ABSTRACT
The aim of the research is to assess the factors fuelling Antimicrobial Resistance (AMR) and its economic and clinical burden. For this purpose, a systematic review was conducted, which included an analysis of factors and economic and clinical burden of AMR. It was found that poorly treated sewage; discharges from antibiotic manufacturing plants, empirical prescribing, lack of antimicrobial stewardship, poor AMR monitoring; hospital-acquired infections and human-to-human contacts with environmental pathogens through food; and increase in global trade and travel are the factors behind the spread of AMR. Further, based on previous research, the study found a significant economic and clinical burden caused by AMR infections. It is recommended that well-organised antimicrobial stewardship be in place, AMR monitoring, limit access to antibiotics via over the counter dispensing without prescriptions, mandatory sensitivity tests for antimicrobial prescription be considered, proper hygiene in hospitals and medicine manufacturing sites must be ensured to reduce global AMR.
Key words: Antimicrobial Resistance, antimicrobial resistance (AMR), antibiotic resistance, economic burden, clinical burden.
Over the last decade, antimicrobial resistance (AMR) has become a global menace. Its rise is due to the misuse of antimicrobial in food-producing humans and animals, and globalisation and suboptimal infection control facilitated its spread across the globe (Huttner et al., 2013). According to WHO (2017), AMR is a comprehensive term for resistance in several types of microorganism and involves resistance to antiviral, antiphrastic, antiviral and antibacterial drugs. Consequently, the effectiveness of standard treatment is lost, and infections continue to spread. AMR is observed as a global concern because of the existing and probable effect on global population health, Gross Domestic Product (GDP) and cost to healthcare, largely through inadequate treatment options (O’Neill, 2014).
Earlier reports suggest that figures of infections are increasing globally due to resistant microbes (ECDC, 2015). Generally, the societal (or economic) viewpoint includes the possible effect on the labour via lost productivity (Smith and Coast, 2012); however, it also comprises the burden on patient out-of-pocket expenditures and on careers (Tam and O’Brien, 2016; Naylor et al., 2018). According to Hwang and Gums (2016), the rise of AMR has placed significant societal concerns and economic burden on the healthcare systems. Various factors have resulted in the occurrence of AMR, including access and inappropriate use of antimicrobials, microbial adaptation via selective pressures and a lack of new antimicrobials in development. Recently, efforts have been made to reduce a few of these factors in outpatient and inpatient setting along with increasing public awareness and promoting education to clinicians. The programs such as antimicrobial stewardship offer a multi-intervention framework to control the inappropriate recommending of antimicrobials, offer best antimicrobial therapy, and avert the increase of AMR.
AMR in humans is impacted by environmental and bacterial factors, such as exposure to environmental waste and pollution, hospital-acquired infections, over the use of antibiotics in animal farming and food production (Allcock et al., 2017). Landers et al. (2012) concluded that antimicrobial use in clinical medicine has substantially reduced the problem of infectious diseases and supported multifaceted medical interventions, for example, advanced surgery and organ transplantation which routinely are susceptible to infections have had positive outcomes. Further, in clinical medicine, the overuse or misuse of antimicrobial is a key factor behind the development of AMR in the global population. Maragakis et al. (2008) assert that treatment factors such as delay in proper antimicrobial treatment and toxicity related to treatment contributed to negative impacts in patients infected with AMR organisms.
Antimicrobials have a significant role in diminishing mortality and morbidity from infective diseases. Nevertheless, these benefits have been threatened by the rise and spread of bacteria that resist antimicrobials (O’Neil, 2014; Smith and Coast, 2012). KPMG (2014) and Taylor et al. (2014) asserted that AMR in recent years had become a prevalent issue in different countries, despite their income level. It was found that in 2014, approximately 700,000 deaths were reported globally, and all of them were linked to infections that resulted from AMR organisms. The ratio of death is expected to reach 10 million annually in a few decades if no robust mitigation measures are put in place.
