Full Length Research Paper

ABSTRACT
Off-label prescribing is very common among physicians, particularly among psychiatrists and there is limited information regarding the extent of the unapproved drug use in Makkah city. The objective of this study was to assess the prevalence of off-label indications for antidepressant, antipsychotic and antiepileptic and the strength of evidence supporting use of the prescribed drug for the respective indication. A case sectional study was conducted on 15,955 prescriptions from 1 October 2018 to 6 January 2019 based on patient medication records obtained from an electronic medical record (EMRs) - health information system (HIS) from King Abdulaziz Hospital in Makkah city, Saudi Arabia. Two official databases (Micromedex and Lexicomp) were used to evaluate dual primary outcomes the determination off-label and on-label prescriptions and the level of evidence supporting the off-label indications. It showed that in 3 months there were 15,955 prescriptions concerning antipsychotics, antidepressants and antiepileptics drugs were issued to 5292 patients. Out of total 15,955 prescriptions, about 2218 (13.9%) prescriptions were off-label prescriptions for 29 drugs. The most frequently prescribed by class, were antidepressants 1025 (46.3%) followed by antipsychotics 1005 (45.3%) then antiepileptics 188 (8.5%). Off-label drugs use is common in psychiatric department and when physicians prescribed antidepressants, antipsychotics and antiepileptics for off-label indication, most of these prescribed indications were not supported by strong scientific evidences. The risks and benefits of off-label use should be carefully weighed up prior to prescribing these agents.
Key words: Off-label, antipsychotics, antiepileptics, psychiatric, case sectional study.
INTRODUCTION
The legal, prescribed use of a drug in a way that has not been approved by the Food and Drug Administration (FDA) is commonly referred to as an “off-label use.” Off-label occurs when a drug is used for a certain disease being treated, a dose, duration of treatment, and for an age group of patients other than that not specifically addressed in the product labeling (Eguale et al., 2012; Wittich et al., 2012). This is different from prescription errors which are an avoidable medication errors that can occur in hospitals worldwide (Shrestha and Prajapati, 2019).
Antidepressants (ADs) are the 3rd most commonly prescribed medication in the United States (Mercier et al., 2013). A study has analyzed 106,850 ADs prescriptions and found that one-third (29.3%) of all ADs prescriptions were written for an off-label indication and among all ADs, Tricyclic Antidepressant (TCAs) had the highest off label prescribing. Only 16% of all off-label ADs prescriptions were supported by strong scientific evidence for the respective indication (Wong et al., 2017). In addition, anti-epileptic drugs are also one of the most common central nervous system (CNS) class that is frequently used for unapproved indication. In one of US large studies, it was shown that antiepileptic drugs were the most frequently used off-label and 83% of all off-label antiepileptic prescriptions were found to be associated with little or no supportive evidence (Franco et al., 2014). A retrospective study that has been conducted at a private hospital in Indonesia showed the off-label use of anticonvulsants occuring in one-third of patients receiving prescriptions of anticonvulsants (Rahajeng et al., 2018).
The most common off-label indications for ADs were: trazodone for insomnia, citalopram for anxiety, amitriptyline for pain, and amitriptyline for insomnia, while only amitriptyline for pain, escitalopram for panic disorders, and venlafaxine for obsessive compulsive disorder had a strong scientific evidence (Wong et al., 2017). On the other hand, atypical antipsychotics (AAPs) are FDA approved for the treatment of schizophrenia and bipolar disorders. Also, the antidepressant and antipsychotics undergo off-label uses such as treating depression, post-traumatic stress disorder, dementia, anxiety, obsessive-compulsive disorder, insomnia, eating disorders and substance abuse. For example, Quetiapine blocks histamine and serotonin type 2A receptors; therefore, it has been used as a commin off-label therapy for insomnia (Sartori and Singewald, 2019). A study conducted in the United states demonstrated that the use of AAPs between 1995 and 2008 has increased as well as its off-label use that doubled during this period (Varghese and Carroll, 2015).
A study found that off-label use which lacked strong scientific evidence had a higher adverse drug effects (ADEs) rate compared with on-label use. They also found that off-label use with strong scientific evidence had about the same risk for ADEs as on-label use (Eguale et al., 2016).
