Full Length Research Paper

ABSTRACT
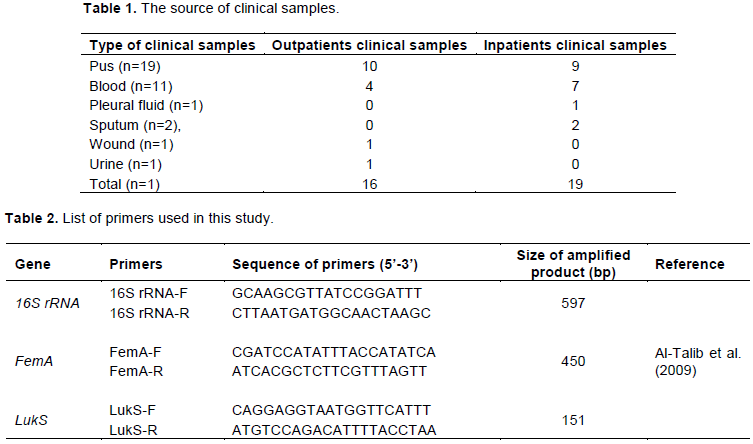
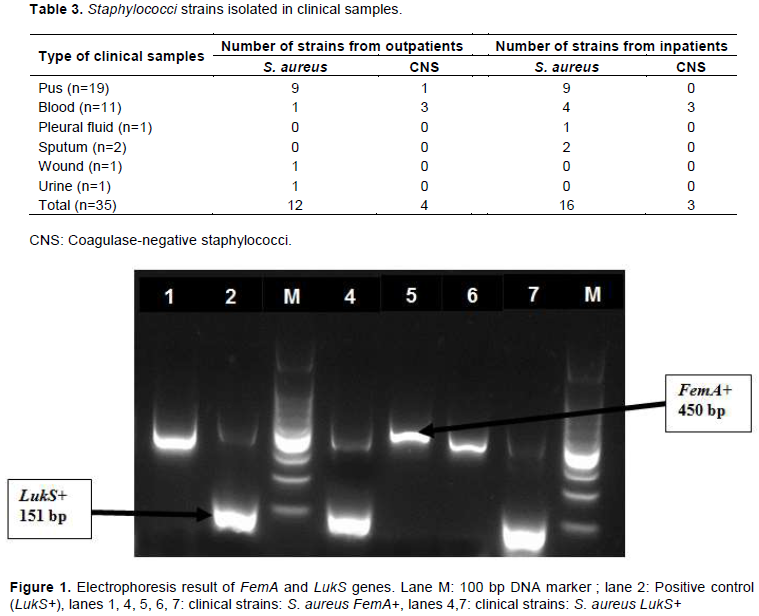
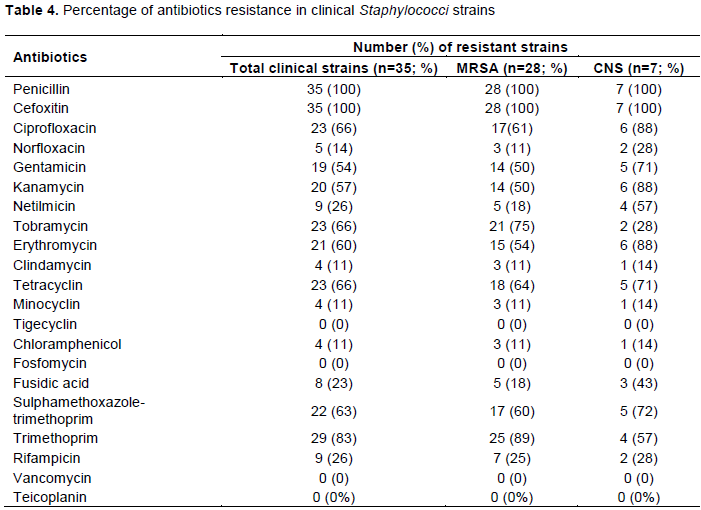
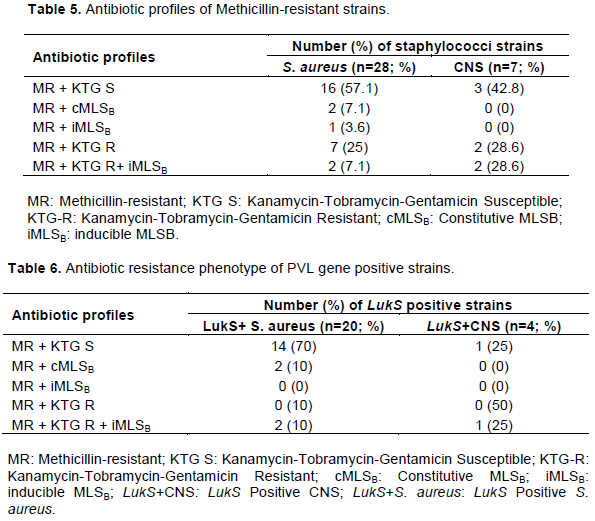
Methicillin-resistant staphylococci have emerged as significant pathogens which cause various infections and its multidrug resistance is a major concern. This study aimed to determine the prevalence of Panton-Valentine leukocidin (PVL) gene and antibiotic resistance patterns of staphylococci isolated from clinical infections in Abidjan. A total of 35 staphylococci strains was obtained from 35 clinical samples (pus, blood, pleural fluid, sputum, wound, and urine), then, characterized by polymerase chain reaction (PCR) to differentiate S. aureus from coagulase-negative staphylococci (CNS) and to detect the presence of PVL genes (LukS). The antimicrobial susceptibility was performed using disk diffusion method and the phenotype of resistance to macrolides-lincosamides-streptogramin B (MLSB) was detected. Out of 35 strains, 80% (28/35) were methicillin-resistant Staphylococcus aureus (MRSA) and 20% (7/35) were methicillin-resistant CNS (MR-CNS). S. aureus were isolated from 75% of outpatient samples and 84.2% of inpatient samples. However, CNS were isolated from 25% of outpatient samples and 15.8% of inpatient samples. LukS were detected in 68.6% of strains (20 MRSA and 4 MR-CNS) and both inpatients and outpatients. The highest resistance rates were observed for penicillin (100%), cefoxitin (100%), ciprofloxacin (66%), tobramycin (66%), tetracyclin (66%), sulphamethoxazole-trimethoprim (63%), erythromycin (60%), kanamycin (57%) and gentamicin (54%). In addition, S. aureus strains were subdivided into five antibiotics resistance phenotypes: 57.1% belonged to phenotype 1 (Methicillin-resistant and susceptible to Kanamycin-Tobramycin-Gentamicin) followed by 25% of phenotype 4 (Resistant to Methicillin-Kanamycin-Tobramycin-Gentamicin), 7.1% of phenotype 2 (MR with constitutive MLSB), 7.1% of phenotype 5 (MR and resistant to Kanamycin-Tobramycin-Gentamicin with inducible MLSB) and 3.6% of phenotype 3 (MR with inducible MLSB). CNS strains were grouped in three phenotypes (1, 4 and 5). 100% of LukS positive MRSA were multi-drug resistant, with 45% of strains resistant to 6 or more antibiotics. The high level of multi-drug resistance of clinical PVL positive staphylococci with inducible MLSB, suggest increasing the monitoring of these pathogens in Côte d’Ivoire.
Key words: Methicillin-resistant Staphylococcus aureus (MRSA), Panton-Valentine Leukocidin, inducible MLSB, multi-drug resistance.
INTRODUCTION
MATERIALS AND METHODS
RESULTS
DISCUSSION
CONCLUSION
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGEMENTS
REFERENCES
|
Abdollahi S, Ramazanzadeh R, Khiabani ZD, Kalantar E (2016). Epidemiological and Inducible Resistance in Coagulase Negative Staphylococci. Global Journal of Health Science 8(4):109. |
|
|
