ABSTRACT
Urinary Tract Infection (UTI) is one of the commonest infectious disease in pregnancy, and in pregnancy we have very limited number of antibiotics to treat the UTI. This study was conducted on 151 patients who attended the gynecology clinic during the study period. Nineteen UTI proven cases of UTI were studied for prevalence of microorganism and sensitivity pattern against different antibiotics. Among the bacteria isolated, Escherichia coli (73.68%) and Staphylococcus aureus (10.52%) were the most prevalent Gram negative and Gram positive bacteria respectively. To know the resistance pattern of microorganism we used commercially available discs of different antibiotics. Gram negative bacteria showed more resistance as compared to Gram positive one. It is observed that the most effective antibiotic for Gram negative isolates is Ceftriaxone (87.5%), followed by Amoxicillin + Clavulanic acid (81.25%), Amikacin (75%), Cefuroxime (75%), Cefixime (68.75%) and Mezlocillin (62.5%). For the Gram positive bacteria, Ceftriaxone, Amikacin and Amoxicillin + Clavulanic acid were the most effective antimicrobials (100%). Multidrug resistance Gram negative bacteria were also tested for Extended-spectrum Beta Lactamase (ESBL), 35.71% of E. coli isolates were ESBL producer.
Key words: Urinary tract infection, pregnancy, drug resistance, uropathogens, extended spectrum β-lactamase.
Urinary Tract Infections (UTIs) are common and in the clinical practice it is the second most community-acquired infection worldwide (Awaness et al., 2000; Marcus et al., 2005). UTIs affects all age groups, but due to absence of prostatic secretion, short urethra, easy contamination of urinary tract by fecal bacteria and pregnancy, women are
more prone than men (Jido, 2014; Awaness et al., 2000).
UTI is one of the most common type infections during pregnancy and after anemia second most common disease (Santos et al., 2011). Due to the physiological change, plasma volume increases and urine concentration decreases during pregnancy. Around 70% pregnant women may suffer from glucosuria, which leads to the bacterial growth and UTI (Morgan, 2004; Lucas and Cunningharm, 1993). Additionally, 2-13% of pregnancies complaint for asymptomatic bacteriuria and, if not cured, may lead to adverse fetal and maternal consequences including symptomatic UTIs (Bahadi et al., 2010; Amiri et al., 2015). UTIs can cause certain complications, prolonged hospital stays and significant morbidity (Matuszkiewicz-Rowińska et al., 2015; Smaill and Vazquez, 2015).
The ability of uropathogens (that is, Escherichia coli and Klebsiella pneumoniae) to produce large quantity of Extended-spectrum beta lactamase (ESBL), makes UTI challenging to treat (Zorc et al; 2005; Stürenburg and Mack, 2003). In addition, ESBL may cause serious problems, particularly in those patients who have functional structural anomalies of the urinary tract, diabetic patients undergone a kidney transplant and patients with polycystic kidney disease (Zorc et al., 2005).
Usually in clinical practice the treatment for UTIs is given empirically, so earlier data of uropathogens prevalence as well as susceptibility for the particular region or setup is necessary (Haider et al., 2010). Emerging trend of bacterial resistance towards different antimicrobials, is due to the excessive application of antibiotics (Dias Neto et al., 2003; Farrell et al., 2003). Therefore, it is necessary to assess the antimicrobial susceptibility to accomplish the most suitable and effective therapy (Farajnia et al., 2009). Furthermore, for screening of ESBL, the sensitivity also depends upon the antimicrobial agents used for testing. However, in Saudi Arabia only few studies are conducted and reported that prevalence of ESBL varies from 11-36% in different regions (Nicolas-Chanoine et al., 2008). The surveillance of antimicrobial resistance is obligatory to decide the susceptibility pattern of uropathogens for the selection of empirical antibiotics.
Study setting
This prospective cross-sectional study was conducted at Najran University Hospital, Najran region of Saudi Arabia from August 2018 to January 2019.