The most off label anticonvulsants used were oxcarbazepine (67.27%), carbamazepine (46.15%), pregabalin (45.45%), phenytoin (37.62%), valproate (25.34%), and gabapentin (18.28%); and they found that the most common off-label use fall in neurological (neuropathy pain, stroke, trigeminal neuralgia, cephalgia, petit) and psychiatric, than in rheumatic and renal disorders (Rahajeng et al., 2018). In the matter of adverse effects for AAPs, off-label use showed an increased risk of cardiovascular events and death (Varghese and Carroll, 2015). Cardiovascular symptoms, edema, and vasodilation events were more common in elderly patients with dementia taking olanzapine and risperidone. Another study that evaluated 5,106 of elderly patients with dementia showed a 1.6-1.7-fold increase in mortality among AAP users versus non-users (Varghese and Carroll, 2015). Quetiapine and Aripiprazole were not associated with cardiovascular risk, whereas risperidone was associated with an increased risk of stroke (Maher et al., 2011). On the contrary, there was lack of evidence for using AAPs in insomnia as well as its potential adverse reaction (Park et al., 2013).
Sometimes, the reasons for prescribing off-label treatment by physicians are often difficult to discern even after reviewing electronic medical records (Walton et al., 2008). Physicians may erroneously believe that the medications are safe and efficacious for an off-label use without emphasizing the prescribed drugs with strong scientific evidence (Fukada et al., 2012).
Although an estimated 29% of antidepressants are prescribed for off-label indications (Wong et al., 2016), It is unknown to what extent these off-label prescriptions are supported by scientific evidence. However, there are limited studies in Makkah region in Saudi Arabia that describe the overall magnitude of off-label prescribing or the consequences of prescribing antidepressant, antipsychotic and antiepileptic drugs for unevaluated or under evaluated indications.
Therefore, we aim in this study to assess the prevalence of off-label indications for antidepressants, antipsychotics and antiepileptics along with the strength of evidence supporting use of the prescribed drugs for the respective indication and applying cost analysis.
METHODOLOGY
Study design and setting
We conducted a case sectional study on 15,955 prescriptions for antidepressants, antipsychotics and antiepileptics. Drug prescriptions were obtained from 1 October, 2018 to 6 January, 2019 based on patient medication records obtained from an electronic medical record (EMRs) - Health Information System (HIS) from King Abdulaziz Hospital in Makkah city, Saudi Arabia.
Data collection and assessment
Data for this study were collected from the electronic medical records in King Abdulaziz Hospital. The EMRs consisted of patient information such as (patient name, age, diagnosis and drug therapy for the respective diagnosis). We used two official databases (Micromedex and Lexicomp) to evaluate the off-label and on-label prescriptions and determine the level of evidence supporting the respective indications.
Inclusion and exclusion criteria
We enrolled patients who were being treated with at least one drug of these three classes: antidepressants, antipsychotic and antiepileptics, and adult patients who are 18 years of age or older. We excluded all indications that were either not clear or suggest inaccurate prescribing. Any drug that is not available in King Abdulaziz Hospital such as all monoamine oxidase inhibitors, first generation antipsychotics (except haloperidol and fluphenazine) and antiepileptic drugs such as divalproex, felbamate, lacosamide, levetiracetam, oxcarbazepine, fosphenytoin, tiagabine and zonisamide were also excluded.
Outcomes and measurement
On-label versus Off-label indications
According to the Food and Drug Administration (FDA), the on-label or off-label drug use was classified according to the intended indication.
Indications were considered approved by FDA (on-label) if they could be matched to the therapeutic indication reported in the drug’s package labeling. Any indication that could not be matched to the labeled indication was considered off-label.
Level of evidence for off-label indications
For each off- label drug indication, the level of scientific evidence that support the drug’s overall efficacy was categorized using Micromedex and Lexicomp databases. We considered any data that was derived from meta-analyses of randomized controlled trials, with homogeneity of results and large numbers of patients as a data that has strong level of evidence. We also considered any data that was derived from meta-analyses of randomized controlled trials, with conflicting conclusions and involving small numbers of patients as a data that has moderate level of evidence while the lack of evidence exists when the data was derived from observational studies or from experts' opinion.
Accordingly, the following 2 variables were created: (1) on- or off- label use (2) off-label use with and without strong scientific evidence.
Cost of drug prescribed as off-label use for specific indication
One of the most commonly prescribed drugs was taken as off- label from three classes of antidepressants, antipsychotics and antiepileptics for treatment of insomnia. Thereafter, we compared between the costs so that we assumed all other factors constant such as efficacy, physician preference, side effects and strengths. We obtained the costs of all drugs from Saudi Drug and Food Administration (SFDA) authority. We calculated what would be the costs for treatment of insomnia assuming all prescriptions of insomnia were prescribed for at least 6 months.
