ABSTRACT
The antimicrobial inhibitory effects of five common antiseptics [Chlorhexidine (CHX), Hydrogen peroxide (H2O2), Iodine, Ethanol and Dettol] were investigated using agar well diffusion method. The organisms used included methicillin-resistant Staphylococcus aureus (MRSA), Acinetobacter baumannii, Escherichia coli, Klebsiella species and Pseudomonas aeruginosa. The undiluted concentrations of the antiseptics showed variable zones of inhibition against the tested organisms, on MRSA it ranged from 25 mm (CHX) to 30 mm in other antiseptics, on A. baumannii 20 mm (CHX) to 34 mm Dettol, on E. coli 20 mm Dettol to 38 mm (H2O2), on Klebsiella spp. 20 mm Dettol to 24 mm (CHX), whereas on P. aeruginosa it ranged from 13 mm Iodine to 30 mm (H2O2). The minimal inhibitory concentration (MIC) of chlorhexidine concentration against MRSA and P. aeruginosa was 10%, while A. baumannii was 20%. All the study bacteria were resistant to ethanol by all concentrations. The result showed that H2O2 was the most effective antiseptics than the others followed by CHX. The study bacteria were found to be crucially susceptible to the routinely used antiseptics tested. Though, there is the need for continuous surveillance for the detection of emerging resistance pattern.
Key words: Antimicrobial, antiseptics, disinfectants, nosocomial.
Nosocomial infections (NI) are referred to those infections occurring after 48 h of hospital admission, or 3 days of discharge (Kouchak and Askarian, 2012). About 10% of the hospital admitted persons will have NI, and it has been shown that NI is usually associated with prolong length of hospital stay, increased costs, and resulted in significant morbidity and mortality (Al-Talib et al., 2010; Raines and Rosen, 2016). Currently, NI has become a trend in healthcare setting globally including Malaysia. Nosocomial bacteria including methicillin-resistant Staphylococcus aureus (MRSA) and Pseudomonas aeruginosa, have become endemic in many health care centres. Infections with these organisms are often difficult to treat, owing to a reducing armamentarium of active antiseptic agents. Also, hospital associated infections involving these and other microorganisms are associated with considerable morbidity and mortality (Climo et al., 2013). Antiseptics and disinfectants had a fundamental role in infection control practices and help in the avoidance of NI. Antiseptics are used in sterilization of medical and surgical instruments and wards equipment. However, extensive using of different antiseptics might lead to the development of resistant pathogens that eventually makes the antiseptics become ineffective (Matthew et al., 2017). Different bacteria showed variable degrees of resistance to antiseptics (McDonnell and Russell, 1999); although, Gram-negative bacteria are commonly more resistant than Gram-positive bacteria to antiseptics (Russell, 1999). Antiseptics are mainly used to inhibit the growth of microorganisms or to interrupt the route of transmission of germs between the infection source and healthy subjects (Mbajiuka et al., 2015). Previous study by El-Mahmood and Doughari (2009) revealed that five frequently used antiseptics were contaminated with nosocomial Gram positive and negative bacteria, therefore, antiseptics used in hospitals and laboratories must be evaluated regularly to determine their potency validation to remove or inactivate known pathogens from inanimate objects (Sridhar, 2012). Chlorhexidine is an antiseptic with a broad-spectrum activity against many organisms, including S. aureus and Enterococcus species. Chlorhexidine is a cationic polybiguanide that has antibacterial effects and has been used as antiseptic in clinical practice (Mullany et al., 2006). Chlorhexidine salts dissociate and release the positively charged chlorhexidine cationic molecules which bind to negatively charged bacterial cell walls and causing bactericidal effect (Cheung et al., 2012). Using chlorhexidine at low concentrations resulted in a bacteriostatic effect while at high concentrations it can cause membrane disruption and cell death. Chlorhexidine lasts much longer than other antiseptics, therefore, it is often combine with alcohol in skin preparation to reduce microbial burden on patients’ skin and prevent secondary bacterial infections (Climo et al., 2013). Previous studies have found that daily bathing with 2% chlorhexidine-im-pregnated washcloths reduced the incidence of NI infections by 60% (Climo et al., 2013; Vernon et al., 2006).