Study participants
The study was carried out on the patients consulting the Outpatient Department (OPD) and Inpatient Department (IPD) of the hospital.
Inclusion and exclusion criteria
All the pregnant women irrespective to their age, parity and gestational age were included, while women with underlying renal pathology, chronic renal disease, patients who are already on antibiotics for other diseases, mentally retarded, unconscious patients, drug addicts and patients unable to comply were excluded from the study.
Ethical approval
The research was conducted in accordance with the Declaration of Helsinki. The study protocol was reviewed and approved by Najran University Ethical Committee (12-06-16 EC). An informed consent was also signed by the patients for participating in the study.
Isolation and identification of UTI isolates
Patients were instructed to collect the Midstream Sample Urine (MSU) and cultured in the pathological laboratory of Najran University hospital for the isolation of the uropathogens, urine sample was streaked on MacConkey’s agar plates (Saudi Prepared Media Laboratory, Riyadh, Saudi Arabia) and incubated at 37°C for 24 h. Next day or after 24 h individual colonies were selected and identified on the basis of their biochemical and morphological characteristics (Akhtar et al., 2014).
For identification of gram negative bacteria
Motility test, Gram-staining and capsule staining (Anthony’s method) were performed to check the morphological characteristics, to see the growth pattern of bacteria, different medias like Mac-Conkey’s agar no.3, Eosine Methylene Blue agar were used, and for the observation of biochemical characteristics, sugar fermentation (glucose, lactose, maltose, manitol, xylose and sucrose) TSI, IMVIC (indole, MR, VP, citrate) and nitrate test were done (Al Yousef et al., 2016).
For identification of gram positive bacteria
To check the morphological characteristics, gram-staining and capsule staining (Anthony’s method) were performed. To check the growth pattern, different media including MacConkey’s agar no.3, Nutrient agar, Brain Heart infusion agar, Manitol Salt agar and blood agar base (Oxoid) supplemented with 5% sheep blood were used. For biochemical characteristics, sugar fermentation, oxidase, catalase, novabiocin, optochin, bactracin and bile esculin sensitivity test were performed (Akhtar et al., 2014; Al Yousef et al., 2016).
Maintenance of clinical uropathogens
All the stock cultures were preserved in vials by growing the UTI isolates in 3 ml nutrient broth and next day overlapping with 3 ml 40% glycerol. Vials (tightly sealed) were used to freeze the isolates at 2-8°C.
Determination of antibiotic resistance profile
Disc diffusion method is used for screening of antibiotic resistance. For this purpose, with the help of wire loop UTI isolate lawn were made on nutrient agar plate, then the discs of commercially available antibiotics were placed on that culture plate and incubated at 37°C for 24 h. After 24 h the zone of inhibition around the discs were observed (Al Yousef et al., 2016). Various antibiotics of different classes, such as Ampicillin, Amoxicilin, Amoxicilllin + Clavunic acid, Mezlocillin, Cefuroxime, Ceftazidime, Cefixime, Cefipime, Ceftriaxone, Imipenem (cell wall synthesis inhibitors); Tetracycline, Gentamicin, Amikacin, Clindamycin, Erythromycin, Nitrofurantoin, Tobramycin (protein synthesis inhibitors); Trimethoprim, Co-trimoxazole, Ciprofloxacin, Norfloxacin (inhibits bacterial DNA synthesis), were used to assess the susceptibility profile of uropathogens. ESBL production was assessed using the CLSI recommendations for ESBL screening and phenotypic confirmation tests (CLSI USA; 2018).
Statistical analysis
The statistical relation between age and antibiotic sensitivity was analysed by two tailed chi-square test, wherein Pearson Chi-Square value and likelihood ratio were calculated using Statistical Package for Social science (SPSS), Version 16 for windows. Differences were considered significant if p<0.05.
For this observational study, a total of 200 pregnant women were selected for the study. However, only 151 pregnant women were examined based on their symptoms for UTI.
