ABSTRACT
Fungal infection and antifungal drug resistance especially in the treatment of immuno suppressive syndromes, has created an increased demand for reliable and affordable methods of in vitro testing of antifungal agents that can assist in their diagnosis. This study aimed to investigate antifungal susceptibility testing method that is reliable, flexible, affordable, accurate, cheap and less time consuming in order to reduce the prevalence of antifungal drug resistance using the plasma micro broth dilution assay. Results show differences in the performances of the agar dilution, plasma micro-broth dilution assay and disc diffusion test methods of ketoconazole susceptibility testing using Candida albicans with respect to time, cost and reliability. Therefore, development of an in vitro antifungal susceptibility testing method that will allow the clinical laboratory to perform with some confidence is imminent.
Key words: Plasma micro broth, antifungal, Candidas albican, in vitro.
The rising prevalence of serious fungal infection and antifungal drug resistance especially in the treatment of immuno suppressive syndromes has created an increased demand for reliable and affordable methods of in vitro testing of antifungal agents that can assist in their diagnosis. These methods usually performed in the laboratory for susceptibility testing can be grouped into three categories; diffusion, dilution and diffusion-dilution (Alexander et al., 2009). Resistance to antifungal agents has resulted in morbidity and mortality from treatment failures and increased health care costs. Although defining the precise public health risk and estimating the increase in costs, it is not a simple undertaking and there is little doubts that emergent antifungal resistance is a serious global problem.
The phenomenon of switching of some antifungal agents from only prescription to over-the counter (OTC) has provided conducive environment to the misuse of the antifungal agents. The misuse has been implicated in the rise of antifungal resistant strains as the result of selective pressure. Nevertheless, the trends of opportunistic fungal infections have been observed to increase in recent decades from 18% to above 60%, which has resulted in the increase use of antifungal agents (Mushi et al., 2017).
Candida albicans is the commonest cause of candidiasis (moniliasis). The yeast is the common commensal of the gastrointestinal tract. Most Candida infections are opportunistic, occurring in debilitated persons. Candidiasis is also associated with prolonged broad spectrum antibiotic therapy.
Many different clinical forms of candidiasis are known, involving primarily the mucosal surfaces (thrush), gastrointestinal or urogenital tract, and deep-seated infection such as cadidaemia or meningitis (Imran and Alshammry, 2016a).
Diffusion method such as the disc diffusion method first described by Bawer et al. (1966) require little specialized equipment and are easily customizable. Briefly, a test organism suspension is plated on a culture plate; paper discs containing the drug are deposited on the inoculated plate and incubated (Alexander et al., 2009). Plates are subsequently inspected for growth and the zones of growth inhibition surrounding the paper discs are measured.
Dilution methods allow for high sample throughput and quantitative inference regarding the minimal inhibitory concentration (MIC) needed to inhibit growth in vitro, but are associated with higher cost (Jorgensen et al., 1993). Wells containing dilution of the test drug are inoculated with the organism and incubated. The MIC that inhibits fungal growth in vitro is determined. Test drugs are most commonly diluted in twofold dilution series potentially leading to broad ranges of concentration being summarized by one MIC value (Turnidge and Paterson, 2007).
Agar dilution involves the incorporation of varying concentrations of antimicrobial agents into an agar medium usually using serial two-fold dilutions, followed by the application of defined organism inoculums to the agar surface of the plate (Alexander et al., 2009).
The rising prevalence of serious fungal infection and antifungal drug resistance has created an increased demand for reliable and affordable methods of in vitro testing of antifungal agents that can assist in their diagnosis. The techniques employed are often taken for granted.
Early investigators recognized these techniques, which are the disc diffusion, the agar dilution and the micro-broth dilution tests, and observed that there were many variables affecting the result of these tests. Consequently, there was recognition (as early as the late 1990s) that standardization of these techniques was required. This has led to many organizations producing standardized antifungal susceptibility testing methodologies that can help in antifungal susceptibility testing. With all this, there is need for the establishment of antifungal susceptibility testing method that is reliable, flexible, affordable, accurate, cheaper and less time consuming in order to reduce the prevalence of antifungal drug resistance.
An experimental study was carried out on antifungal susceptibility testing using three isolates of C. albicans designated A, B and C; all isolated from cases of vaginal candidiasis from Science for Life Foundation Laboratory, Bemenda, North West region of Cameroon. Disc diffusion, agar dilution and plasma micro-broth dilution tests for antifungal susceptibility assays were employed.