Abdulgader SM, Shittu AO, Nicol MP, Kaba M (2015). Molecular epidemiology of Methicillin-resistant Staphylococcus aureus in Africa: a systematic review. Frontiers in Microbiology 6:348. |
|
|
Al-Talib H, Yean CY, Al-Khateeb A, Hassan H, Singh K K, Al-Jashamy K, Ravichandran M (2009). A pentaplex PCR assay for the rapid detection of methicillin-resistant Staphylococcus aureus and Panton-Valentine Leucocidin. BMC Microbiology 9:113. |
|
|
Amini R, Abdulamir AS, Ling BP, Jahanshiri F, Hematian A, Zargar M, Sekawi Z, Jalilian FA (2012). Isolation and identification of methicillin-resistant Staphylococcus aureus from keys of college students using different detection methods. British Biotechnology Journal 2(1):13-25 |
|
|
Amissah NA, van Dam L, Ablordey A, Ampomah O-W, Prah I, Tetteh CS, van der Werf TS, Friedrich AW, Rossen JW, van Dijl JM, Stienstra Y (2017). Epidemiology of Staphylococcus aureus in a burn unit of a tertiary care center in Ghana. PLoS ONE 12(7):e0181072. |
|
|
Asiimwe BB, Baldan R, Trovato A, Cirillo DM (2017). Molecular epidemiology of Panton-Valentine Leukocidin-positive community-acquired methicillin resistant Staphylococcus aureus isolates in pastoral communities of rural south western Uganda. BMC Infectious Diseases 17:24. |
|
|
Bhattacharya S, Bir R, Majumdar T (2015). Evaluation of Multidrug Resistant Staphylococcus aureus and their Association with Biofilm Production in a Tertiary Care Hospital, Tripura, Northeast India. Journal of Clinical and Diagnostic Research 9(9):DC01-DC04 |
|
|
Bhatta DR, Cavaco LM, Nath G, Kumar K, Gaur A, Gokhale S, Bhatta DR (2016). Association of Panton Valentine Leukocidin (PVL) genes with methicillin resistant Staphylococcus aureus (MRSA) in Western Nepal: a matter of concern for community infections (a hospital based prospective study). BMC Infectious Diseases 16:199. |
|
|
Boswihi SS, Udo EE, Monecke S, Mathew B, Noronha B, Verghese T, Tappa SB (2018). Emerging variants of methicillin-resistant Staphylococcus aureus genotypes in Kuwait hospitals. PLoS One 13:e0195933. |
|
|
Bottega A, Rodrigues MA, Carvalho FA, Wagner TF, Leal IAS, dos Santos SO, Rampelotto RF, Hörner R (2014). Evaluation of constitutive and inducible resistance to clindamycin in clinical samples of Staphylococcus aureus from a tertiary hospital. Revista da Sociedade Brasileira de Medicina Tropical 47(5):589-592. |
|
|
Chen X, Wu Z, Zhou Y, Zhu J, Li K, Shao H, Wei L (2017). Molecular and virulence characteristics of methicillin-resistant Staphylococcus aureus in burn patients. Frontiers Laboratory Medecine 1:43-47. |
|
|
Committee of antibiogram of French Society of Microbiology (CA-SFM) /European Committee on Antimicrobial Susceptibility Testing (EUCAST). Recommandations.Version 1.0 February 2016. |
|
|
Dekker D, Wolters M, Mertens E, Boahen K, Krumkamp R, Eibach D, Schwarz NG, Adu-Sarkodie Y, Rohde H, Christner M, Marks F, Sarpong N, May J (2016). Antibiotic resistance and clonal diversity of invasive Staphylococcus aureus in the rural Ashanti Region, Ghana. BMC Infectious Diseases 16:720-726. |
