Full Length Research Paper

ABSTRACT
The ayurvedic medicinal system is the world’s most primitive medical systems which were originated in India. For the treatment of Sprue syndrome, a very well-known ayurvedic preparation named Kutajarista (KTJ) is used in the south Asian region. This study aimed to detect the impact of chronic administration of KTJ on hematological parameters. The experimental animals were subdivided into two groups. A high dose (50 mL/kg) of body weight was given to the first group for 42 days and the second group which was considered as the control group was treated with normal water for the same period. There was a remarkable reduction [10.37%, p=0.092] in the total numbers of red blood cells (RBC). A prominent decrease [10.75%. p=0.097] is also observed in the hemoglobin content of the blood. There was a noticeable [11.05%, p=0.077] decrease in the hematocrit level of the blood and a very high [64.35%, p=0.19] increase in the number of white blood cell (WBC) count of the male Sprague-Dawley rat. A remarkably high increase was observed in the absolute count of Neutrophils (220.161%, p=0.12), Eosinophils (368.75%, p=0.11), Lymphocytes [11.29%, p=0.06], and Monocyte [142.781%, p=0.13] count. Also a prominent [↑ 14.15%, p=0.42] increase in the number of platelet counts was observed. Rat cutaneous tail bleeding time and whole blood clotting time shortening were also observed and the result is statistically prominent. As the result shows a significant change in different hematological parameter it can be summarized that KTJ have potential hemotoxicity at a higher dose. Further study is required at a lower dose.
Key words: Ayurvedic, Kutajarista, hemotoxicity, red blood cells (RBC), white blood cells (WBC).
INTRODUCTION
Ayurvedic system of medicine is the world’s most ancient medical system that originated in India about 3000 years ago. Most of the primitive traditional methods of healing such as Tibetan, Chinese and Greek medicine were influenced by the ayurvedic medicine system. In the Indian sub-continent, nearly 80% of the population is currently using ayurvedic preparations and medicinal plants to meet their primary level of disease recovery. At the very beginning of the twentieth-century world health organization recommended larger-scale use of ayurvedic medicine in developing countries as an alternative medicinal system and the use of ayurvedic and herbal origin extracts is increasing day by day (Mohammed et al., 2020; Pehlivan and Sevindik, 2018; Sevindik et al., 2017; “WHO, 2002).
The Sprue syndrome is known in Ayurveda as Grahani is characterized by anemia, weight loss, diarrhea, frothy stools, sore mouth, and indigestion. Besides, mucus appears in the patient's stool. In the morning after rising from bed, the patients significantly discharge a large amount of stool (Bennett et al., 2014; Ramakrishna et al., 2006). Kutajarista (KTJ) is prepared as liquid ayurvedic medicinal form, and currently used at the dose of 12 to 24 mL once or twice daily for the treatment of sprue syndrome, mal-absorption syndrome, ulcerative colitis, diarrhea, irritable bowel syndrome, dysentery or blood dysentery fever, Croon’s disease, etc. ( Verma, 1991; Dash, 1984; Dastur, 1960; Nadkarni, 1976; Mishra, 2010). It acts as an anti-motility and anti-secretory agent thus helps in the treatment of diarrhea (Shamkuwar and Shahi, n.d.). 5 to 10% self-generated alcohol present in the liquid KTJ preparation provides a media to deliver various herbal active components to the body after ingestion (Government of India, 1990).