Preparation of C. albicans suspension
Pure cultures of Candida albicans were obtained from the Science for Life Foundation Laboratory. The isolates were inoculated onto Sabouraud dextrose agar (SDA) plates and incubated at room temperature for 48 h after which the colonies on the SDA were further cultured onto SDA slant in a culture tube. It was then sub-cultured onto brain heart infusion agar (BHIA) for 48 h to test for purity. With the aid of a sterile Pasture pipette, the colonies on the surface of the cultures were gently washed with sterile distilled water and vortexed for 15 s, and the cell density was adjusted with a spectrophotometer by adding sufficient sterile saline to increase the transmittance to that produced by a 0.5 McFarland standard at a 530-nm wavelength. The final inoculum suspension was made by a 1:100 dilution followed by a 1:20 dilution of the stock suspension with brain heart infusion broth medium, which resulted in 0.5 × 103 to 2.5 × 103 cells/ml. In each case, the inoculum size was verified by enumeration of CFU obtained by subculture on Sabouraud dextrose agar.
Susceptibility testing
Disc diffusion method
Paper discs of 6 mm in diameter were made from Whatman No. 1 filter paper using a paper perforator. The discs were placed in a Petri dish and sterilized in a hot air oven at a temperature of 160°C for 60 min.
Ketoconazole 200 mg (Teva Pharmaceuticals USA, Inc.) was obtained in tablet form and was dissolved in 10 ml of sterile distilled water in a sterile bottle. Two sets of 25 µg discs of ketoconazole were prepared. One set was dried at a temperature of 25°C while the other was dried at 40°C in an enclosed incubator, to rule out the effect of temperature on disc potency.
Prepared and well dried SDA plates were seeded with the already prepared inoculums of C. albicans and were kept for 15 min at room temperature for complete absorption. The antifungal discs prepared were carefully placed on the seeded plates, incubated at 37°C, and examined for zones of inhibition after 24 and 48 h. Commercial fluconazole disc was set alongside as positive control while a blank Whatman No. 1 filter paper disc without antifungal agent was placed as a negative control.
Agar dilution method
The antifungal agent (ketoconazole 200 mg) was dissolved in 10 ml of sterile distilled water. Various dilutions were made in sterile molten SDA in test tubes to obtain 50, 25, 12.5, and 6.25 µg/ml concentrations, which were kept in a slanting position at room temperature for solidification. The slopes obtained were inoculated with 50 µl of a uniform suspension of the broth culture of C. albicans and all slopes were incubated at 37°C and were checked on 24 and 48 h for growth. Controls were set alongside. For positive control, griseofulvin incorporated into SDA slants at concentration of 500 µg/ml was use, while for negative control, plain SDA slope was used. As such, absence of growth was considered sensitive while growth was considered resistant. After 48 h of incubation, a Gram stain was done to confirm the presence and absence of growth. The MIC was considered as the lowest concentration that gave no growth.
Plasma micro-broth dilution assay
A serial dilution of antifungal agent (ketoconazole 200 mg) was made in sterile micro titer plate using brain heart infusion broth (BHIB) as diluent in wells of different columns in triplicate to obtain concentrations of 50, 25, 12.5, and 6.25 µg/ml. 50 µl of fresh plasma was added into the wells of the first columns, while a drop of 1% phenol red indicator was added into the wells of the first and second columns. In the third column, only BHIB and ketoconazole was added. In the fourth column, only BHIB was added into the wells with no antifungal agent (positive control). All were done in triplicate to minimize error. One drop (50 µl) of the already prepared inoculums of C. albicans (0.25×102/50 to 1.25×102/50 µl) was added into the different wells using a sterile glass pasture pipette. Chloramphenicol was added into the various wells at a concentration of 10 µg to inhibit the growth of bacterial contamination. It was then incubated at 37°C for 24 and 48 h. Growth was examined macroscopically by colour changes and confirmed microscopically by examining Gram stained preparations and also wet mount from the various wells. Pink coloration was an indicator of growth, that is, resistant, while yellowish coloration indicated absence of growth, that is, sensitive.