According to Ventola (2015), AMR infections are a significant economic and clinical burden to the healthcare system in the United States and also to patients and their families. Such infections are prevalent in hospitals, because of the presence of vulnerable patients, increased use of antibiotics and extensive use of invasive procedures in healthcare settings. Approximately 2 million Americans annually develop Health Care-Associated Infections (HAIs), largely because of AMR pathogens. It was estimated that the overall economic burden due to AMR infections on the US economy was around $35 billion annually lost in productivity and $20 billion in healthcare costs. Also, AMR infections cause a huge burden to communities and families because of healthcare costs and lost wages. The reasons behind AMR are complex and comprise human behaviour in different aspects of society, and major environmental factors are behind the spread of AMR infections. Endeavours have been made in the past to describe dissimilar features of AMR and the interventions required to address the challenge (Laxminarayan et al., 2013).
Nevertheless, there has been a lack of coordinated action primarily at the political, national and global level. Indeed, antibiotics have shown positive effects in societal and medical developments and at present are essential in healthcare settings. The developments in modern medicine, for example, organ transplantation, surgery, preterm babies’ treatment and cancer chemotherapy would not be possible, which is taken for granted today without effective treatment for bacterial infections. It is most likely that in few years of time, that dire setback will have to be faced by humans economically, socially and medically, if unprecedented and real coordinated actions are not taken globally, we may revert to a pre-antibiotic era (Laxminarayan et al., 2013). Therefore, to emphasise more on this, the present study assesses what factors fuel antimicrobial resistance globally and how it is contributing to the economic and clinical burden. For this purpose, the research applies a systematic review technique to assess the factors and the associated burdens.
Research approach and design
The study has used a qualitative research approach in order to investigate factors which contribute to the AMR crisis and how this crisis has resulted in increased economic and clinical costs. The qualitative research is deemed appropriate for the study as the objectives of the research do not include specific statistical measurement. Considering the nature of the qualitative approach, it helps the study to focus on drawing suppositions from different social meaning and settings. For this reason, the study performs a systematic review underlying its qualitative research approach.
Literature search
The systematic qualitative research is conducted through identifying articles which are related to the field of AMR explained as a crisis and its economic and clinical consequences. The articles which were searched for ensured to be between 2008 to 2019, from Google Scholar, International Healthcare Journals Online as well as other global healthcare official websites such as The Lancet Infectious Diseases Commission, Centres for Disease Control and Prevention (CDC), and World Health Organisation (WHO). The articles and information published within these sites and journals were found to be relevant by searching for relevant keywords, such as; Antimicrobial Resistance, AMR crisis, Antibiotic Resistance, Factors of Antimicrobial Resistance, Causes of Antimicrobial Resistance, Consequences of AMR Infection, AMR Economic Cost, Economic Burden and Clinical Burden of AMR.
Inclusion criteria
Articles which included reviews and reported evidence of AMR crisis were included in the systematic qualitative review of the present research if they matched the following predefined study sample criteria:
(i) Reported trends of growing AMR infection among individuals around the globe
(ii) Were published at and after 2008.
(iii) Studied AMR from a global, economic, social and political point of view rather than just biological.
(iv) The research process and technique, sample size, conclusion and literature review were clearly reported in them
Data extraction and analysis
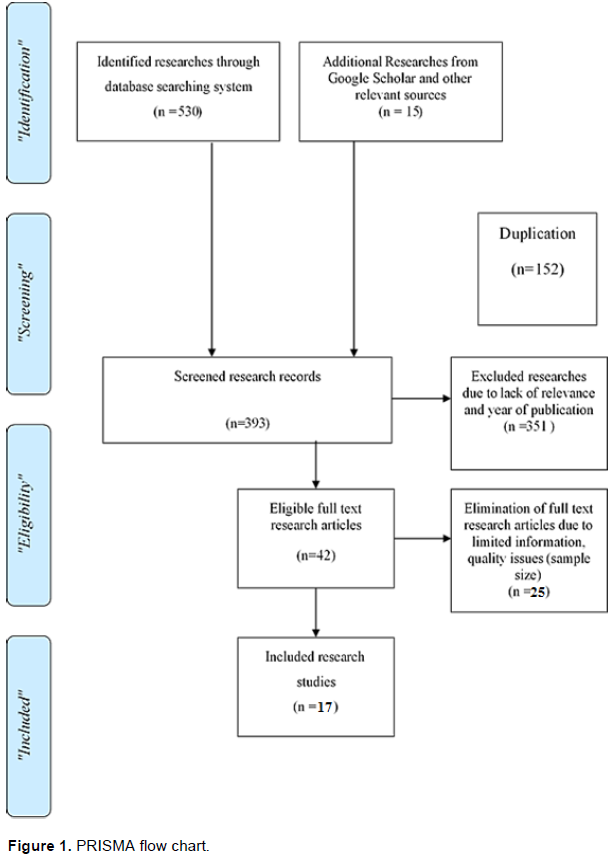
With the purpose to select the relevant research material having high quality for the current study, the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) approach was undertaken to extract the data. PRISMA approach assists the researcher to filter out research articles having inappropriate quality and information (Figure 1).