Hydrogen peroxide (H2O2) plays a central role in sterilization and disinfection of critical items in Malaysian hospitals. Also H2O2 is the most effective antiseptic used in hospitals since the 1920s because it kills bacteria cells by destroying their cell walls. H2O2 has “hydroxyl radicals” a potent oxidant, which react with macromolecules such as membrane lipids and DNA thus resulting in bacterial death (Shahriari et al., 2011). In its pure form, H2O2 is a colourless liquid, slightly more viscous than water. H2O2 is used in hospital and ICU in a vapour form to decontaminate rooms from multi-drug resistant, also used to sterile surfaces, including surgical tools (Lemmen et al., 2015).
Nowadays most of the hospital used Iodine (povidone iodine) which is a natural dark violet, non-metallic solution that considered among the most effective skin antiseptics and used widely in minor wound cleaner. Iodine has excellent bactericidal, fungicidal, tuberculocidal, virucidal and sporicidal properties (Bouaziz et al., 2016). Iodine can penetrate the cell wall of microorganisms quickly, and the lethal effects are believed to result from disruption of protein and nucleic acid structure and synthesis (McKeen, 2012). Although, povidone-iodine has a rapid bactericidal effect than chlorhexidine, but povidone-iodine has not been shown to have a persistent effect like chlorhexidine (Bigliardi et al., 2017).
Ethanol is used extensively in the homes, healthcare settings and laboratories. It consists of two water-soluble chemical compounds ethyl alcohol and isopropyl alcohol that have germicidal characteristics. Alcohols showed bactericidal rather than bacteriostatic activities against vegetative forms of bacteria but do not destroy bacterial spores. Hence, alcohol is not generally being used as sterilizing material instrument (Tuhina et al., 2013). Both ethanol and isopropanol have similar modes of action against different types of microorganisms, however isopropyl alcohol is likely to be more effective than ethanol against bacteria, while the reverse appears to be true for viruses (William et al., 2008). Dettol is another antiseptic, which is used in hospitals and homes; it is available in multi-forms like soap, spray, hand wash, surface wipes, mildew remover and a bathroom cleaner. The active ingredient in Dettol is para-chloro-meta-xylenol. Dettol has greater effects against Gram-positive bacteria and works by disruption of the cell wall and inhibiting the function of enzymes (Mahon et al., 2014).
The aim of this study was to evaluate the antimicrobial effects of some commonly used disinfectants and antiseptics against common bacteria that cause nosocomial infections in hospitals.
Antiseptics
This study was conducted in microbiology laboratory at Institute of Medical Molecular Biotechnology, Faculty of Medicine, Universiti Teknologi MARA (UiTM) from February to August 2017. In this study, the same antiseptics which were already used by different wards and Operation Theater in UiTM Private Specialist Centre (PPP-UiTM), Sungai Buloh, Selangor, Malaysia were used. Five commonly used antiseptics and disinfectants were evaluated in this study including Heptin [Chlorhexidine Gluconate 0.5% in alcohol 70% Nanz Med Science Pharma, Himachal Pradesh, India)], Hydrogen peroxide 6% w/v (Wellmex Sdn Bhd, Selangor, Malaysia), Iodine [Povidone Iodine 7.5% w/v (Thermalife, Pinang, Malaysia)], Alcohol [Ethanol 70% v/v Fisher, Loughborough, UK)] and Dettol [Chloroxylenol 4.8% w/v (Reckitt Benckiser, Hull, UK)].
Disinfectant dilution methods
A series of decreasing concentrations of the antiseptics were obtained using serial dilution method in which the original concentration of antiseptic was considered 100%, the subsequent concentration was prepared by adding 9 ml of antiseptic into a tube with 1 ml distilled water to give 90% concentration. Then the rest concentrations were prepared in descending same manner. The antiseptics concentrations used in this study range from 100 to 10%.
Cultivation of bacterial strains
Five bacterial types isolated from UiTM Private Specialist Centre were used in this study including methicillin-resistant S. aureus (MRSA), Acinetobacter baumannii, Escherichia coli, Klebsiella species and P. aeruginosa. Each bacterium was cultured in nutrient agar for 24 h at 37°C. All tested bacteria were maintained in nutrient broth at 4°C and subcultured on Luria Bertani agar plates 24 h prior to any antimicrobial test. Luria Bertani broth was used for all antibacterial testing.