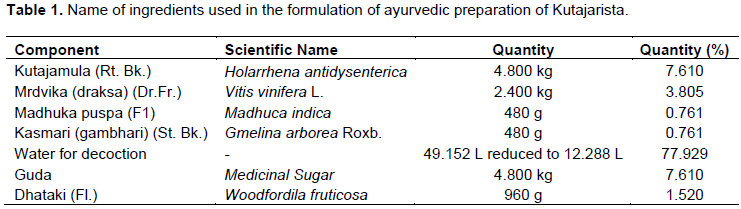
Bangladesh National Formulary of Ayurvedic Medicine included KTJ as herbal medicine in 1992 (Bangladesh National Formulary of Ayurvedic Medicine, 1992) approved by the Government of Bangladesh vide Ministry of Health and Family Welfare Memo No. Health-1/Unani-2/89/ (Part-1) 116 dated 3-6-1991, 2011. The formulation of KTJ is given in Table 1 (Anonymous, 2003; Classical Ayurvedic Prescriptions for Common Diseases (Only for registered ayurvedic medical practitioners), 2010). Directorate of Drug Administration has issued Notification DA/Admin/1-10/96/6212 dated 19th October 1996 has issued a license under Drug Act, 1940.
Ayurvedic medicines have a good safety profile (Ernst, 2002). But recent studies have reported that heavy metal in the ayurvedic preparation (e.g. Lead, Arsenic) shows toxicity (Keen et al., 1994; Olujohungbe et al., 1994). The safety profile of most of the ayurvedic medicine is not yet completely investigated. Considering this issue, this research work has been launched to detect the level of hemotoxicity after chronic administration of the marketed ayurvedic medicinal preparation, KTJ.
MATERIALS AND METHODS
Drugs, chemicals, and reagents
For this hemotoxicological study, KTJ was collected from Sri Kundeswari Aushadhalaya Limited, Chittagong. Ketamine injection was purchased from ACI Limited, Bangladesh. All other reagents and chemicals used in this work were purchased from Human GmbH, Wiesbaden, Germany.
Experimental animals
For acute toxicological study female Swiss Albino mice with body weight in the range of 35 to 40 g were used and the hemotoxicological experiment use 45 to 60 day old male Sprague-Dawley rats that were bred and maintained at the animal house of the Department of Pharmacy, Jahangirnagar University. These animals were weighed in the range of 150 to 170 g and were healthy. Plastic cages having dimensions of 30 × 20 × 13 cm and softwood shavings as the bed were used for housing of all animals. They were fed with rat chow prepared according to the formula developed at Bangladesh Council of Scientific and Industrial Research (BCSIR) and water was provided ad libitum. The rats were maintained at scheduled 12 h a day and 12 h night cycle. Ethical guide for the care and use of laboratory animals approved by the Ethical Review Committee, Faculty of Life Sciences, Department of Pharmacy, Jahangirnagar University was fully followed throughout the experiment on animals.
Design of the study
Acute toxicity study
Guidelines of the Organization for Economic Co-operation and Development (OECD) were followed to detect the acute oral toxicity level (Oecd/Ocde, 2008). Non-pregnant twenty four female mice with body weight in the range of 35 to 40 g were subdivided into six groups (n=4). Different doses of experimental drug Kutajarista (KTJ) (50, 60, 70, 80, 90 and 100 mL/kg of body weight) were administered by intra-gastric syringe. The dose was divided into two equal fractions and administered within 12 h. The observation was done for mortality and clinical signs of toxicity (general behavior, respiratory pattern, cardiovascular signs, motor activities, reflexes and changes in skin and fur texture) for all experimental animals at 1, 2, 3 and 4 h and thereafter once a day for the next three days following KTJ administration.
Chronic toxicity studies
The experiment of detection of chronic hemotoxicity level on rats was started with randomly divided sixteen rats into 2 groups (n=8). One group was treated with KTJ in the dose of 50 mL/kg of body weight for 42 days and another was used as a control and was administered with distilled water only as per the same volume as the drug-treated group for the same period (Gad, 1988). After acclimatization, ayurvedic medicinal preparation KTJ was administered to the rats by an intra-gastric syringe between the 10 and 12 am daily throughout the 42 days long study period. To identify a particular animal all the experimental animals were marked carefully on the tail. By using the identification mark, responses were noted separately for a particular period before and after the administration (Stevens and Gallo, 1989).
Blood samples collection
After completion of 42 days of long treatment with KTJ, the food supply stopped for 18 h. Then 24 h after the last drug administration, Ketamine (500 mg/kg i.p.) was injected to anesthetize the animals. Whole blood samples were collected from post vena cava and transferred to EDTA-added tubes immediately and marked properly. All analyses of blood were completed within 12 h of sample collection (Wolford et al., 1986).