Demographic characteristics of study subjects
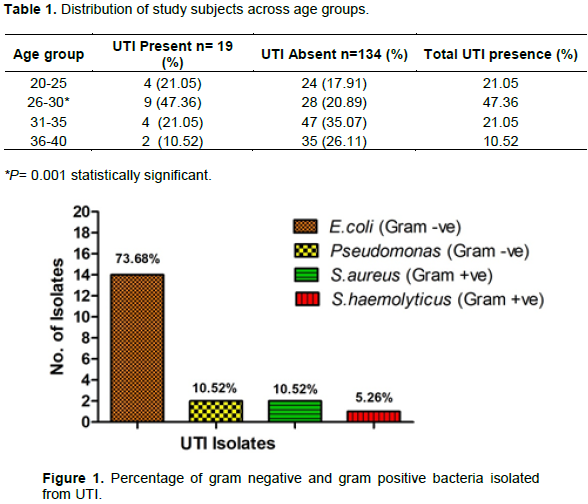
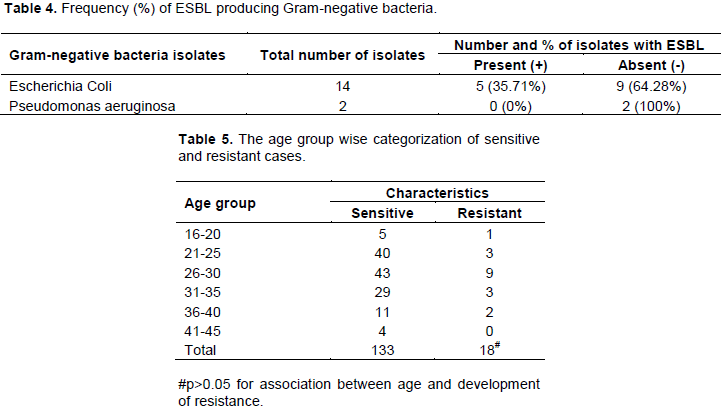
In this study, we observed that mean age of the patients was 28.52 ± 5.96 years. The age group 26-30 years shows highest number (47.36%) positive cases among the pregnant women, there is a statistically significant difference (pË‚ 0.001) when compared to other age groups (Table 1). Further, correlation between the different age group and sensitivity as well as resistance was computed using chi-square test. Chi-square test revealed no significant association between different age groups and antibiotic specificity (Table 5) with a p value > 0.05 and Chi-Square value of 3.590.
Different UTI isolates
Urine culture reports revealed that only 19 patients were found to have a positive culture result (presence of UTI). Amongst positive culture results, 14 patients (73.68%) were found to be positive for E. coli, followed by 2 patients (10.52%) each for Staphylococcus aureus and Pseudomonas, and 1 patient (5.26%) for Staphylococcus haemolyticus (Figure 1).