Antimicrobial susceptibility assays
Well diffusion method
Agar well diffusion method was used to determine antimicrobial activity of different antiseptics. Two bacterial colonies were inoculated in Tryptic soy broth for 3 h at 37°C and turbidity was adjusted in phosphate buffered saline to 0.5 McFarland’s scale. 100 μl of bacterial broth was spread on Muller-Hinton agar plates containing ten 6 mm wells. Thirty microliters of each different concentration (10, 20, 30, 40, 50, 60, 70, 80, 90 and 100%) of each antiseptic was poured into each well and these plates were incubated at 37°C aerobically for 24 h. The diameter of the zone of growth inhibition around the wells were measured in millimeters and recorded. Wells containing antiseptics which showed no inhibition zones were considered as negative results. Antibiotic disc was used as positive control.
Minimal inhibitory concentration (MIC)
Broth dilution assay was used to determine the MIC of different antiseptics against bacteria causing nosocomial infections as recommended by the Clinical Laboratory Standards Institute (Wayne, 2012). The concentrations of the antiseptics tested ranged from 100 to 10%. This test was performed in sterile bijou bottles which were loaded with 100 µL of each antiseptic dilution into each bottle.
Bacterial inoculums (100 µL) containing 5 × 105 CFU of each microorganism were added to each bottle (European Society of Clinical Microbiology and Infectious Diseases, 2003). In each panel of the tested antiseptic, a positive control (without antiseptic) and negative control (no inoculum) were added. All bottles were aerobically incubated at 37°C. After incubation for 24 h, the bacterial growth was assayed by its visible turbidity. The highest dilution of the antiseptic which showed no visible bacterial growth and no turbidity in bijou bottle was considered as MIC. After 24 h of incubation, 100 µL of each mixture was pipetted and inoculated on blood agar and spread uniformly with the sterile spreader and again incubated for 24 h at 37°C. On the next day, all blood agars were examined and all bacterial colonies were counted and recorded.
Ethical approval
The study was conducted in accordance with the principles of the Declaration of Helsinki. All participants provided written informed consent.