Determination of hematologic parameter
Hematologic profile studies involved analysis of blood parameters such as Red Blood Cells (RBCs) and WIC (WBC Impedance Count) level determined by Electrical Impedance method, Hemoglobin (HGB) level determined by Modified hemiglobincyanide method, Platelet level was determined by Electrical Impedance method, WOC (WBC Optical Count) level was determined by Laser light scatter (Tatsumi et al., 1999; van Kampen and Zijlstra, 1961). Differential analysis was done by the CELL-DYN 3700 System. Erythrocyte Sedimentation Rate is determined by Wintergreen Method (Brigden, 1999). The modified procedure of Mohamed et al. (1969) was used for the determination of bleeding time (Dejana et al., 1979). Clotting time was determined with the method of Goldstein and Abramson (1996). MCV, MCH, and MCHC, HCT, and PCT are calculated according to the formula given by Diem and Konrad (1975) and Ketley (1993).

The platelet distribution width (PDW) is a measure of the heterogeneity of the platelet population. Red cell distribution width (RDW) is a measurement factor for the detection of the level of the heterogeneity of the RBC population.
Statistical analysis
The group data are expressed as Mean ± Standard Error of the Mean (SEM). Unpaired "t" tests were done for statistical significance tests. Statistical Package for Social Science (SPSS) for WINDOWS (Ver. 22) was applied for the analysis of data. Differences between groups were considered significant at p < 0.05, 0.01, and 0.001.
RESULTS
Acute toxicity study
No mortality was observed at the highest administered dose of 100 mL/kg of body weight. Thus the LD50 value was found to be greater than the highest administered dose in the current study. No convulsion, respiratory distress, general irritation, and restlessness were noticed. Since KTJ is used for many years in ayurvedic medicinal system for the clinical purpose of treatment of diarrhea, dysentery, irritable bowel syndrome, or sprue syndrome, a limit test was performed in acute oral toxicity study. OECD test guideline 425 suggests that when there is information in support of low or non-toxicity and immortality nature of the test material, then the limit test at the highest starting dose level 100 mL/kg body weight was launched. Therefore, it can be summarized that KTJ when administered at a high dose is non-toxic oral formulations.
Chronic hematologic profile study
Effect on different blood cell count
Comparing with the control group a statistically noticeable decrease [10.37%; p=0.092] in the total number of red blood cell count of the male rat was observed after 42 days administration of KTJ. Again a very high increase [64.35%; p=0.19] observed in white blood cell (WBC) count that is statistically prominent. The absolute count of different WBC such as Neutrophil, Eosinophil, Lymphocyte, and Monocyte counts was also increased grossly. The platelet count of the male rat also showed a high [14.15%; p=0.42] increase. Different blood cell count data is presented in Table 2.

Effect KTJ on differential (WBC) count in male rats
Blood cell count result obtained by Electrical Impedance method on blood sample of 42 days KTJ administered rat shows an insignificant but noticeable [94.80%; p=0.067] increase in the percentage of Neutrophil count and an increase in the percentage of Eosinophil count [185.214%; p=0.034] and the result not significant. Lymphocyte count decreased significantly [32.28%; p=0.027] and Monocyte count increased [47.721%; p=0.021]. All the results are presented in Table 3.