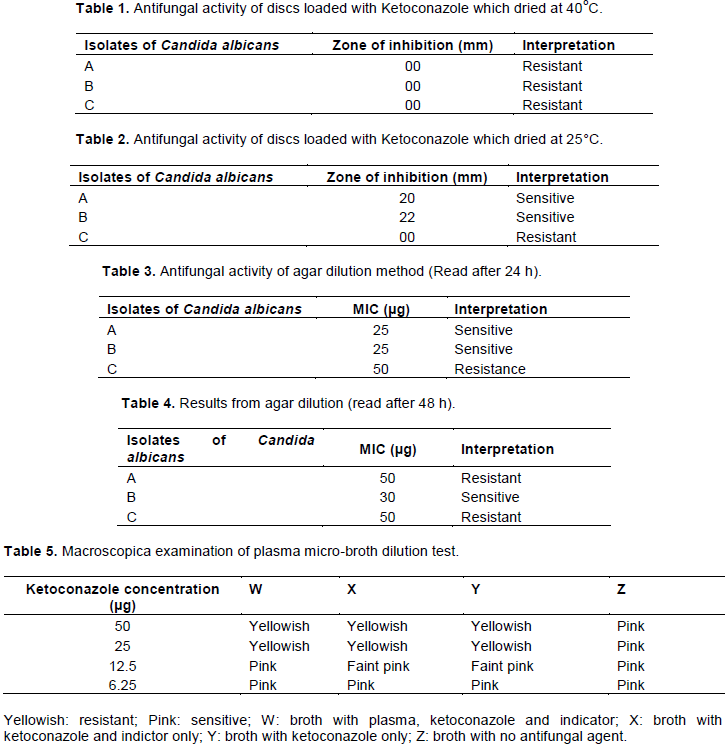
According to the results of disc diffusion obtained, all the isolates were resistant to disc that were prepared and dried at 40°C (Table 1). Two Candidal isolates were sensitive to prepared ketoconazole discs which were dried at 25°C with mean zone diameters of 20 and 22 mm, respectively (Table 2). For the agar dilution method, two of the isolates were inhibited after 24 h of incubation with mean MIC of 25 µg (Table 3), and on further incubation for 48 h, only one isolate was sensitive with an MIC of 30 µg (Table 4).
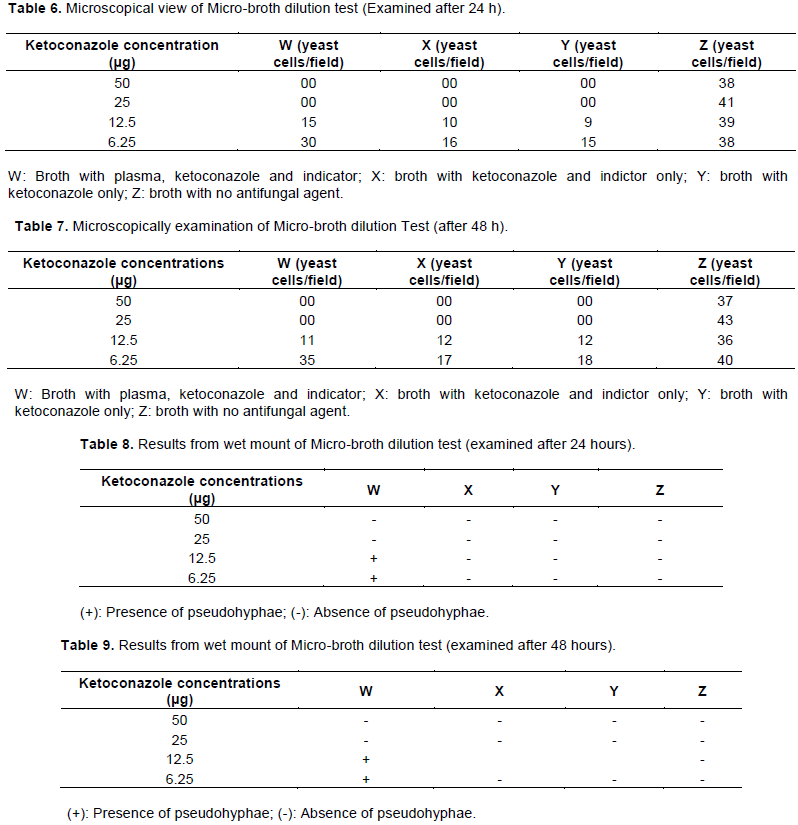
According to antifungal activity using micro-broth dilution assay, macroscopically examination of the micro titer plates read after 24 and 48 h of incubation revealed pink coloration for wells that had growth and yellow coloration for those that did not have growth (Table 5). Results from Gram stained preparations red after 24 h of incubation reveal a MIC of 25 µg. In the column containing the plasma, the first and second dilutions had no yeast cell, while the third and fourth dilutions had 15 and 30 yeast cells/field, respectively. In the column containing broth, indicator and ketoconazole, the first and second dilutions showed no yeast cells/field while the third and the fourth dilutions had 10 and 16 yeast cells/field, respectively. In the column containing only broth and ketoconazole, the first and second dilutions had no yeast cell/field while the third and fourth dilutions had 9 and 15 yeast cells/field, respectively. The column containing no ketoconazole had 38, 41, 39, and 38 yeast cells/field in the first, second, third and fourth dilutions, respectively (Table 6). Microscopically, examination of Gram stained preparations for plasma micro-broth dilution assay examined after 48 h, in case of the column containing the plasma, the first and second dilutions had no yeast cell, while the third and fourth dilutions had 11 and 35 yeast cells/field, respectively. In the column containing broth, indicator and ketoconazole, the first and second dilutions had 0 yeast cell/field while the third and fourth dilutions had 12 and 17 yeast cells/field, respectively. In the column containing only broth and ketoconazole, the first and second dilutions had 0 yeast cell/field while the third and fourth dilutions had 12 and 18 yeast cells/field, respectively. The column containing no ketoconazole had 37, 43, 36 and 40 yeast cells/field in the first, second, third and fourth dilutions, respectively (Table 7).