Initially, after a thorough search, the researchers were able to extract 545 citations, from which 152 duplicates were excluded. In the second step, the researcher reviewed 393 non-duplicate abstracts and excluded 351 abstracts due to lack of relevance, and the required period of study (criteria 2). Finally, the researchers reviewed 42 full-text papers; however, based on the aforementioned criteria (1, 3 and 4) and due to limited information related to the research problem, the sample size of the paper was reduced to 14 only, which were considered for analysis. The papers meeting the criteria were analysed and evaluated on the basis of their year of publication, location of study, method of testing and the findings. The data was then analysed using descriptive analysis technique and was discussed based on findings derived from the studies using a systematic review of the selected papers (Tables 1 and 2).
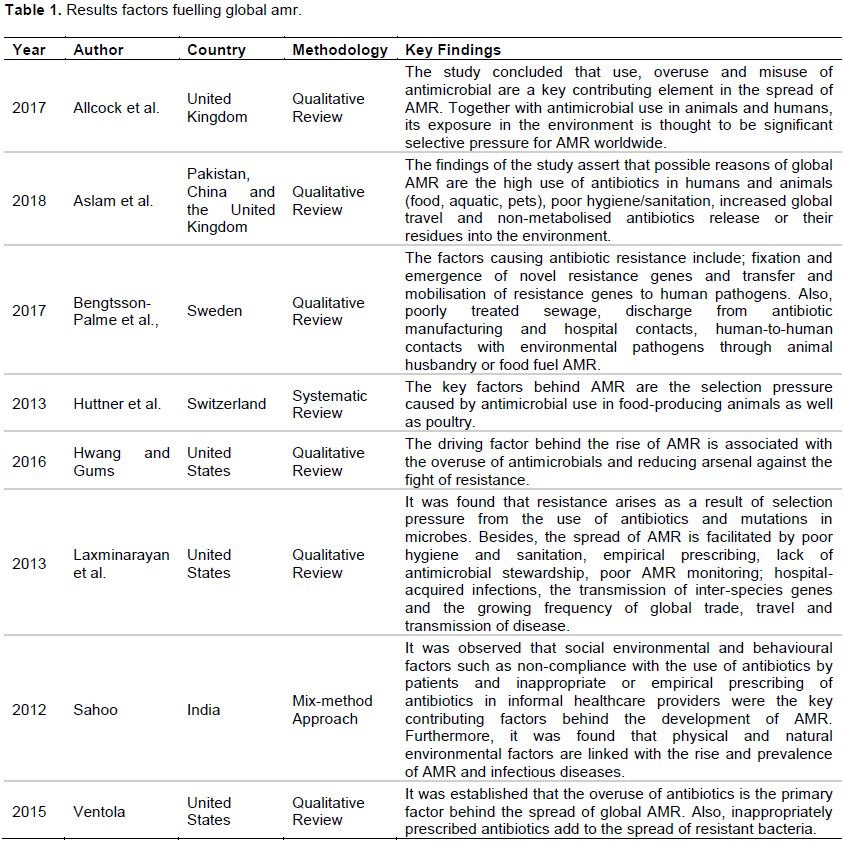
The table exhibits the list of studies which were reviewed to evaluate the factors that cause global antimicrobial resistance and the impact of these factors on the economic and clinical burden. For this reason, the systematic theme-based review is divided into two parts; namely the factors and the second one being the economic and clinical burdens.