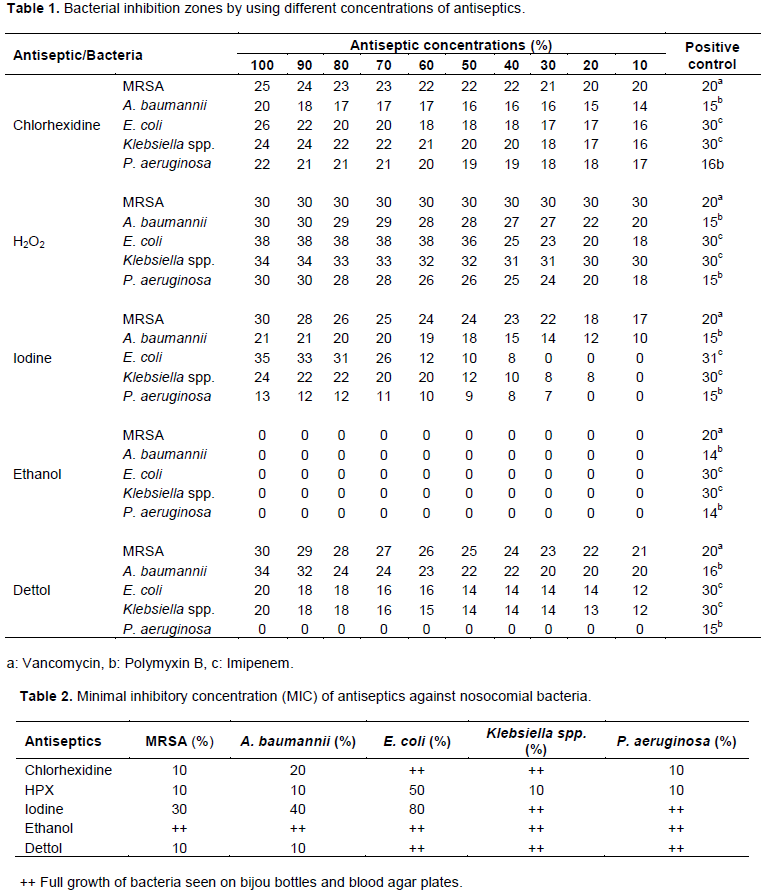
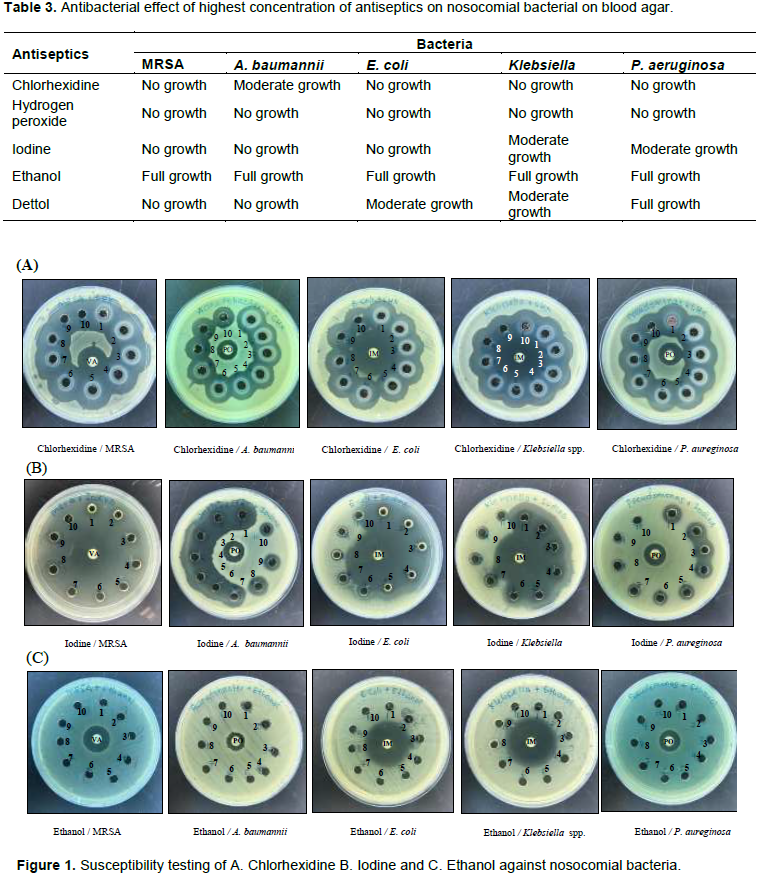
The antibacterial effect of antiseptics on nosocomial bacteria was presented in Table 1 which showed the inhibitory effects of different antiseptics on nosocomial bacteria using different concentrations of antiseptics. Specific antibiotic discs were used as a positive control accordingly. H2O2 showed excellent inhibitory effects on all nosocomial bacteria even with lower concentrations (10%). However, ethanol did not show any inhibitory effects as shown in Figure 1a to c.
The MIC of chlorhexidine against MRSA and P. aeruginosa was 10%, while for A. baumannii was 20% (Table 2). The results showed that Klebsiella spp. was sensitive to H2O2 only with MIC of 10%, while A. baumannii was resistant to ethanol only. MRSA, A. baumannii and E. coli were sensitive to Iodine at various concentrations. E. coli was sensitive to H2O2 with MIC of 50%. Vancomycin disc was used as a positive control and showed inhibition in the growth of MRSA while polymyxin B disc was effective against A. baumannii and P. aeruginosa. Also, Imipenem showed inhibition of E. coli and Klebsiella spp.
Thus, H2O2 clearly shows effectiveness against all nosocomial bacteria since it has the largest zone of inhibition among all the antiseptics (Table 1).
Table 3 shows the inhibitory effects of the highest concentration of different antiseptics used on nosocomial bacteria after 10 min incubation. The results showed that H2O2 had excellent effect and all bacteria showed no growth on blood agar, while chlorhexidine and iodine had excellent effects on E. coli and Klebsiella. The next antiseptic in descending order of their effectiveness was Dettol since both E. coli and Klebsiella were able to survive. However, all studied bacteria showed full growth and not affected by ethanol.
This study showed that antiseptics used in PPP-UiTM still have considerable bactericidal effects on nosocomial bacteria. In 2010, Malaysia was estimated to have hundred thousand cases of nosocomial infection, amounting to 13.9% of the overall hospital admissions (Frost and Sullivan, 2011). This study revealed that different types of nosocomial bacteria vary in their response to different types of antiseptics.