Antimicrobial susceptibility profile
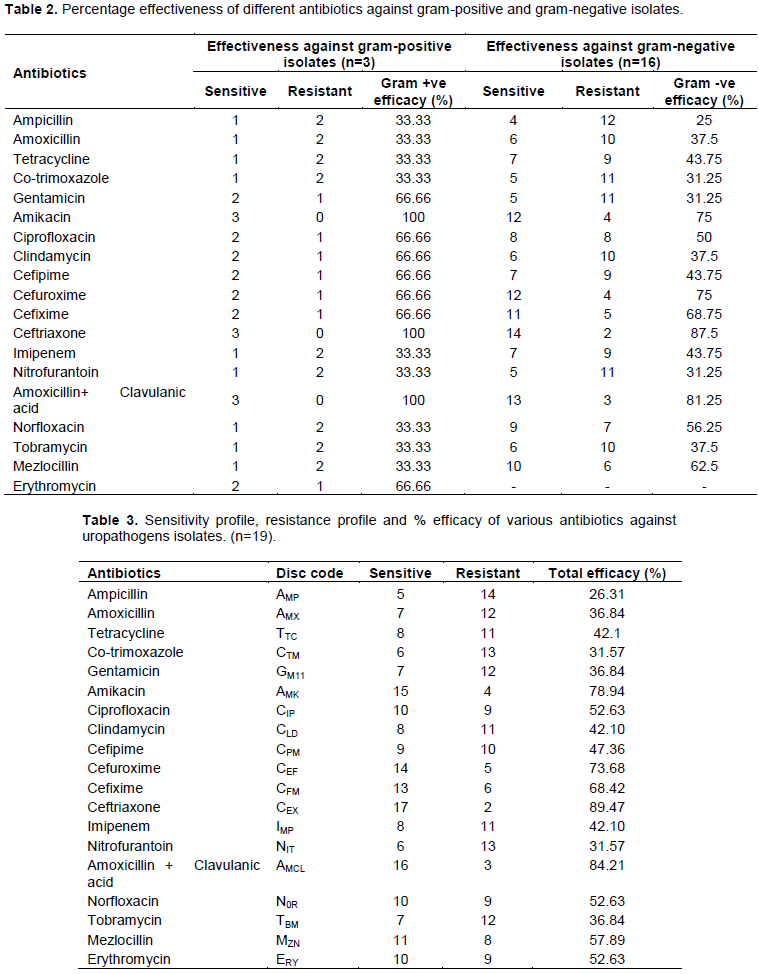
In our study it is observed that most effective antibiotic for Gram negative isolates is Ceftriaxone (87.5%) followed by Amoxicillin + Clavulanic acid (81.25%), Amikacin (75%), Cefuroxime (75%), Cefixime (68.75%) and Mezlocillin (62.5%) and among the gram positive isolates Ceftriaxone, Amikacin and Amoxicillin + Clavulanic acid are most effective (100%) (Table 2). It is also observed that antibiotic efficacy varies from 26.31 to 89.47% (Table 3).
ESBL prevalence
The Gram-negative bacteria showing multidrug resistance were also tested for ESBL, and we observed that only 35.71% of E. coli isolates were ESBL producer. Another Gram negative bacteria like Pseudomonas aeruginosa was not found to be ESBL producer (Table 4).
During pregnancy asymptomatic bacteriuria is a commonest infection, which usually leads to the development of symptomatic UTI and put the mother and fetus on risk (Akhtar et al., 2014; Al-Aali and Yousef, 2015; Haider et al., 2010). We observed that overall prevalence of UTI among the pregnant women is 12.5% which is almost similar to a study conducted in different parts of Saudi Arabia (Al-Sibai et al., 1989).
The age group of 26-30 years indicated highest percentage (47.36%) of UTI infection, as this age group is sexually more active, leading to higher incidence of UTIs. This result is co-related with another study conducted by Al-Aali and Yousef, in Taif region of Saudi Arabia (Al-Aali and Yousef, 2015) and Imade et al, in Benin City, Nigeria (Imade et al., 2010). For the symptomatic bacteriuria during pregnancy, advanced maternal age is one of the important risk factor and women likely to have had many children before current pregnancy and this may be the multifactorial risk factor for acquiring the UTI during pregnancy (Akinloye et al., 2006).
It is also observed that the frequency of Gram negative isolates is more as compare to the Gram positive isolates, and the most predominant microorganism is E. coli (73.68%) followed by Pseudomonas (10.52 %). This result correlates with the other studies conducted in different part of Saudi Arabia and other countries as well (Saeed and Tariq, 2011; Al-Aali and Yousef, 2015). Actually the pattern may be differing from place to place and time to time, but in most of the studies conducted in different regions of the world, it is observed that E. coli is the most common microorganism causing UTI in pregnancy or clinical practice.