The rapidly growing issue of antimicrobial resistance has become a major concern for governments around the world and authorities which are responsible for Global public healthcare. The major factor which has a substantial level of impact on an individual’s health and causes infectious diseases is the environment that the individual resides in or is exposed to. Consequently, many professionals and researchers under this domain have identified environmental components to be a significant factor associated with antibiotic resistance. For example, the study of Sahoo (2012) highlighted the impact of the environment as a key driver in spreading AMR. Previous research suggests that aside from natural and physical environmental factors that influence antibiotic resistance development, behavioural and social factors also play a role (Pruden et al., 2012). Moreover, the factor of geographical variation is also important in antibiotic resistance. According to Parveen (2006), similar geographical variation in antibiotic resistance and agricultural factors is an environment to host antimicrobial-resistant bacteria. It is further explained that in many regions especially developing countries, easy access to first-line and second-line antibiotics and dispensing of antibiotics without prescriptions is a key driver and also limited options (Schwartz et al., 2018). Healthcare professionals are accustomed to using cheaper, ineffective and toxic antibiotics (referred to as biological substances before being healing compounds), and are considered toxic for clinical use like the antiparasitic or antiviral agent, (Rolain and Baquero, 2016), on patients hence increasing the antibiotic resistance of bacteria (Ventola, 2015).
Furthermore, other factors which contribute to the increasing crisis of antimicrobial resistance include the population levels in different geographical regions and human behaviours on various societal levels (Allcock et al., 2017). Similarly, as discussed in the table, the research of Aslam et al (2018) also highlighted factors similar to those documented in Parveen et al. (2006)’s study. The study drew conclusions upon the basis of unavailability of newer and advanced drugs due to regulatory requirements and a decrease in financial funding from the nations on research and development of new antibiotics with novel chemical structures. Hence these factors together fuel antimicrobial resistance thereby, increasing the global crisis.
Overall, the common factor which was found to be propelling the AMR crisis is the lack of knowledge of ways in which environment can affect health and antibodies. Further, agricultural and climate change is also the factor behind the growth of such bacteria (Laxminarayan et al., 2013; Hwang and Gums, 2016; Huttner et al., 2013). From the conclusion of these studies, it can be implied that the issue can be addressed by multidisciplinary approaches across health care institutions and environmental and agricultural sectors. Hence, governments and public healthcare regulatory bodies can implement these findings to minimise the factors and make people aware of the scourge. Besides, the recognition and identification of these factors can help to examine different approaches which will combat the rising problem of antimicrobial resistance, from social and as well as healthcare point of view (Ohl and Dodds, 2011).
