this antimicrobial. M. fortuitum was the specie that showed resistance to the largest number of antimicrobials concomitantly, followed by M. brisbanensis and M. abscessus (Table 2). M. abscessus infection was associated with the use of surgical instruments non-exclusive to the healthcare facility (P=0.048).
M. fortuitum and M. abscessus are species frequently reported as etiologic agents in infections arising from plastic surgeries (Sharma et al., 2016; Romero et al., 2017). Resistance to ciprofloxacin was evidenced in NTRGM analyzed in different regions of Brazil (Duarte et al., 2009). SSIs caused by NTRGM are difficult to manage, since the diagnosis is late (Park et al., 2016) and the antimicrobial treatment is prolonged; it brings side effects to the patient, which also hinders the healing process of the infection (Sharma et al., 2016; Romero et al., 2017). In many cases, there is a need for surgical intervention. Studies have shown that the removal of breast implants after infections by M. abscessus and M. fortuitum resulted in a better prognosis for the patient (Sharma et al., 2016; Romero et al., 2017). On the other hand, surgical interventions for debridement and removal of prostheses due to infection have culminated in physical sequelae (Park et al., 2016).
It is known that exogenous factors to the patient, such as inadequate reprocessing of surgical instruments, increase the risk of SSI, and that the acquisition of loaner surgical instruments, as well as the use of products owned by the surgeon, are factors that interfere negatively in the quality of its reprocessing (Seavey, 2010). Although the healthcare facility has the responsibility to ensure the safety of the reusable medical devices (RMD), there are problems related to the management and reprocessing of these devices that can put patients and healthcare team at risk.
The cleaning step, considered the most important in the reprocessing of RMD, is generally the most affected in the case of loaner instruments/devices, especially due to delays in the delivery of the surgical set to the establishment with the necessary advance for the fulfillment of all reprocessing steps. This can lead workers to take “shortcuts” to meet the expected time for the surgical procedure. Additionally, the high-turnover of these sets in several healthcare services makes it impossible to guarantee the quality of the reprocessing steps in all of them (Seavey, 2010). An analysis of loaner instruments and orthopedic implants in clinical use revealed their contamination, including by biofilm, at the time of delivery to the hospital, as well as after the sterilization process, that is, ready-to-use (Costa et al., 2018).
In conclusion, SSIs by NTRGM following plastic surgery, predominantly by M. fortuitum, including species resistant to ciprofloxacin, occurred in young women, especially those that underwent the procedures in private clinics. These results highlight the importance of SSI notification through a robust surveillance system. The association of M. abscessus infection with the use of non-exclusive instruments points to the need for rigorous management and reprocessing of these devices, as well as the registration of these products both by the Sterilizing Service Unit and in the patients' records in order to allow its traceability.
The authors have not declared any conflict of interests.
REFERENCES
|
Agência Nacional de Vigilância Sanitária (2009). Ministério da Saúde - Resolução nº 8 de 27 de fevereiro de 2009. Dispõe sobre as medidas para redução da ocorrência de infecções por Micobactérias de Crescimento Rápido - MCR em serviços de saúde - Brazil, Brasília.
|
|
|
|
Agência Nacional de Vigilância Sanitária (2019). Ministério da Saúde - Boletim de Segurança do Paciente e Qualidade em Serviços de Saúde n°19, GVIMS/GGTES/Anvisa. Notificações de Casos de infecções por Micobactérias de Crescimento Rápido (MCR) de 2014-2018. Brazil, Brasília. Available:
View Accessed 10 October 2019.
|
|
|
|
|
Clinical and Laboratory Standards Institute (2011). Susceptibility Testing of Micobacteria, Nocardiae, and Other Aerobic Actinomycetes; Approves Standard- Second Edition. CLSI document M24-A2. Wayne.
|
|
|
|
|
Costa DM, Lopes LK, Tipple AF, Johani K, Deva AK, Watanabe E, Vickery K (2018). Evaluation of stainless steel surgical instruments subjected to multiple use/processing. Infection, Disease and Health 23:3-9.
Crossref
|
|
|
|
|
Duarte RS, Lourenço MC, Souza-Fonseca L, Leao SC, Efigenia de Lourdes TA, Rocha IL, Coelho FS, Viana-Niero C, Gomes KM, da Silva MG, Lorena NS, Pitombo MB, Ferreira RM, Garcia MH, de Oliveira GP, Lupi O, Vilaça BR, Serradas LR, Chebabo A, Marques EA, Teixeira LM, Dalcolmo M, Senna SG, Sampaio JL (2009). Epidemic of postsurgical infections caused by Mycobacterium massiliense. Journal of Clinical Microbiology 47(7):2149-55.
Crossref
|
|
|
|
|
Leão SC, Viana-Niero C, Matsumoto CK, Lima KVB, Lopes ML, Palaci M, Hadad DJ, Vinhas S, Duarte RS, Lourenço MCS, Kipnis A, Neves ZC, Gabardo BMA, Ribeiro MO, Baethgen L, Assis DB, Madalosso G, Chimara E, Dalcolmo MP (2010). Epidemic of surgical-site infections by a single clone of rapidly growing mycobacteria in Brazil. Future Microbiology 5(6):971-80.
Crossref
|
|
|
|
|
Park BY, Kwon JW, Kang SR, Hong SE (2016). Analysis of malpractice claims associated with surgical site infection in the field of plastic surgery. Journal of Korean Medical Science 31(12):1963-1968.
Crossref
|
|
|
|
|
Romero FA, Powell EA, Babady NE, Kaltsas A, Figueroa CJ, Pulitzer M, Mehrara BJ, Glickman MS, Morjaria S (2017). Nontuberculous Mycobacterial Infections After Silicone Breast Implant Reconstruction Emphasize a Diversity of Infecting Mycobacteria. Open Forum Infectious Diseases 4(4):ofx189.
Crossref
|
|
|
|
|
Seavey R (2010). Reducing the risks associated with loaner instrumentation and implants. AORN Journal 92(3):322-34.
Crossref
|
|
|
|
|
Sharma P, Vazquez-Guillamet LJ, Miljkovic G (2016). Atypical Mycobacterial infection after abdominoplasty overseas: a case report and literature review. Case Reports in Infectious Diseases 2016:3642567.
Crossref
|
|