Chlorhexidine is a broad spectrum bactericidal antiseptic that is widely used as in dental, surgical settings and also used in handwashing. Same as previously reported, this study showed excellent inhibitory effects of chlorhexidine against MRSA, A. baumannii and P. aeruginosa even with low concentrations (Ekizoglu et al., 2016; Lanjri et al., 2017); while on E. coli and Klebsiella it was ineffective with lesser inhibitory zones compared to Imipenem as a consequent of the outer membrane which acts as a selective permeability barrier in limiting the entry of many harmful chemical compounds into the bacterial cell (Russell et al., 1998). Chlorhexidine is working on the cytoplasmic membrane and its cationic nature helps in connection with the anionic group (phosphate groups of teichoic acids in Gram-positive bacteria and lipopolysaccharide in Gram negative bacteria) on the bacterial surface with resulting modification of membrane permeability. The effect is mainly due to electrostatic interaction of the chlorhexidine with the acid phospholipids in the cytoplasmic membrane which implies actual absorption onto the cytoplasmic membrane of Gram positive and Gram negative bacteria and leading to a destructive effect. Using chlorhexidine at low concentrations resulted in a bacteriostatic effect while at high concentrations; it can cause membrane disruption and cell death due to coagulation of the cytoplasm (Estrela et al., 2003). Chlorhexidine lasts much longer than other antiseptics; therefore, it is often combined with alcohol in a newer skin preparation composed of 2% chlorhexidine gluconate and 70% isopropyl alcohol (Mangram et al., 1999). It is reported to have a rapid onset of action and has persistent activity to reduce microbial burden on patients’ skin and prevent secondary bacterial infections (Climo et al., 2013). Adaptation and resistance to chlorhexidine has been reported previously among MRSA and many other Gram-negative bacteria including P. aeruginosa and E. coli (Kampf and Kramer, 2004).
Hydrogen peroxide has a broad-spectrum effect against bacteria, bacterial spores, viruses and yeasts (Brudzynski, 2006). This study showed excellent inhibitory effects of H2O2 against both Gram-positive and negative bacteria even with lowest concentration of H2O2 due to a potent oxidant which produce a hydroxyl radicals which in turn will attack cell membrane, lipids, DNA, and other essential cell components (Mai-Prochnow et al., 2008). The results of the present study were in agreement with previous report by Lemmen et al. (2015) who deduced that H2O2 was effective against nosocomial pathogens such as MRSA and multidrug-resistant A. baumannii in hospital settings. Previous study by Kenar et al. (2007) concluded that higher concentrations of H2O2 (10 to 30%) and prolonged interaction are required for sporicidal activity, unfortunately the effect of H2O2 on fungus was not included in this study. Although H2O2 showed inhibitory effect on E. coli after 50% dilution but it is still effective in reducing the expression of all the virulence factors of E. coli by oxidative stress of H2O2 (Hegde et al., 2008). Thus, H2O2 clearly shows effectiveness against all nosocomial bacteria since it has the largest zone of inhibition among all the antiseptics.
The results of this study showed that iodine had comparable effects to chlorhexidine but less than H2O2. These results however were not in agreement with previous finding that chlorhexidine are more effective than iodine in reducing nosocomial infections (Nishimura, 2006). The results reveal variations of the effect of Iodine on different bacteria with different dilutions. The best inhibitory effect of iodine seen against MRSA, A. baumannii and E. coli with dilutions of 30, 40 and 80%, respectively. Hence the more dilution of iodine might weaken the iodine linkage to the carrier polymer with an accompanying increase of free iodine in solution. Therefore, iodine must be diluted according to the supplier’s directions to achieve antimicrobial activity. Based on the aforementioned results, we recommended to use iodine in lower concentrations to avoid skin irritation as previously reported (Murthy and Krishnamurthy, 2009). Due to its rapid, effective and broad-spectrum antimicrobial effects, povidone iodine is likely to remain a highly effective in preventing nosocomial infections in the foreseeable future. A previous clinical trials revealed that iodine was significantly superior to other antiseptic agents such as silver sulfadiazine cream and non-antiseptic dressings, but had lesser effect than rifampicin local cream. Therefore, iodine should be considered among the modern antiseptic agents. In contrast, iodine has many cellular targets, including fatty acids, nucleotides and the free sulfur amino acids cysteine and methionine in proteins 63. This makes the development of resistance unlikely.