According to results obtained from examination of wet mount from the different wells, all the wells that had growth from the columns that contain plasma were positive for pseudohyphae, while all those that did not contain plasma had no pseudohyphae (Tables 8 and 9).
The development of a standardized antifungal susceptibility testing method by the NCCLS has been important, and the in vitro results of the MIC have been shown to correlate quite well with clinical outcome (Rex et al., 1997).
The results of this study showed that the agar dilution test detected 2 strains with a MIC of 25 µg/ml, 1 strain resistance with a MIC of 50 µg/ml after 24 h, while the result read after 48 h indicated that all strains were resistant, this correlate with the reference method for agar dilution introduced by the NCCLS (2002).
With the disc diffusion test, the results from the disc prepared and dried at 40°C detected all the yeasts resistant. In addition, the results read at 48 h detected all the yeasts resistant. This results corroborates previous findings (Imran and Al-Karrem, 2016b)
The disc diffusion method gave a zone diameter of 20 and 22 mm for isolates A and B, respectively while isolate C was resistance with a zone diameter of 00 mm when the results were read after 24 h of incubation. When the disc test results read at 48 h were compared with the results obtained by the Cantón et al. (1999) method, it was found that there was correlation in the two methods. In a similar study carried out by Mushi et al. (2017) with 40 Candida isolates, MIC was ≥16 μg/ml for 14 strains and 11 (79%) of these were detected by the disc test when results were read after 48 h.
A study by Cantón et al. (1999) with 143 Candida isolates from blood cultures evaluated the same commercial disc method that was used. In their study, however, the result of the disc test was read after 24 h and not 48 h. They found that all seven resistant strains and four of seven sensitive strains had zone diameters <22 mm. Of the 129 susceptible strains, 19 strains (15%) had zone diameters <22 mm and were classified as resistant by the disc test. Their results differ from those of the other studies in the sense that, the results were read after 24 h and not 48 h, and it is possible that the shorter incubation time used by Cantón et al. (1999) might explain the differences.
In the present experience, the zone diameters are often difficult to read after 24 h due to poor growth, and this is the reason why 48 h of incubation has been used routinely. The disc test methods used in these different studies vary somewhat, it is necessary that the method should be well suited standardized because resistant strains of C. albicans have nearly always been detected.
In a study carried out by Kirkpatrick et al. (1998), most sensitive and resistance strain were also detected. Susceptible strains especially strains for which the MIC was 8 μg/ml was reported as resistant by the disc test. The results obtained by the ketoconazole disc test are quite comparable to the results obtained by the much used oxacillin disc screening test for detection of penicillin-resistant pneumococci (Jette et al., 1999).
The plasma micro-broth dilution test indicated all the 3 strains of C. albicans used in this study sensitive to ketoconazole with a MIC of 25 µg when the results were read after 24 and 48 h of incubation. From the plasma broth dilution assay, the column that contained fresh plasma showed excessive growth indicating that the plasma had a positive impact on the growth of C. albicans.
The present results from the plasma micro broth dilution assay confirmed that, duration of incubation has been a major factor associated with antifungal susceptibility tests; particularly with Candida species. The 48 h yeast incubation time specified in M27-A (NCCLS, 1995), has been a source of controversy ever since it was first chosen (Lozono et al., 1999). Studies on antifungal susceptibility testing, before the NCCLS undertook preparation of a reference method, had already indicated that results read during the exponential phase of yeast growth were consistent and independent of inoculums size, but the principle of exponential-phase and endpoint readings have generally been ignored (Galgiani et al., 1987).
The micro-broth dilution test adopted from the original NCCLS M27-A broth microdilution MIC test is currently employed in many laboratories. Despite the considerable effort that went into defining and standardizing the M27-A test parameters, many authors have indicated that for tests with Candida spp., a 24 h end-point may improve reproducibility and correlate better with responses in vivo than the recommended 48 h reading time (Lozano et al., 1999).