For the treatment of UTIs antibiotics are commonly used, though the antibiotic resistance is reported by conducting different studies all over the world, especially in developing countries (Lamikanra and Okeke, 1997; Gaspari et al., 2005). Our results were in accordance to another study conducted in Dessie area, North-East Ethiopia, which reported that E. coli, pseudomonas and proteus species were most common pathogens and the E. coli were almost resistant to Ampicillin, Tetracycline, and Co-trimoxazole (Abejew et al., 2014).
Due to the increasing resistance of antibiotics, treatment of UTI is challenging, especially in pregnancy because we have limited options of antibiotics to treat the disease. In our study, we also determined the antimicrobial sensitivity pattern for all the isolates by disc diffusion method with the help of commercially available disc of different antibiotics. Majority of the isolates (Gram negative and Gram positive) were found to be resistant against most of the antibiotics, while antibiotic efficacy varied from 26.31 to 89.47%, moreover Gram negative isolates showed more resistance than gram positive one. We observed the most effective antibiotic is Ceftriaxone (87.5%) followed by Amoxicillin + Clavulanic acid (81.25%) and Amikacin (75%), the findings were consistent with the study conducted by Saeed and Tariq (2011).
Interestingly, resistance to Ampicillin, Amoxicillin, Co-trimoxazole, Tobramycin, Nitrofurantoin and Erythromycin was found to be more common in our study. It can be correlated between use and frequency of antibiotics and the kind of resistance strain in humans (Akhtar et al., 2014). Over the past few years, ESBL producing strains are continuously increasing among the different clinical isolates and in different part of the world, it varies from 1.5% in Denmark to 69% in India (Hansen et al., 2012; Pathak et al., 2014). In our study we found that only 35.71% of E. coli is ESBL producer which is almost similar to another study conducted in Riyadh and New Delhi (Alqasim et al., 2018; Akhtar et al., 2014). Other studies conducted in 2002 and 2004 observed that the prevalence of ESBL was 5.6 and 10.3% respectively (Kader and Kumar, 2005). The recent reports show that the prevalence of ESBL in UTIs is increasing continuously in Saudi Arabia, leaving very few options for the physicians for effective treatment of UTIs.
Finally, we suggest that for the empirical use of antibiotic in pregnancy or in clinical practice, local study and prevalence should be conducted rather than to follow the universal guidelines, because the prevalence and resistance pattern of microorganism against different antibiotics varies from time to time and place to place.
In conclusion, regional clinical data regarding the prevalence and efficacy of antibiotics should be taken into consideration along with the treatment guidelines. Our findings urge the need for routine screening for susceptibility of uropathogens in different populations, especially with pregnant women with UTIs, as it may have serious consequences on both mother and fetus. Therefore, screening of all antenatal women visiting the gynecology clinics should be made mandatory, and positive cases must be followed up closely after treatment to avoid recurrence. Adopting this strategy will significantly aid the clinicians in the rational use of antibiotic therapy, prevent overuse and/or misuse of antibiotics, and reduce the emergence of bacterial resistance.
The authors have not declared any conflict of interests.
The authors are thankful to the Najran University Hospital, Najran, Saudi Arabia for providing the facilities to conduct this research.
REFERENCES
|
Abejew AA, Denboba AA, Mekonnen AG (2014). Prevalence and antibiotic resistance pattern of urinary tract bacterial infections in Dessie area, North-East Ethiopia. BMC research notes 7(1):687.
Crossref
|
|
|
|
Akhtar SM, Mohsin N, Zahak A, Ruhal AM, Pillai PK, Kapur P, Zaki AM (2014). Antimicrobial sensitivity pattern of bacterial pathogens in urinary tract infections in South Delhi, India. Reviews on recent clinical trials 9(4):271-275.
Crossref
|
|
|
|
|
Akinloye O, Ogbolu DO, Akinloye OM, Terryalli OA (2006). Asymptomatic bacteriuria in pregnancy in Ibadan, Nigeria: a re-assessment. British Journal of Biomedical Science 63(3):109-112.
Crossref
|
|
|
|
|
Al-Aali KY, Yousef W (2015). Prevalence of Asymptomatic Bacteriuria in Pregnant Women, Western Region, Taif, Saudi Arabia. International Journal of Science and Research 4(12):1125-1131.