|
|
Dong J, Quiu J, Li H, Dai X, Zhang Y, Tan W, Niu X, Deng X, Zhao S (2013). Apigenin alleviates the symptoms of Staphylococcus aureus pneumonia by inhibiting the production of alpha-hemolysin. FEMS Microbiology Letters 338:124-131. |
|
|
Egyir B, Guardabassi L, Sørum M, Nielsen SS, Kolekang A, Frimpong E, Addo KK, Newman MJ, Larsen AR (2014). Molecular epidemiology and antimicrobial susceptibility of clinical Staphylococcus aureus from Healthcare Institutions in Ghana. PLoS ONE 9:e89716 |
|
|
Kacou NA, Koffi KS, Ekaza E, Kouamé- Elogne C, Anne BJC, Dosso M (2011). Staphylococcus aureus infection and virulence genes in Abidjan (Côte d'Ivoire). European Journal of scientific Research 52:339-344. |
|
|
Kaspar U, Kriegeskorte A, Schubert T, Peters G, Rudack C, Pieper DH, Wos-Oxley M, Becker K (2016). The culturome of the human nose habitats reveals individual bacterial Fingerprint patterns. Environmental Microbiology 18:2130-2142. |
|
|
Kateete DP, Kimani CN, Katabazi FA, Okeng A, Okee MS, Nanteza A, Joloba ML, Najjuka FC (2010). Identification of Staphylococcus aureus: Dnase and mannitol salt agar improve the efficiency of the tube coagulase test. Annals of Clinical Microbiology and Antimicrobials 9:23-29. |
|
|
Kpeli G, Otchere I D, Lamelas A, Buultjens A L, Bulach D, Baines SL, Seemann T, Giulieri S, Nakobu Z, Aboagye SY, Owusu-Mireku E, Pluschke G, Stinear TP, Yeboah-Manu D (2016). Possible healthcare-associated transmission as a cause of secondary infection and population structure of Staphylococcus aureus isolates from two wound treatment centres in Ghana. New Microbes and New Infections 13:92-101. |
|
|
Kumari J, Shenoy SM, Baliga S, Chakrapani M, Bhat GK (2016). Healthcare-Associated Methicillin-Resistant Staphylococcus aureus Clinical characteristics and antibiotic resistance profile with emphasis on macrolide-lincosamide-streptogramin B resistance. 2016. Sultan Qaboos University Medecine Journal 16:175-181. |
|
|
Lai PS, Bebell LM, Meney C, Valeri L, White MC (2018). Epidemiology of antibiotic-resistant wound infections from six countries in Africa. BMJ Global Health 2:e000475. |
|
|
Lenart-Boron A, Wolny-Koladka K, Stec J, Kasprowic A (2016). Phenotypic and molecular antibiotic resistance determination of airborne coagulase negative Staphylococcus spp. strains from healthcare facilities in Southern Poland. Microbial Drug Resistance 22:515-522. |
|
|
Lesens O, Haus-Cheymol R, Dubrous P, Verret C, Spiegel A, Bonnet R, Bes M, Laurichesse H, Beytout J, Etienne J, Migliani R, Koeck JL, the Working Group on Cutaneous Infections in the Army (2007). Methicillin susceptible, Doxycycline resistant Staphylococcus aureus, Côte d'Ivoire. Emerging Infectious Diseases 13:488-490. |
|
|