Statistical analysis
Statistical analyses were performed using SPSS Var 23.0 software 2015.
To estimate the prevalence of off-label indications, the number of off-label prescriptions was divided by the total number of antidepressants, antiepileptic and antipsychotic prescriptions.
To estimate the level of scientific evidence for off-label prescriptions, the number of off- label prescriptions in each evidence category was divided by the total number of off-label antidepressant, antiepileptic and antipsychotic prescriptions.
To estimate the percentage of cost difference per 6 months, firstly we calculated the total cost for one month by the following formula: Cost per unit × Total number of units consumed per 6 months. Thereafter we calculated the percentage of cost variation by the following formula: Price of the most expensive brand / Price of the least expensive brand × 100 (Kamath, 2017); and cost ratio by the following formula: Price of the most expensive brand / Price of the least expensive brand (Kamath, 2017).
Ethics
Ethical approval was obtained from Umm Al-Qura University IRB commity UQU- COP-EA-#143912.
RESULTS
Prevalence of off- label indications
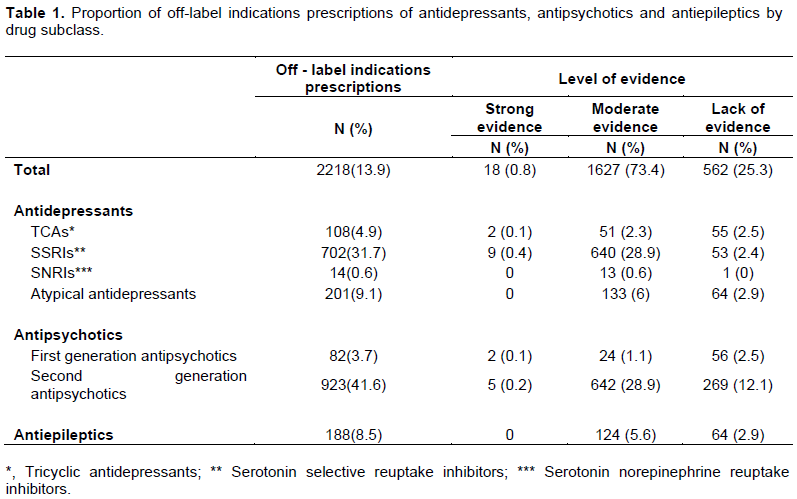
During the study period (October 2018 – 6 January, 2019), about 15,955 prescriptions concerning antipsychotics, antidepressants and antiepileptics drugs were issued to 5292 patients. Of the 15,955 prescriptions, 2218 (13.9%) prescriptions were off-label prescriptions for 29 drugs. The most frequently prescribed prescriptions were antidepressants 1025 (46.3%), followed by antipsychotics 1005 (45.3%), and then antiepileptics 188 (8.5%).
The largest subclasses of drugs (in numbers of off-label prescriptions) were second-generation antipsychotic (41.6%), serotonin selective reuptake inhibitors SSRIs (31.7%), atypical antidepressants (9.1%), tricyclic antidepressants TCAs (4.9%), first-generation antipsychotics (3.7%). By contrast, the prevalence of off- the label was much lower in serotonin-norepinephrine reuptake inhibitors SNRIs (0.6%), as shown in Table 1.
The most frequently prescribed drugs were quetiapine (31.8%), escitalopram (26.6%), mirtazapine (9%), olanzapine (4.1%), amitriptyline (4.1%), lamotrigine (3%), fluvoxamine (2.9%) and risperidone (2.7%) as shown in Table 2.
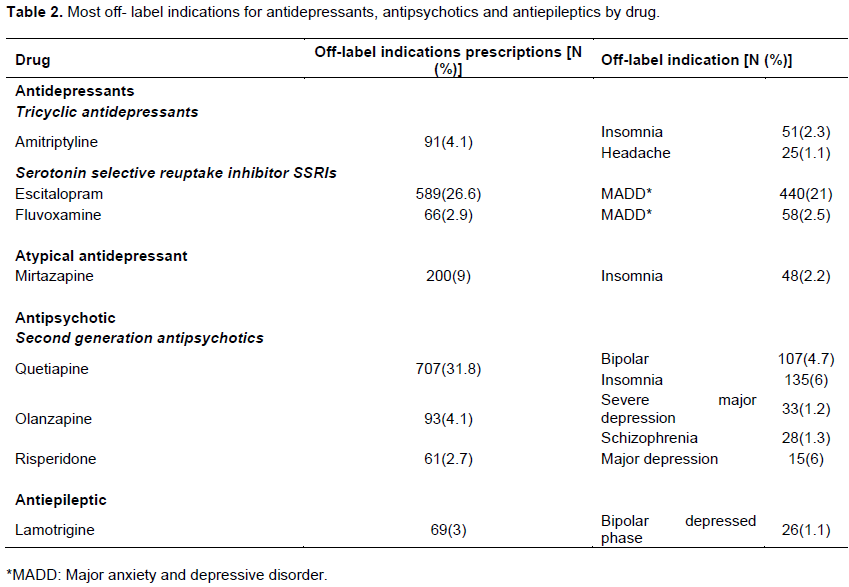
while amitriptyline, mirtazapine, and quetiapine for insomnia lacked scientific evidence as shown in Table 2.