Crossref
|
|
|
|
|
Al-Dujiaily AA (2000). Urinary tract infection during pregnancy in Tikrit. Medical Journal of Tikrit 6(3):220-224.
|
|
|
|
|
Alqasim A, Abu Jaffal A, Alyousef AA (2018). Prevalence of Multidrug Resistance and Extended-Spectrum β-Lactamase Carriage of Clinical Uropathogenic Escherichia coli Isolates in Riyadh, Saudi Arabia. International Journal of Microbiology 2018:1-9.
Crossref
|
|
|
|
|
Al-Sibai MH, Saha A, Rasheed P (1989). Socio-biological correlates of bacteriuria in Saudi pregnant women. Public health 103(2):113-121.
Crossref
|
|
|
|
|
Al-Yousef SA, Younis S, Farrag E, Moussa HS, Bayoumi FS, Ali AM (2016). Clinical and laboratory profile of urinary tract infections associated with extended spectrum β-lactamase producing Escherichia coli and Klebsiella pneumoniae. Annals of Clinical andLaboratory Science 46(4):393-400.
|
|
|
|
|
Amiri M, Lavasani Z, Norouzirad R, Najibpour R, Mohamadpour M, Nikpoor AR, Raeisi M, Zare Marzouni H (2015). Prevalence of urinary tract infection among pregnant women and its complications in their newborns during the birth in the hospitals of Dezful City, Iran, 2012-2013. Iranian Red Crescent Medical Journal 17(8):e26946.
Crossref
|
|
|
|
|
Awaness AM, Al-Saadi MG, Aadoas SA (2000). Antibiotics resistance in recurrent urinary tract infection. Kufa medical journal 3:159.
|
|
|
|
|
Bahadi A, El Kabbaj D, Elfazazi H, Abbi R, Hafidi MR, Hassani MM, Moussaoui R, Elouennass M, Dehayni M, Oualim Z (2010). Urinary tract infection in pregnancy. Saudi Journal of Kidney Disease and Transplantation 21:342-344.
|
|
|
|
|
Clinical and Laboratory Standards Institute (CLSI) (2018). Performance Standards for Antimicrobial Susceptibility Testing. 28th Information Supplement (M100-S28), Clinical and Laboratory Standards Institute, Wayne, PA, USA.
|
|
|
|
|
Dias Neto JA, Silva LDMD, Martins ACP, Tiraboschi RB, Domingos AL A, Suaid HJ, Cologna AJ (2003). Prevalence and bacterial susceptibility of hospital acquired urinary tract infection. Acta Cirurgica Brasileira 18:36-38.
Crossref
|
|
|
|
|
Farajnia S, Alikhani MY, Ghotaslou R, Naghili B, Nakhlband A (2009). Causative agents and antimicrobial susceptibilities of urinary tract infections in the northwest of Iran. International Journal of Infectious Diseases 13(2):140-144.
Crossref
|
|
|
|
|
Farrell DJ, Morrissey I, De Rubeis D, Robbins M, Felmingham DAUK (2003). A UK multi centre study of the antimicrobial susceptibility of bacterial pathogens causing urinary tract infection. Journal of Infection 46(2):94-100.
Crossref
|
|
|
|
|
Gaspari RJ, Dickson E, Karlowsky J, Doern G (2005). Antibiotic resistance trends in paediatric uropathogens. International journal of antimicrobial agents 26(4):267-71.
Crossref
|
|
|
|
|
Haider G, Zehra N, Munir AA, Haider A (2010). Risk factors of urinary tract infection in pregnancy. The Journal of the Pakistan Medical Association 60(3):213.
|
|
|
|
|
Hansen DS, Schumacher H, Hansen F, Stegger M, Hertz FB, Schønning K, Justesen US, Frimodt-Møller N, DANRES Study Group (2012). Extended-spectrum β-lactamase (ESBL) in Danish clinical isolates of Escherichia coli and Klebsiella pneumoniae: Prevalence, β-lactamase distribution, phylogroups, and co-resistance. Scandinavian Journal of Infectious Diseases 44(3):174-181.