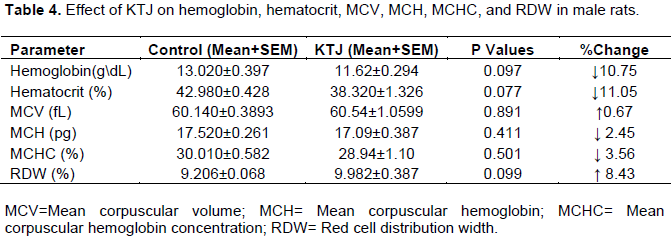
Effect of KTJ on hemoglobin, hematocrit, MCV, MCH, MCHC, and RDW in male rats
After 42 days long administration of KTJ at a dose of 50 ml/kg on male rat the blood sample analysis reports recommend that the hemoglobin content of the blood decrease [10.75%; p=0.097] which is statistically not significant but prominent and hematocrit level of the blood decrease [11.05%; p=0.077] which is statistically noticeable. Different red cell index showed a statistically insignificant change as mean corpuscular volume (MCV) increase [0.67%; p=0.891], mean corpuscular hemoglobin (MCH) decrease [2.45%; p=0.411], mean corpuscular hemoglobin concentration (MCHC) also decrease [3.56%; p=0.501], Red cell volume distribution width (RDW) increase [8.43%; p=0.099]. All the results are presented in Table 4.
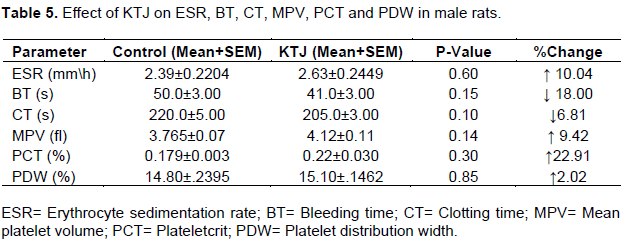
Effect of KTJ on ESR, BT, CT, MPV, PCT and PDW in male rats
Some other blood parameter tests like erythrocyte sedimentation rate, bleeding time, clotting time, mean platelet volume, platecrit value, and platelet volume distribution width were done and result of the drug administered group compared with the control group rat to detect any potential change the level of different blood constituents. The test report suggests a statistically insignificant [10.04%; p=0.60] increase in erythrocyte sedimentation rate and a statistically prominent [18%; p=0.15] shortening of male Sprague-Dawley rat’s cutaneous tail bleeding time. A little [6.81%; p=0.10] shortening of whole blood clotting time in male rats was noticed, the decrease though not significant was prominent. Statistically prominent result was observed in different platelet parameter as in the Mean Platelet Volume (MPV) increase [9.42%; p=0.14], Platecrit value (PCT) increase [22.91%; p=0.30]. A very negligible [2.02%; p=0.85] decrease in the platelet volume distribution width of the male rat was noticed which was statistically not significant. All the results are presented in Table 5.
DISCUSSION
To investigate the level of hemotoxicity of an administered drug or preparation it is essential to assess the hematological profile of an animal. The evolution of risk is done by the analysis of hematological parameters as any abnormal toxicity sign in humans can be well predicted, when tests involve rodents (Olson et al., 2000).
Reviewing the overall study we found a noticeable change in the hematologic parameters that include the possibility of occurrence of an anemic condition, hypersensitivity, allergic symptoms, and leukemia.
Bone marrow parenchyma cell is responsible for the generation of new red blood cells which is also known as erythrocytes (Khan et al., 2013). The principal function of RBC is to carry and protect hemoglobin (Hb) which is responsible for oxygen transport to body tissue. The level of Hb concentration in the blood determines the level of tissue oxygenation. The number of red blood cells or hemoglobin concentration per unit of blood dropped below the normal range, then the condition is termed as anemia. In anemic body condition, cells get less oxygen than their demand (Longo et al., 2015). At any point in the life cycle of RBC (production, recycling, or regulating) anemia may occur in the body. The previous study suggests that six to eight-week-long intake of some ayurvedic preparation reduce the level of RBC and hemoglobin level in the blood of human and animal (Gunturu et al., 2011; Nipa et al., 2016; Rahman et al., 2020). In the current study, the drug KTJ noticeably reduces the RBC count in the blood of Sprague-Dawley rats and that is why we can recommend that the drug has the potential to cause anemia when used for a longer time.