Ethanol has a rapid broad-spectrum antimicrobial effect against bacteria, viruses and fungi; however, it is not sporicidal, therefore it is not recommended for sterilization, yet ethanol is used as antiseptics for both hard-surface and skin (McDonnell and Russell, 1999). This study demonstrates that all bacteria were resistant to ethanol at various concentrations. These results were in agreement with recent report by Pidot et al. (2018) who stated that the multidrug-resistant bacterium has become gradually tolerant to the ethanol in widely used hospital disinfectants such as hand rub solutions. Although ethanol performs a multifunctional inhibitory effect on bacterial cells, however the resistant bacteria can overcome the denaturation of proteins, inhibition of DNA, RNA, protein, and peptidoglycan synthesis by ethanol. Researchers have found out that drug-resistant bacteria that commonly cause hospital infections have the chance to develop resistance to ethanol (Cariz, 2018).
Dettol had broad spectrum activity as it inhibited the growth of Gram positive and Gram negative bacteria. Dettol is working through the penetration into the cell and action at the target site through intra-cellular mechanism. Both MRSA and A. baumannii were most susceptible to Dettol at different concentrations even at lowest concentration of 10%. It still showed the highest inhibition zone at 30 and 34 mm for MRSA and A. baumannii, respectively, however P. aeruginosa was resistant even with 100% concentration. Also, both E. coli and Klebsiella were resistant at 100% concentration. Previous studies showed variations for the effects of Dettol on different pathogens due to difference in the species or strains of the organisms or the techniques used (Rutala et al., 2000).
This study has confirmed that H2O2 was the strongest antiseptic against nosocomial bacteria followed by chlorhexidine, whereas ethanol was the weakest one. Determination of antimicrobial efficiency of antiseptics regularly is crucial to reduce NI which also could be reduced by using a proper antiseptic with adequate dilutions.
The authors have not declared any conflict of interests.
This work was supported by Faculty of Medicine, Universiti Teknologi MARA (UiTM) under the program, Research Entity Initiative (REI) Grant [600-IRMI/DANA 5/3/REI (0008/2016)]. The authors would like to thank UiTM Private Specialist Centre for their support, and also all technicians in multi-disciplinary laboratory for their help and support.
REFERENCES
|
Al-Talib HI, Yean CY, Al-Jashamy K, Hasan H (2010). Methicillin-resistant Staphylococcus aureus nosocomial infection trends in Hospital Universiti Sains Malaysia during 2002-2007. Annals of Saudi medicine 30(5):358-363.
Crossref
|
|
|
|
Bigliardi PL, Alsagoff SAL, El-Kafrawi HY, Pyon JK, Wa CTC, Villa MA (2017). Povidone iodine in wound healing: A review of current concepts and practices. International Journal of Surgery 44:260-268.
Crossref
|
|
|
|
|
Bouaziz A, Dib AL, Aimeur R, Lakhdara N, Bererhi N, Boureni A, Bouaziz O, Miguel GE, Elena RM, Elena RE (2016). Evaluation of the bactericidal efficacy of different dilutions of tincture of iodine on three bacterial reference strains. Journal of Chemical and Pharmaceutical Research 8(3):242-245.
|
|
|
|
|
Brudzynski K (2006). Effect of hydrogen peroxide on antibacterial activities of Canadian honeys. Canadian Journal of Microbiology 52(12):1228-1237.
Crossref
|
|
|
|
|
Cariz J (2018). Hospital Superbug Becoming Resistant to Alcohol Disinfectants.
View. Accessed 27/2/2019.
|
|
|
|
|
Cheung HY, Wong MM, Cheung SH, Liang LY, Lam YW, Chiu SK (2012). Differential actions of chlorhexidine on the cell wall of Bacillus subtilis and Escherichia coli. PloS One 7(5):1-12.