Liu C, Bayer A, Cosgrove SE, Daum RS, Fridkin SK, Gorwitz RJ, Kaplan SL, Karchmer AW, Levine DP, Murray BE, Rybak M J, Talan DA, Chambers HF (2011). Clinical practice guidelines by the Infectious Diseases Society of America for the treatment of methicillin-resistant Staphylococcus aureus infections in adults and children. Clinical Infectious Diseases 52:285-292. |
|
|
Magiorakos A, Srinivasan A, Carey RB, Carmeli Y, Falagas ME, Giske CG, Harbarth S, Hindler JF, Kahlmeter G, Olsson-Liljequist B, Paterson DL, Rice LB, Stelling J, Struelens MJ, Vatopoulos A, Weber JT, Monnet DL (2011). Multidrug resistant, extensively drug-resistant and pandrug-resistant bacteria: an international expert proposal for interim standard definitions for acquired resistance. Clinical Infectious Diseases 18:268-281. |
|
|
Maheshwari V, Kaore NCM, Ramani VK, Gupta SK, Borle A, Kaushal R (2014). A study to assess knowledge and attitude regarding hand hygiene amongst residents and nursing staff in a teritiary care setting of hospital city. Journal of Clinical and Diagnostic Research 8:DC04-07. |
|
|
Messina JA, Thaden JT, Sharma-Kuinkel BK, Fowler Jr VG (2016). Impact of bacterial and human genetic variation on Staphylococcus aureus infections. PLoS Pathogens 12:e1005330. |
|
|
Nanoukon C, Argemi X, Sogbo F, Orekan J, Keller D, Affolabi D, Schramm F, Riegel P, Baba-Moussa L, Pre’vost G (2017). Pathogenic features of clinically significant coagulase-negative Staphylococci in hospital and community infections in Benin. International Journal of Medical Microbiology 307:75-82. |
|
|
Oliveira CF, Paim TGS, Reiter KC, Rieger A, D'azevedo PA (2014). Evaluation of four different DNA extraction methods in coagulase-negative staphylococci clinical isolates. Revista do Instituto de Medicina Tropical de São Paulo 56(1):29-33. |
|
|
Ouedraogo A-S, Dunyach-Remy C, Kissou A, Sanou S, Poda A, Kyelem CG, Solassol J, A-L Ba-uls, Van De Perre P, Ouédraogo R, Jean-Pierre H, Lavigne J-P, Godreuil S (2016). High Nasal Carriage Rate of Staphylococcus aureus Containing Panton-Valentine leukocidin- and EDIN-Encoding Genes in Community and Hospital Settings in Burkina Faso. Frontiers in Microbiology 7:1406. |
|
|
Pedroso S HSP, Sandes SHC, Filho RAT, Nunes A C, Serufo JC, Farias LM, Carvalho MAR, Bomfim MRQ, Santos SG (2018). Coagulase-Negative Staphylococci Isolated from Human Bloodstream Infections Showed Multidrug Resistance Profile. Microbial Drug Resistance 24:635-647. |
|
|
Pereira JN, Rabelo MA, Lima JL, Neto AM, Lopes AC, Maciel MA (2016). Phenotypic and molecular characterization of resistance to macrolides, lincosamides and type B streptogramin of clinical isolates of Staphylococcus spp. of a university hospital in Recife, Pernambuco, Brazil. The Brazilian Journal of Infectious Diseases 20:276-281. |
|
|
Saba CKS, Amenyona JK, Kpordze SW (2017). Prevalence and pattern of antibiotic resistance of Staphylococcus aureus isolated from door handles and other points of contact in public hospitals in Ghana. Antimicrobial Resistance and Infection Control 6:44. |
|
|