WBC serves in the body's defense mechanism by detecting and destroying the disease-causing agents that enter into the body. Five different types of cell lines (neutrophils, eosinophils, basophils, lymphocytes, and monocytes) comprises the WBC population with all having individual function in the body defense system. A high increase in WBC count is considered as a nonspecific marker of inflammation which is linked with the immune system and correlate both acute and chronic infection and exposure to irritating or toxic agents (O’Byrne and Dalgleish, 2001; Pai et al., 2004; Rader, 2000; Ridker et al., 2000; Ross, 1999). In the current study, we noticed a significant and high increase in the WBC count after chronic administration of KTJ that is matched with the previous study (Nipa et al., 2016; Rahman et al., 2020; Suresh Gupta et al., 2006). A very high increase was also noticed in the differential count of different WBCs. A very high increase in the white blood cell count is the sign of hypersensitivity, inflammation, and leukemia or cardiovascular problem (Majd et al., 2014).
Platelets are not nucleate and are the smallest formed element in the blood (~1-4 µm, ~3-15 fl) with a life cycle of only 4 to 10 days. These are derived from the myeloid stem cell. In most species, counts range between 200,000 and 500,000 µL-1 (rats~800,000 µL-1; mice, >1,000,000 µL-1) (Corey et al., 2014). The primary function of platelets is to maintain homeostasis. More specifically, they can form a plug at the sites of endothelial cell lining injury. Previous studies suggest that a change in the platelet count correlates various infections, inflammation, and myeloproliferative disorders (Sankar, 2017). The current study shows a prominent increase in platelet count that may indicate the presence of infections, inflammation after chronic administration of KTJ.
The main component of the red blood cell is hemoglobin which comprises approximately 33% of a total red blood cell. It is responsible for oxygen transport to tissue which is one of the main functions of blood. The concentration hemoglobin in the whole blood normally is about one-third of the hematocrit. Hemoglobin concentration test in the blood is done as it is a common indicator of iron deficiency. The hematocrit is measured as a percentage and helps to measure the ratio of blood volume occupied by RBCs (Tripathi et al., 2014). Both hemoglobin and hematocrit are considered as a late marker of iron deficiency anemia though it is non-specific (Wu et al., 2002). A correlation observed in the concentration of hemoglobin and hematocrit value, which is the lower value of hematocrit indicates a low number of circulating RBC which ultimately implies decreased oxygen-carrying ability by hemoglobin and produce symptoms of anemia.
A high hematocrit value may reflect an absolute increase in the number of RBCs or a decrease in plasma volume (Lokwani, 2013). In the current study, after chronic administration of the drug Kutajarista prominently decreases hemoglobin concentration and hematocrit level which is a clear indication of hemotoxicity.
Some morphological parameters as mean corpuscular volume (MCV), mean corpuscular hemoglobin (MCH) and mean corpuscular hemoglobin concentration (MCHC) are calculated to identify the types of anemia (Beutler, 1981). Decrease the value of MCV indicates the presence of iron-deficiency anemia (Lokwani, 2013). MCH values are reduced in anemia patients, and the MCHC value is reduced in severe disease. The RDW is a marker of the variation in cell volume within the red cell population. Different sizes and shapes of the red cell can be identified by the RDW test and a high value of RDW rule out liver disease, hemolytic anemia, vitamin B12 deficiency, and folic acid deficiency. In the current study, we observed a very slight change in the MCV, MCH, MCHC, and RDW values.
Any kind of inflammation can be screened non-specifically by the erythrocyte sedimentation rate test. The increased presence of plasma fibrinogen, immunoglobulins, and other acute-phase reaction proteins causes the red blood cell to settle more rapidly under the disease state (Saha et al., 2018). Time taken for platelet plug formation and blood vessel constriction to occur is bleeding time. The clotting time will be prolonged if plasma factors such as prothrombin or fibrinogen are reduced. This study shows an increased erythrocyte sedimentation rate (ESR) value which indicates the presence of any type of inflammation. Bleeding time and clotting time decreased noticeably.