Crossref
|
|
|
|
|
Climo MW, Yokoe DS, Warren DK, Perl TM, Bolon M, Herwaldt LA, Weinstein RA,Sepkowitz KA, Jernigan JA, Sanogo K, Wong EW (2013). Effect of daily chlorhexidine bathing on hospital-acquired infection. The New England Journal of Medicine 368(6):533-542.
Crossref
|
|
|
|
|
Ekizoglu M, Sagiroglu M, Kilic E, Hascelik AG (2016). An investigation of the bactericidal activity of chlorhexidine digluconateagainst multidrug-resistant hospital isolates. Turkish Journal of Medical Sciences 46(3):903-909.
Crossref
|
|
|
|
|
El-Mahmood AM, Doughari JH (2009). Bacteriological examination of some diluted disinfectants routinely used in the Specialist Hospital Yola, Nigeria. African Journal of Pharmacy and Pharmacology 3(5):185-190.
|
|
|
|
|
Estrela C, Ribeiro RG, Estrela CR, Pecora JD, Sousa-Neto MD (2003). Antimicrobial effect of 2% sodium hypochlorite and 2% chlorhexidine tested by different methods. Brazilian Dental Journal 14(1):58-62.
Crossref
|
|
|
|
|
European Society of Clinical Microbiology and Infectious Diseases (2003). Determination of minimum inhibitory concentrations (MICs) ofantibacterial agents by broth dilution. Clinical Microbiology and Infection 9(8):1-7.
|
|
|
|
|
Frost, Sullivan (2011). Hospital-acquired Infection Incidence - Trends in Malaysia.
View acceseed 27/2/2019.
|
|
|
|
|
Hegde A, Bhat GK, Mallya S (2008). Effect of exposure to hydrogen peroxide on the virulence of Escherichia coli. Indian Journal of Medical Microbiology 26(1):25-28.
Crossref
|
|
|
|
|
Kampf G, Kramer A (2004). Epidemiologic background of hand hygiene and evaluation of the most important agents for scrubs and rubs. Clinical Microbiology Reviews 17(4):863-893.
Crossref
|
|
|
|
|
Kenar L, Ortatatli M, Yaren H, Karayilanoglu T, Aydogan H (2007). Comparative sporicidal effects of disinfectants after release of a biological agent. Military Medicine 172(6):616-621.
Crossref
|
|
|
|
|
Kouchak F, Askarian M (2012). Nosocomial infections: the definition criteria. Iranian Journal of Medical Sciences 37(2):72-73.
|
|
|
|
|
Lanjri S, Uwingabiye J, Frikh M, Abdellatifi L, Kasouati J, Maleb A, Bait A, Lemnouer A, Elouennass M (2017). In vitro evaluation of the susceptibility of Acinetobacter baumannii isolates to antiseptics and disinfectants: comparison between clinical and environmental isolates. Antimicrobial Resistance and Infection Control 6(36):1-7.
Crossref
|
|
|
|
|
Lemmen S, Scheithauer S, Hafner H, Yezli S, Mohr M, Otter JA (2015). Evaluation of hydrogen peroxide vapor for the inactivation of nosocomial pathogens on porous and nonporous surfaces. American Journal of Infection Control 43(1):82-85.
Crossref
|
|
|
|
|
Mahon CR, Lehman DC, George M (2014). Textbook of Diagnostic Microbiology 5ed: Elsevier.
View
|
|
|
|
|
Mai-Prochnow A, Lucas-Elio P, Egan S, Thomas T, Webb JS, Sanchez-Amat A, Kjelleberget S (2008). Hydrogen peroxide linked to lysine oxidase activity facilitates biofilm differentiation and dispersal in several gram-negative bacteria. Journal of Bacteriology 190(15):5493-5501.
Crossref
|
|
|
|
|
Mangram AJ, Horan TC, Pearson ML, Silver LC, Jarvis WR (1999). Guideline for Prevention of Surgical Site Infection, 1999. Centers for Disease Control and Prevention (CDC) Hospital Infection Control Practices Advisory Committee. American Journal of Infection Control 27(2):97-132.