This study is at an exciting stage in the development of an in vitro antifungal susceptibility testing method that will allow the clinical laboratory to perform with some confidence. It was realized that there were many differences in the performances of the agar dilution, plasma micro-broth dilution assay and disc diffusion test method of ketoconazole susceptibility testing using C. albicans with respect to time, cost and reliability. However, the plasma micro-broth dilution assay for antifungal susceptibility testing of C. albicans is the cheapest, most reliable, and less time consuming to be performed in the clinical diagnostic laboratory of less developed countries.
The authors have not declared any conflict of interests.
REFERENCES
|
Alexander KA, Warnick LD, Wiedmann M (2009). Antimicrobial resistant Salmonella in dairy cattle in the United States. Veterinary Research Communications 33(3):191-209.
Crossref
|
|
|
|
Bawer AW, Kirby WMM, Sherris JC, Turck M (1966). Antibiotic susceptibility testing by a standardized single disc method. American Journal of Clinical Pathology 45:493-496.
Crossref
|
|
|
|
|
Cantón E, Pemán J, Carrillo-Mu-oz A, Orero A, Ubeda P, Viudes A, Gobernado M (1999). Fluconazole susceptibilities of bloodstream Candida sp. isolates as determined by National Committee for Clinical Laboratory Standards Method M27-A and two other methods. Journal of Clinical Microbiology 37(7):2197-2200.
|
|
|
|
|
Galgiani JN, Reiser J, Brass C (1987). Comparison of relative susceptibilities of Candida species to three antifungal agents as determined by unstandardized methods. Journal of Antimicrobial Chemotherapy 31(9):1343-1347
Crossref
|
|
|
|
|
Imran ZK, Al-Karrem ZA (2016a). Evaluation natural cloning of azole- resistant genes CDR1, CDR2, MDR and ERG11 between clinical and soil isolates of Candida albicans based on gene expression. International Journal of PharmTech Research 9(11):229-236.
|
|
|
|
|
Imran ZK, Alshammry ZW (2016b). Molecular diagnosis of Candidemia of intensive care unit patients based on sequencing analysis of ITS regions. International Journal of PharmTech Research 9(12):658-668.
|
|
|
|
|
Jetté LP, Sinave C (1999). Use of an oxacillin disc screening test for detection of penicillin and ceftriaxone-resistant pneumococci. Journal of clinical Microbiology 37(4):1178-1181.
|
|
|
|
|
Jorgensen JH (1993). Selection criteria for an antimicrobial susceptibility testing system. Journal of Clinical Microbiology 31(11):2841-2844.
|
|
|
|
|
Kirkpatrick WR, Turner TM, Fothergill AW, McCarthy DI, Redding SW, Rinaldi MG, Patterson TF(1998). Fluconazole disk diffusion susceptibility testing of Candida species. Journal of Clinical Microbiology 36(11):3429-3432
|
|
|
|
|
Lozono F, Szekely A, Johnson EM (1999). Comparison of a new commercial colorimetric micro dilution method with a standard method for in vitro susceptibility testing of Manual of Clinical Microbiology, page 18 7th editions.
|
|
|
|
|
Mushi MF, Masewa B, Jande M, Mirambo MM, Mshana SE (2017). Prevalence and factors associated with over-the-counter use of antifungal agents in Mwanza City, Tanzania. Tanzania Journal of Health Research 19(1).
Crossref
|
|
|
|
|
National Committee for Clinical Laboratory Standards (NCCLS) 1995). Methodsfor Antifungal Disc Diffusion Susceptibility Testing of Yeasts: Approved Standard M44-A. NCCLS, Wayne, PA, USA.
|
|
|
|
|
National Committee for Clinical Laboratory Standards (NCCLS) (2002). Reference Method for Broth Dilution Antifungal Susceptibility Testing of Yeasts- Second Edition: Approved Standard M27-A2. NCCLS, Wayne, PA, USA.
|
|
|
|
|
Rex JH, Pfaller MA, Galgiani JN (1997). Development of interpretive breakpoints for antifungal susceptibility testing: conceptual framework of in vitro-in vivocorrelation data for fluconazole, itraconazole, and Candida infections. Clinical Infectious Disease 24:235-247.
Crossref
|
|
|
|
|
Turnidge J, Paterson DL (2007). Setting and revising antibacterial susceptibility breakpoints. Clinical Microbiology Reviews 20(3):391-408.
Crossref
|
|