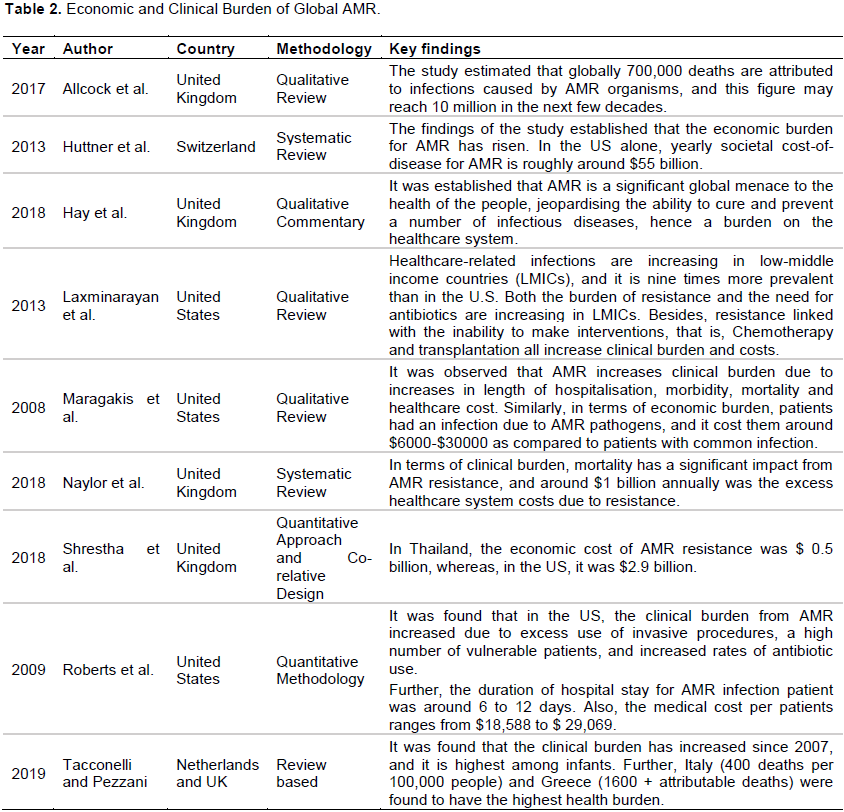
AMR crisis is gaining much attention from healthcare professionals, researchers and government due to the economic burden it poses on a country nationwide, as well as to the patients infected by it and to their families. For example, according to the studies of Aslam et al. (2018); Naylor et al. (2018) and Allcock et al. (2017), the clustering of patients who are vulnerable to AMR in hospitals was resource-intensive, thereby requiring extensive use of aggressive treatments which require millions of funds for the patients’ family to pay. It also increases the burden on hospitals and clinics to efficiently keep their resources stocked up in case of emergencies.
These scenarios were further evidenced by healthcare regulatory bodies such as Centres for Disease Control and Prevention. They explained that even in nations where effective drugs are being used, records showed that patients taking such treatments were required to stay longer in hospitals, have to make more routine visits to the doctor and long-term recuperation (Centres for Disease Control and Prevention, 2013). It eventually exhausts the resources for other patients with severe diseases.
Further, it was reported by Wright (2014) and Bartlett et al. (2013) that the total economic burden measured on the economy of the US by AMR ranged from $18,588 to $29,069. The findings of AMR being an economic and clinical burden are further reinforced by the studies of Shrestha et al. (2018) whereby the researcher concluded that oftentimes the economic costs of consuming antibiotic by each AMR patient were considerably exceeding the purchase costs of it; although measuring the economic cost and clinical burden is a challenge identified by Maragakis et al. (2008). The study also strengthened the argument that AMR crisis has a significant impact on economic and clinical burden by explaining that the cost of patients exposed to AMR infections is higher compared to those patients who are not infected by AMR pathogen.
Similarly, Hay et al. (2018) asserted that AMR is a global threat to wellbeing and health of people, damaging the ability to prevent and cure infectious diseases; therefore, it is now considered as an economic burden on healthcare facilities. Similarly, Tacconelli and Pezzani (2019) concluded that since 2007, the clinical burden has increased, and it is highest among infants. Major European countries like Greece and Italy recorded the highest health burdens due to AMR. In terms of the U.S, Roberts et al. (2009) assert that the clinical burden from AMR has increased significantly, largely because of invasive procedures and increasing rates of antibiotic use. Hence, it can be concluded based on these studies, AMR is fuelling globally due to factors as mentioned earlier and is exerting serious economic and clinical burden on the healthcare system and the people.
The study aims to assess the factors behind the global spread of AMR and its clinical and economic burden. The study used a systematic review technique to determine the factors and clinical and economic burden of AMR. Several factors behind the global of the spread of AMER were found using data of 14 relevant journal articles such as; delay in proper antimicrobial treatment; hospital-acquired infections, travel and transmission of disease, poorly treated sewage, empirical prescribing, lack of antimicrobial stewardship, poor AMR monitoring etc. From the review of the studies, it was found that there is a significant economic and clinical burden of AMR infections, that is, high costs of medical treatment around $18, 000 to $29,000 per patient and 6 to 12 days of hospital stays. Therefore, we recommend that well organised antimicrobial stewardship be in place, AMR monitoring, limited access to antibiotics over the counter without prescriptions, mandatory sensitivity tests for the antimicrobial prescription is required to reduce global AMR. It is also further recommended that proper hygiene in hospitals must be ensured to reduce AMR infections, and this can all be done by coordinated actions at a national and global level.