Crossref
|
|
|
|
|
Matthew EW, Lucy JB, Laura CB, Sutton JM (2017). Mechanisms of increased resistance to chlorhexidine and cross-resistance to colistin following exposure of Klebsiella pneumoniae clinical isolates to chlorhexidine. Antimicrobial Agents and Chemotherapy 61(1):1-12.
|
|
|
|
|
Mbajiuka C, Onuoha S, Ugah U (2015). Comparative studies of the efficacy of some disinfectants on human pathogens. Researcher 7(1):39-45.
|
|
|
|
|
McDonnell G, Russell AD (1999). Antiseptics and disinfectants: activity, action, and resistance. Clinical Microbiology Reviews 12(1):147-179.
Crossref
|
|
|
|
|
McKeen LW (2012). Introduction to Food Irradiation and Medical Sterilization. The effects of sterilization on Plastics and Elastomers. Oxford - United Kindom Elsevier; P 27.
Crossref
|
|
|
|
|
Mullany LC, Darmstadt GL, Tielsch JM (2006). Safety and impact of chlorhexidine antisepsis interventions for improving neonatal health in developing countries. The Pediatric Infectious Disease Journal 25(8):665-675.
Crossref
|
|
|
|
|
Murthy MB, Krishnamurthy B (2009). Severe irritant contact dermatitis induced by povidone iodine solution. Indian Journal of Pharmacology 41(4):199-200.
Crossref
|
|
|
|
|
Nishimura C (2006). Comparison of the antimicrobial efficacy of povidone-iodine, povidone- iodine-ethanol and chlorhexidine gluconate-ethanol surgical scrubs. Dermatol 212 Suppl 1(21-25).
Crossref
|
|
|
|
|
Pidot SJ, Gao W, Buultjens AH, Monk IR, Guerillot R, Carter GP, Lee JYH, Lam MMC, Grayson ML, Ballard SA, Mahony AA, Grabsch EA, Kotsanas D, Korman TM, Coombs GW, Robinson JO, da Silva AG, Seemann T, Howden BP, Johnson PDR, Stinear TP (2018). Increasing tolerance of hospital Enterococcus faecium to handwash alcohols. Science Translational Medicine 10(452):eaar6115.
|
|
|
|
|
Raines K, Rosen K (2016). The effect of chlorhexidine bathing on rates of nosocomial infections among the critically ill population: An analysis of current clinical research and recommendations for practice. Dimensions of Critical Care Nursing35(2):84-91.
Crossref
|
|
|
|
|
Russell AD (1999). Bacterial resistance to disinfectants: present knowledge and future problems. The Journal of Hospital Infection 43(Supplement):S57-S68.
Crossref
|
|
|
|
|
Russell AD, Tattawasart U, Maillard JY, Furr JR (1998). Possible link between bacterial resistance and use of antibiotics and biocides. Antimicrobial Agents and Chemotherapy 42(8):2151.
Crossref
|
|
|
|
|
Rutala WA, Barbee SL, Aguiar NC, Sobsey MD, Weber DJ (2000). Antimicrobial activity of home disinfectants and natural products against potential human pathogens. Infection Control and Hospital Epidemiology 21(1):33-38.
Crossref
|
|
|
|
|
Shahriari S, Mohammadi Z, Mokhtari MM, Yousefi R (2011). Effect of hydrogen peroxide on the antibacterial substantivity of chlorhexidine. International Journal of Dentistry 2010:1-4.
Crossref
|
|
|
|
|
Sridhar PN (2012). Testing of disinfectants.
View
|
|
|
|
|
Tuhina B, Joel F, Shampa A (2013). Comparative analysis of newly introduced disinfectants in hospitals in India: An important aspect of infection control policy. International Journal of Infection Control 9(1):1-5.
|
|
|
|
|
Vernon MO, Hayden MK, Trick WE, Hayes RA, Blom DW, Weinstein RA (2006). Chlorhexidine gluconate to cleanse patients in a medical intensive care unit: the effectiveness of source control to reduce the bioburden of vancomycin-resistant enterococci. Archives of Internal Medicine 166(3):306-312.
Crossref
|
|
|
|
|
Wayne P (2012). Clinical Laboratory Standards Institute. In: Performance standards for antimicrobial susceptibility testing. M100-S22.
|
|
|
|
|
William AR, David JW, the Healthcare Infection Control Practices Advisory Committee (HICPAC) (2008). Guideline for disinfection and sterilization in healthcare facilities Healthcare infection control practices advisory committee.
View acceseed 27/2/2019.
|
|