Samutela MT, Kalonda A, Mwansa J, Lukwesa-Musyani C, Mwaba J, Mumbula EM, Mwenya D, Simulundu E, Kwenda G (2017). Molecular characterisation of methicillin-resistant Staphylococcus aureus (MRSA) isolated at a large referral hospital in Zambia. PanAfrican Medical Journal 26:108. |
|
|
Shallcross LJ, Fragasz E, Johnson AM, Hayward AC (2013). The role of the Panton-Valentine leucocidin toxin in staphylococcal disease: A systematic review and meta-analysis. Lancet Infectious Diseases 13:43-54. |
|
|
Shittu A, Oyedara O, Abegunrin F, Okon K, Raji A, Taiwo S, Ogunsola F, Onyedibe K, Elisha G (2012). Characterization of methicillin-susceptible and resistant Staphylococci in the clinical setting: a multicentre study in Nigeria. BMC Infectious Diseases 12:286. |
|
|
Shopsin B, Kaveri SV, Bayry J (2016). Tackling difficult Staphylococcus aureus infections: antibodies show the way. Cell Host Microbe 20: 555-557. |
|
|
Skov R, Christiansen K, Dancer SJ, Daum RS, Dryden M, Huang YC, Lowy FD (2012). Update on the prevention and control of community acquired meticillin-resistant Staphylococcus aureus (CA-MRSA). International Journal of Antimicrobial Agents 39:193-200. |
|
|
Tanwar J, Das S, Fatima Z, Hameed S (2014). Multidrug resistance: An emerging crisis. Interdisciplinary Perspectives on Infectious Diseases 2014:1-7. |
|
|
Tong SYC, Davis JS, Eichenberger E, Holland TL, Fowler Jr VG (2015). Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clinical Microbiology Reviews 28:603-661. |
|
|
van der Meeren BT, Millard PS, Scacchetti M, Hermans MH, Hilbink M, Concelho TB, Ferro JF, Wever PC (2014). Emergence of methicillin resistance and Panton-Valentine leukocidin positivity in hospital- and community-acquired Staphylococcus aureus infections in Beira, Mozambique. Tropical Medicine and International Health 19:169-176. |
|
|
Vandendriessche S, De Boeck H, Deplano A, Phoba M, Lunguya O, Falay D, Dauly N, Verhaegen J, Denis O, Jacobs J (2017). Characterisation of Staphylococcus aureus isolates from bloodstream infections, Democratic Republic of the Congo. European Journal of Clinical Microbiology and Infectious Diseases 36:1163-1171. |
|
|
Willyard C (2017). The drug-resistant bacteria that pose the greatest health threats. Nature 543:15. |
|
|
World Health Organization (WHO) (2014). Antimicrobial resistance: global report on surveillance. Geneva, Switzerland. |
|
|
Yanagihara K, Kihara R, Araki N, Morinaga Y, Seki M, Izumikawa K, Kakeya H, Yamamoto Y, Yamada Y, Kohno S, Tsukamoto K, Kamihira S (2009). Efficacy of linezolid against Panton-Valentine leukocidin (PVL)-positive meticillin-resistant Staphylococcus aureus (MRSA) in a mouse model of haematogenous pulmonary infection. International Journal of Antimicrobial Agents 34:477-481. |
|
|
Zinzendorf NY, Krizo A, Baba-Moussa L, Edoh V, Loukou YG (2012). Molecular Characteristics of Staphylococcus aureus from Military Hospital in Abidjan, Côte d'Ivoire. Bulletin of Environment, Pharmacology and Life Sciences 1:54-58. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