The size of the platelet of a given sample can be measured by mean platelet volume (MPV). An increase in MPV value implies the presence of larger sized platelet which clinically diagnosed as thrombocytopenia (Liu et al., 2012). Plateletcrit (PCT) value reflects the number and size of the platelets and also platelet distribution width (PDW) reflects the variation of platelet size. These markers identify the degree of anisocytosis or heterogeneity of platelet size (Chandrashekar, 2013). This study shows a significant change in the MPV and PCT values but a very negligible change in PWD.
CONCLUSION
From the experiment, it can be concluded that Kutajarista (KTJ) should not be administered chronically at a higher dose as it noticeably reduces red blood cell (RBC) count, hemoglobin, hematocrit, MCH, MCHC and a very high increase in numbers of white blood cell count and platelet count. Further studies should be done by reducing the administered dose. Thus KTJ is to be taken safely only at a dosage of 12 to 24 mL once or twice a day normally advised after food. If needed, it can be mixed with an equal quantity of water.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors are thankful to Focused Research on Ayurvedic Medicine and Education (F.R.A.M.E) Laboratory, Department of Pharmacy, and all faculty members and the technical staff of the Department of Pharmacy, Jahangirnagar University and Noakhali Science and Technology University for their kind co-operation. They thank Mr. Shafiqul Islam for ensuring a constant supply of animals followed by proper maintenance and care of these animals throughout the experimental period.
REFERENCES
|
Anonymous (2003). The Ayurvedic Formulary of India. |
|
|
Dash B (1984). Diagnosis and Treatment of diseases in Ayurveda (Based on Ayurveda Saukhyam of Todarananda). Concept Publishing Company. |
|
|
Bangladesh National Formulary of Ayurvedic Medicine (1992). (Approved by the Government of Bangladesh vide Ministry of Health and Family Welfare Memo No. Health-1/Unani-2/89/ (Part-1) 116 dated 3-6-1991) (2nd ed.). (2011). National Unani and Ayurvedic Formulary Committee Bangladesh Board of Unani and Ayurvedic Systems of Medicine. |
|
|
Bennett JE, Dolin R, Blaser MJ (2014). Mandell, Douglas, and Bennett's Principles and Practice of Infectious Diseases, Ninth edition. |
|
|
Beutler E (1981). Hematology. The Journal of the American Medical Association 245(21):2193-2194. |
|
|
Brigden ML (1999). Clinical utility of the erythrocyte sedimentation rate. American Family Physician 60(5):1443-50 |
|
|
Chandrashekar V (2013). Plateletcrit as a Screening Tool for Detection of Platelet Quantitative Disorders. Journal of Hematology 2(1):22-26. |
|
|
Classical Ayurvedic Prescriptions for Common Diseases (Only for registered ayurvedic medical practitioners) (2010). Central Council for Research in Ayurveda and Siddha. Department of AYUSH, Ministry of Health & Family Welfare Government of India. |
|
|
Corey SJ, Kimmel M, Leonard JN (2014). Systems hematology: An introduction. Advances in Experimental Medicine and Biology 844:3-10. |
|
|
Longo D, Fauci A, Kasper D, Jameson SHJ, Loscalzo J (2015). Harrison's Principles of Internal Medicine: Volumes 1 and 2, 19th Edition. In Mc Graw-Hill. |
|
|
Dastur JF (1960). Everybody's guide to Ayurvedic medicine - A repertory of therapeutic prescriptions based on the indigenous system of India. Taraporevala Sons and Co. |
|
|