Crossref
|
|
|
|
|
Imade PE, Izekor PE, Eghafona NO, Enabulele OI, Ophori E (2010). Asymptomatic bacteriuria among pregnant women. North American Journal of Medical Sciences 2(6):263.
|
|
|
|
|
Jido TA (2014). Urinary tract infections in pregnancy: evaluation of diagnostic framework. Saudi Journal of Kidney Diseases and Transplantation 25(1):85-90.
Crossref
|
|
|
|
|
Kader AA, Kumar A (2005). Prevalence and antimicrobial susceptibility of extended-spectrum β-lactamase-producing Escherichia coli and Klebsiella pneumoniae in a general hospital. Annals of Saudi medicine 25(3):239.
Crossref
|
|
|
|
|
Lamikanra A, Okeke IN (1997). A study of the effect of the urban/rural divide on the incidence of antibiotic resistance in Escherichia coli. Biomedical Letters 55:91 97.
|
|
|
|
|
Lucas MJ, Cunningham FG (1993). Urinary tract infection in pregnancy. Clinical Obstetrics and Gynecology 36(4):855-68.
Crossref
|
|
|
|
|
Marcus N, Ashkenazi S, Yaari A, Samra Z, Livni G (2005). Non-Escherichia coli versus Escherichia coli community-acquired urinary tract infections in children hospitalized in a tertiary center: relative frequency, risk factors, antimicrobial resistance and outcome. The Pediatric infectious disease journal 24(7):581-585.
Crossref
|
|
|
|
|
Matuszkiewicz-Rowińska J, Małyszko J, Wieliczko M (2015). Urinary tract infections in pregnancy: old and new unresolved diagnostic and therapeutic problems. Archives of medical science 11(1):67.
Crossref
|
|
|
|
|
Morgan KL (2004). Management of UTIs during pregnancy. MCN: The American Journal of Maternal/Child Nursing 29(4):254-258.
Crossref
|
|
|
|
|
Nicolas-Chanoine MH, Blanco J, Leflon-Guibout V, Demarty R, Alonso MP, Caniça MM, Park YJ, Lavigne JP, Pitout J, Johnson JR (2008). Intercontinental emergence of Escherichia coli clone O25: H4-ST131 producing CTX-M-15. Journal of Antimicrobial Chemotherapy 61(2):273-281.
Crossref
|
|
|
|
|
Pathak N, Dodds J, Zamora J, Khan K (2014). Accuracy of urinary human papillomavirus testing for presence of cervical HPV: systematic review and meta-analysis. BMJ 349:g5264.
Crossref
|
|
|
|
|
Saeed S, Tariq P (2011). Symptomatic and Asymptomatic Urinary Tract Infections during pregnancy. International Journal of Microbiological Research 2(2):101-104.
|
|
|
|
|
Santos F, Sheehy O, Perreault S, Ferreira E, Berard A (2011). Exposure to antiâ€infective drugs during pregnancy and the risk of small-for-gestational-age newborns: a case-control study. BJOG 118(11):1374-1382.
Crossref
|
|
|
|
|
Smaill FM, Vazquez JC (2015). Antibiotics for asymptomatic bacteriuria in pregnancy. The Cochrane database of systematic reviews 7(8):CD000490.
Crossref
|
|
|
|
|
Stürenburg E, Mack D (2003). Extended-spectrum β-lactamases: implications for the clinical microbiology laboratory, therapy, and infection control. Journal of infection 47(4):273-95.
Crossref
|
|
|
|
|
Zorc JJ, Kiddoo DA, Shaw KN (2005). Diagnosis and management of pediatric urinary tract infections. Clinical microbiology reviews 18(2):417-422.
Crossref
|
|