Cost comparisons of off-label prescribed drugs used in management of insomnia
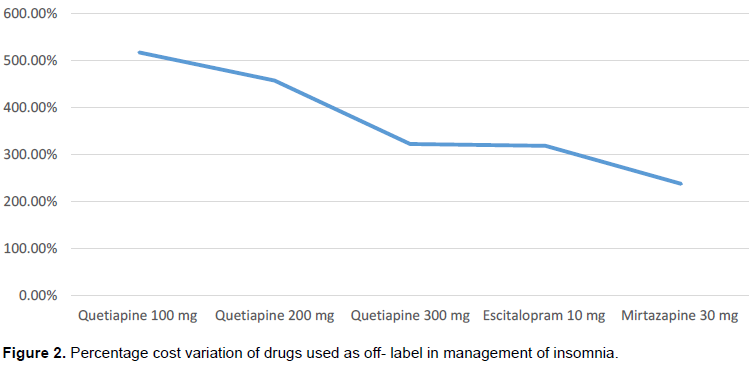
After analyzing the prices of 4 drugs that were used as an off-label in the treatment of insomnia, the results showed that there is a wide variation in costs of mirtazapine 30 mg, quetiapine 100 mg, 200 mg, 300 mg, amitriptyline 25 mg and escitalopram 10 mg as shown in the Table 3.
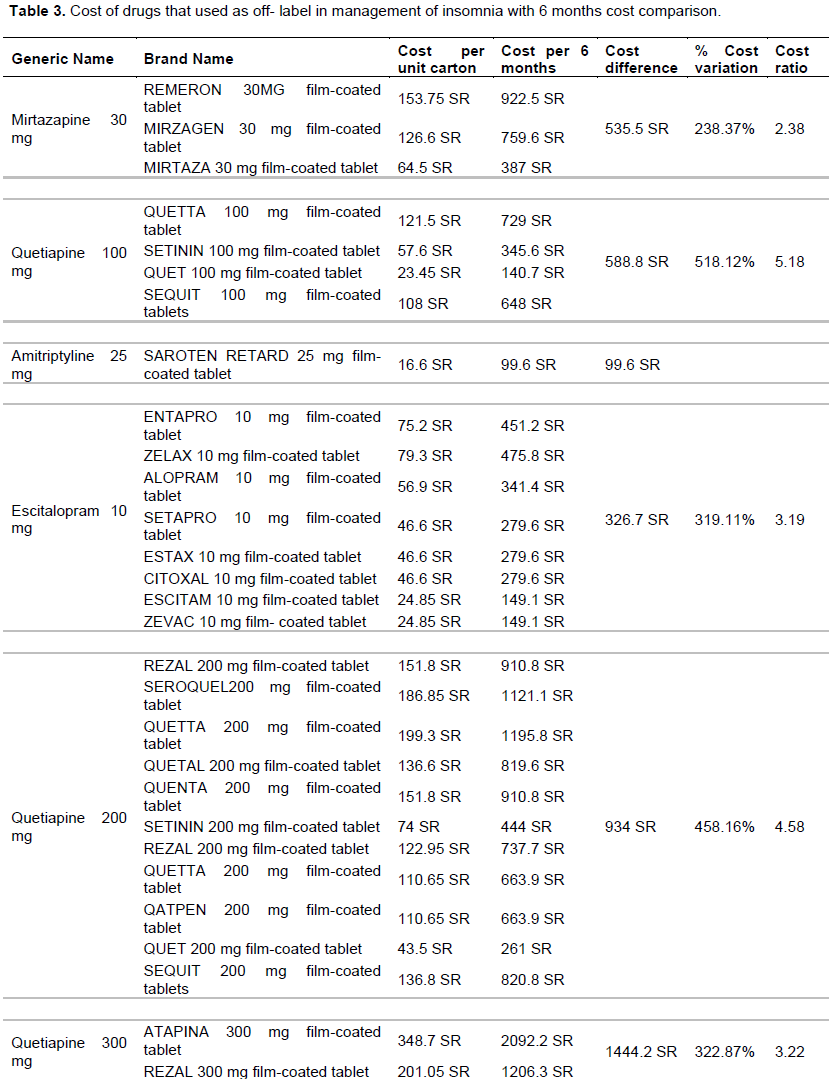
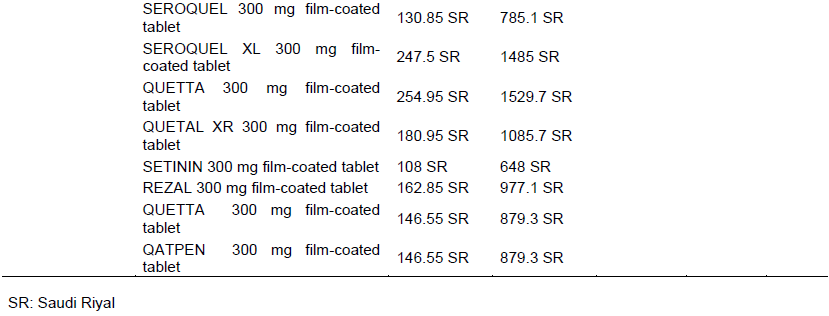
Among all drugs used for insomnia, the most expensive product was quetiapine 300 mg (ATAPINA) while the cheapest product was amitriptyline 25 mg (SAROTEN RETARD). When comparing the costs of these four drugs, there was a significant cost difference between these products. The cost differences calculated over 6 months showed that the highest difference was among quetiapine 300 mg, followed by quetiapine 200 mg, quetiapine 100 mg then mirtazapine, escitalopram while the lowest cost difference was in amitriptyline 25 mg as shown in Table 3. Among antidepressant drugs, escitalopram 10 mg showed the maximum cost variation of 319.11% and among quetiapine strength, the maximum cost variation showed in quetiapine 100 mg of 518.12% as shown in Figure 2.
DISCUSSION
To our knowledge, this is the first study to assess the prevalence of off-label indications for antidepressants, antipsychotics and antiepileptics and the strength of evidence supporting use of the prescribed drug for the respective indication in Makkah region.
Based on the above study, we found that the highest prevalence of off- label use was for antidepressants compared to (Tewodros Eguale,) which was the lowest drug class used as off-label indication. By subclass, the SSRIs had the highest prevalence of off-label indication for 702 prescriptions followed by atypical antidepressants (201 prescriptions) unlike previous study which shows that the TCAs have the highest number of off label prescriptions (9480) (Wong et al., 2017).