Dejana E, Callioni A, Quintana A, de-Gaetano G (1979). Bleeding time in laboratory animals. II - A comparison of different assay conditions in rats. Thrombosis Research 15(1-2):191-197 |
|
|
Diem CL, Konrad (1975). Scientific Tables (7th ed.). Macclesfield: Geigy Pharmaceuticals. |
|
|
Ernst E (2002). Ayurvedic medicines. Pharmacoepidemiology and Drug Safety 11(6):455-456. |
|
|
Goldstein KH, Abramson N (1996). Efficient diagnosis of thrombocytopenia. American Family Physician 53(3):915-920. |
|
|
Government of India (1990). The Ayurvedic Pharmacopoeia of India, Part- I. In Ministry of Health and Family Welfare Department of Ayush. |
|
|
Gunturu KS, Nagarajan P, McPhedran P, Goodman TR, Hodsdon ME, Strout MP (2011). Ayurvedic herbal medicine and lead poisoning. Journal of Hematology and Oncology 4(51). |
|
|
Verma HK (1991). Comprehensive Book of Ayurvedic Medicine for General Practitioners with Annonated Key References Vol I (Based on Modern Diagnosis and Ayurvedic Treatment) (1st ed.). Kalyani Publishers. |
|
|
Nadkarni AK (1976). Indian Materia Medica (Vol. 1). Popular Book Depot. |
|
|
Keen RW, Deacon AC, Delves HT, Moreton JA, Frost PG (1994). Indian herbal remedies for diabetes as a cause of lead poisoning. Postgraduate Medical Journal 70(820):113-114. |
|
|
Ketley N (1993). Wintrobe's Clinical Hematology. Journal of Clinical Pathology. |
|
|
Khan Z, Nawaz M, Khan A, Bacha U (2013). Hemoglobin, red blood cell count, hematocrit and derived parameters for diagnosing anemia in elderly males. Proceedings of the Pakistan Academy of Sciences 50(3):217-226. |
|
|
Liu S, Ren J, Han G, Wang G, Gu G, Xia Q, Li J (2012). Mean platelet volume: A controversial marker of disease activity in Crohn's disease. European Journal of Medical Research 17(1):27. |
|
|
Lokwani D (2013). The ABC of CBC: Interpretation of Complete Blood Count and Histograms. |
|
|
Majd N, Sumita K, Yoshino H, Chen D, Terakawa J, Daikoku T, Kofuji S, Curry R, Wise-Draper TM, Warnick RE, Guarnaschelli J, Sasaki AT (2014). A Review of the Potential Utility of Mycophenolate Mofetil as a Cancer Therapeutic. Journal of Cancer Research 2014(ID 423401):12. |
|
|
Mishra CL (2010). Scientific Basis for Ayurvedic Therapies. (Reprint, x). CRC Press. |
|
|
Mohammed FS, Åžabik AE, Sevindik E, Pehlivan M, Sevindik M (2020). Determination of Antioxidant and Oxidant Potentials of Thymbra spicata Collected from Duhok-Iraq. Turkish Journal of Agriculture - Food Science and Technology 8(5):1171-1173. |
|
|
Nipa JA, Amin MT, Rahman MA, Sharmin F, Karmakar P, Choudhuri MSK (2016). Investigation of hematologic parameter of an Ayurvedic preparation "Amalaki Rasayan" used in jaundice after chronic administration to sprague-dawley rats. Journal of Biomedical and Therapeutic Sciences 3(1):1-6. |
|
|
O'Byrne KJ, Dalgleish AG (2001). Chronic immune activation and inflammation as the cause of malignancy. In British Journal of Cancer 85(4):473-483. |
|
|
Oecd/Ocde (2008). Acute Oral Toxicity - Up-and-Down-Procedure (UDP). Oecd Guidelines for the Testing of Chemicals 425(October):1-27. |
|
|
Olson H, Betton G, Robinson D, Thomas K, Monro A, Kolaja G, Lilly P, Sanders J, Sipes G, Bracken W, Dorato M, Van-Deun K, Smith P, Berger B, Heller A (2000). Concordance of the toxicity of pharmaceuticals in humans and in animals. Regulatory Toxicology and Pharmacology 32(1):56-67. |
|
|
Olujohungbe A, Fields PA, Sandford AF, Hoffbrand AV (1994). Heavy metal intoxication from homeopathic and herbal remedies. Postgraduate Medical Journal 70(828):764. |
|
|