The study has some limitations as it was review-based research and concluded its findings based on already established facts. Therefore, a primary data-based quantitative approach using an experiment or survey strategy would be significant in acquiring fresh data regarding the spread of AMR and its burden on health and economy. For further research, more studies should be carried out. To achieve more comprehensive findings and provide actionable recommendations on the basis of those findings, which can be implemented at the global level.
The authors have not declared any conflict of interests.
REFERENCES
|
Allcock S, Young EH, Holmes M, Gurdasani D, Dougan G, Sandhu MS, Solomon L, Török ME (2017). Antimicrobial resistance in human populations: challenges and opportunities. Global Health, Epidemiology and Genomics 2.
Crossref
|
|
|
|
Aslam B, Wang W, Arshad MI, Khurshid M, Muzammil S, Rasool MH, Nisar MA, Alvi RF, Aslam MA, Qamar MU, Salamat MKF (2018). Antibiotic resistance: a rundown of a global crisis. Infection and Drug Resistance 11:1645.
Crossref
|
|
|
|
|
Bartlett JG, Gilbert DN, Spellberg B (2013). Seven ways to preserve the miracle of antibiotics. Clinical Infectious Diseases 56(10):1445-1450.
Crossref
|
|
|
|
|
Bengtsson-Palme J, Kristiansson E, Larsson DJ (2017). Environmental factors influencing the development and spread of antibiotic resistance. FEMS Microbiology Reviews 42(1):fux053.
Crossref
|
|
|
|
|
Centres for Disease Control and Prevention (2013). Antibiotic / Antimicrobial Resistance (AR/AMR). Retrieved from:
View
|
|
|
|
|
ECDC (2015). European food safety authority, the European centre for disease prevention and control: the European Union summary report on trends and sources of zoonoses, zoonotic agents and food-borne outbreaks in 2013. EFSA Journal 13:3991.
Crossref
|
|
|
|
|
Hay SI, Rao PC, Dolecek C, Day NP, Stergachis A, Lopez AD, Murray CJ (2018). Measuring and mapping the global burden of antimicrobial resistance. BMC Medicine 16(1):78.
Crossref
|
|
|
|
|
Huttner A, Harbarth S, Carlet J, Cosgrove S, Goossens H, Holmes A, Jarlier V, Voss A, Pittet D (2013). Antimicrobial resistance: a global view from the 2013 World Healthcare-Associated Infections Forum. Antimicrobial Resistance and Infection Control 2(1):31.
Crossref
|
|
|
|
|
Hwang AY, Gums JG (2016). The emergence and evolution of antimicrobial resistance: Impact on a global scale. Bioorganic and Medicinal Chemistry 24(24):6440-6445.
Crossref
|
|
|
|
|
KPMG L (2014). The Global Economic Impact of Anti-microbial Resistance. KPMG LLP.
|
|
|
|
|
Landers TF, Cohen B, Wittum TE, Larson EL (2012). A review of antibiotic use in food animals: perspective, policy, and potential. Public Health Reports 127(1):4-22.
Crossref
|
|
|
|
|
Laxminarayan R, Duse A, Wattal C, Zaidi AK, Wertheim HF, Sumpradit N, Vlieghe E, Hara GL, Gould IM, Goossens H, Greko C (2013). Antibiotic resistance-the need for global solutions. The Lancet Infectious Diseases 13(12):1057-1098.
Crossref
|
|
|
|
|
Maragakis LL, Perencevich EN, Cosgrove SE (2008). Clinical and economic burden of antimicrobial resistance. Expert Review of Anti-Infective Therapy 6(5):751-763.