Pai JK, Pischon T, Ma J, Manson JAE, Hankinson SE, Joshipura K, Curhan GC, Rifai N, Cannuscio CC, Stampfer MJ, Rimm EB (2004). Inflammatory markers and the risk of coronary heart disease in men and women. New England Journal of Medicine 351:2599-610. |
|
|
Pehlivan M, Sevindik M (2018). Antioxidant and Antimicrobial Activities of Salvia multicaulis. Turkish Journal of Agriculture - Food Science and Technology 6(5):628. |
|
|
Rader DJ (2000). Inflammatory markers of coronary risk. New England Journal of Medicine 343:1179-1182. |
|
|
Rahman A, Amin MT, Aziz A, Fatema K, Karmakar P, Sen N, Choudhuri MSK (2020). Exploration of the Hematological Profile of Male Sprague-Dawley Rats after Chronic Administration of an Ayurvedic Formulation Punarnavasava (PRV) Used in Ascites Treatment. Journal of Traditional Medicine and Clinical Naturopathy 9(2):287. |
|
|
Ramakrishna BS, Venkataraman S, Mukhopadhya A (2006). Tropical malabsorption. In Postgraduate Medical Journal 82(974):779-787). |
|
|
Ridker PM, Hennekens CH, Buring JE, Rifai N (2000). C-reactive protein and other markers of inflammation in the prediction of cardiovascular disease in women. New England Journal of Medicine 342:836-843. |
|
|
Ross R (1999). Atherosclerosis - An inflammatory disease. New England Journal of Medicine 340:115-126. |
|
|
Saha AK, Schmidt BR, Wilhelmy J, Nguyen V, Do J, Suja VC, Nemat-Gorgani M, Ramasubramanian AK, Davis RW (2018). Erythrocyte Deformability As a Potential Biomarker for Chronic Fatigue Syndrome. Blood 132(1):4874-4874. |
|
|
Sankar J (2017). Thrombocytopenia. Indian Journal of Practical Pediatrics 19(4):338. |
|
|
Gad SC (1988). An Approach to the Design and Analysis of Screening Studies in Toxicology. International Journal of Toxicology 7(2):127-138. |
|
|
Sevindik M, Akgul H, Pehlivan M, Selamoglu Z (2017). Determination of therapeutic potential of mentha longifolia ssp. Longifolia. Fresenius Environmental Bulletin 26(7):4757-4763 |
|
|
Shamkuwar PB, Shahi SR (n.d.). Antimotility and antisecretory effect of Kutajarishta: An ayurvedic antidiarrhoeal formulation. Pelagia Research Library 3(1):71-75. |
|
|
Stevens KR, Gallo MA (1989). Practical consideration in the conduct of chronic toxicity studies, Principles and Methods of Toxicology. (2nd ed.). |
|
|
Gupta MS, Shivaprasad HN, Kharya MD, Rana AC (2006). Immunomodulatory activity of the Ayurvedic formulation "ashwagandha churna." Pharmaceutical Biology 44(4):263-265. |
|
|
Tatsumi N, Tsuda I, Akira F, Takubo T, Hayashi M, Matsumoto H (1999). Principle of Blood Cell Counter - Development of Electric Impedance Method. Sysmex Journal International. |
|
|
Tripathi NK, Ramaiah L, Everds NE (2014). Clinical Pathology: The Role of the Study Director in Nonclinical Studies: Pharmaceuticals, Chemicals, Medical Devices, and Pesticides. |
|
|
Kampen EJV, Zijlstra WG (1961). Standardization of hemoglobinometry II. The hemiglobincyanide method. Clinica Chimica Acta 6(4):538-544. |
|
|
WHO (2002). WHO launches the first global strategy on traditional and alternative medicine (2002). Central European Journal of Public Health. |
|
|
Wolford ST, Schoer RA, Gohs FX, Gallo PP (1986). Reference range database for serum chemistry and haematology values in laboratory animals. Journal of Toxicology and Environmental Health 18:161-188. |
|
|
Wu AC, Lesperance L, Bernstein H (2002). Screening for iron deficiency. Pediatrics in Review / American Academy of Pediatrics 23(5):171-178. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