Crossref
|
|
|
|
|
Naylor NR, Atun R, Zhu N, Kulasabanathan K, Silva S, Chatterjee A, Knight GM, Robotham JV (2018). Estimating the burden of antimicrobial resistance: a systematic literature review. Antimicrobial Resistance and Infection Control 7(1):58.
Crossref
|
|
|
|
|
O'Neill JIM (2014). Antimicrobial resistance: tackling a crisis for the health and wealth of nations. Review on Antimicrobial Resistance 20:1-16.
|
|
|
|
|
Ohl CA, Dodds AES (2011). Antimicrobial stewardship programs in community hospitals: the evidence base and case studies. Clinical Infectious Diseases 53(suppl_1):S23-S28.
Crossref
|
|
|
|
|
Parveen S, Lukasik J, Scott TM, Tamplin ML, Portier KM, Sheperd S, Farrah SR (2006). Geographical variation in antibiotic resistance profiles of Escherichia coli isolated from swine, poultry, beef and dairy cattle farm water retention ponds in Florida 1. Journal of Applied Microbiology 100(1): 50-57.
Crossref
|
|
|
|
|
Pruden A, Arabi M, Storteboom HN (2012). Correlation between upstream human activities and riverine antibiotic resistance genes. Environmental Science and Technology 46(21):11541-11549.
Crossref
|
|
|
|
|
Roberts RR, Hota B, Ahmad I, Scott RD, Foster SD, Abbasi F, Schabowski S, Kampe LM, Ciavarella GG, Supino M, Naples J (2009). Hospital and societal costs of antimicrobial-resistant infections in a Chicago teaching hospital: implications for antibiotic stewardship. Clinical Infectious Diseases 49(8):1175-1184.
Crossref
|
|
|
|
|
Rolain JM, Baquero F (2016). The refusal of the society to accept antibiotic toxicity: missing opportunities for therapy of severe infections. Clinical Microbiology and Infection 22(5):423-427.
Crossref
|
|
|
|
|
Sahoo KC (2012). Antibiotic resistance and environmental factors: focusing on the situation in Odisha, India. Inst för folkhälsovetenskap/Dept of Public Health Sciences.
|
|
|
|
|
Schwartz KL, Achonu C, Brown KA, Langford B, Daneman N, Johnstone J, Garber G (2018). Regional variability in outpatient antibiotic use in Ontario, Canada: a retrospective cross-sectional study. CMAJ Open 6(4):E445.
Crossref
|
|
|
|
|
Shrestha P, Cooper BS, Coast J, Oppong R, Thuy NDT, Phodha T, Celhay O, Guerin PJ, Wertheim H, Lubell Y (2018). Enumerating the economic cost of antimicrobial resistance per antibiotic consumed to inform the evaluation of interventions affecting their use. Antimicrobial Resistance and Infection Control 7(1):98.
Crossref
|
|
|
|
|
Smith RD, Coast J (2012). The economic burden of antimicrobial resistance: why it is more serious than current studies suggest. Technical Report. London School of Hygiene and Tropical Medicine, London.
|
|
|
|
|
Tacconelli E, Pezzani MD (2019). Public health burden of antimicrobial resistance in Europe. The Lancet Infectious Diseases 19(1):4-6.
Crossref
|
|
|
|
|
Tam CC, O'Brien SJ (2016). The economic cost of campylobacter, norovirus and rotavirus disease in the United Kingdom. PloS One 11(2):e0138526.
Crossref
|
|
|
|
|
Taylor J, Hafner M, Yerushalmi E, Smith R, Bellasio J, Vardavas R, Bienkowska-Gibbs T, Rubin J (2014). Estimating the economic costs of antimicrobial resistance: model and results. Santa Monica, CA: RAND Corporation.
|
|
|
|
|
Ventola CL (2015). The antibiotic resistance crisis: part 1: causes and threats. Pharmacy and Therapeutics 40(4):277.
|
|
|
|
|
World Health Organization (WHO) (2017). What is antimicrobial resistance? Retrieved from
View
|
|
|
|
|
Wright GD (2014). Something old, something new: revisiting natural products in antibiotic drug discovery. Canadian Journal of Microbiology 60(3):147-154.
Crossref
|
|