Wong et al. (2017) also showed that the amitriptyline was used for insomnia for about 4349 prescriptions and mirtazapine 473 prescriptions from the total 31,319 off-label prescriptions while our study had 51 prescriptions of amitriptyline and 48 prescriptions of mirtazapine from the total 2218 off-label prescriptions. Among all off-label antidepressant prescriptions, there were 837 prescriptions with moderate levels of evidence which unfortunately represent the highest level of evidence considered when prescribing off label antidepressants and 11 prescriptions for strong level of evidence unlike (Jenna Wong) who had 4977 prescriptions for the same level of evidence (Wong et al., 2017).
There is a consensus on the use of atypical AAPs for non-approved indications that continues to increase regardless of the lack of well-defined studies to support such use and unknown long-term use risks (that is, tardive dyskinesia) in non-psychotic patients, even if was used at low doses (Anderson and Griend, 2014).
For the second generation antipsychotics, the Table 2 shows that quetiapine has the highest percentage and number of prescriptions than other generations in patients with insomnia.
In a recent study, also quetiapine has been prescribed most frequently for off-label use, and the majority of reports was for insomnia; even with insufficient research of atypical APs for primary insomnia, prescribers still use it (Bashawri, 2013). Quetiapine was developed for the treatment of psychiatric disorders, but based on its H1 receptor antagonist, its use for insomnia could also be considered (Anderson and Griend, 2014).
For the antipsychotic drugs, Tewodros Eguale reported that quetiapine has (66.7%), olanzapine (54.2%) and risperidone (43.8%) off label use out of total off-label use for antipsychotics (43.8%) and none of them have strong evidence but all of them are considered to have moderate and lack of evidence; while in our study, we found highest level of evidence of second generation antipsychotics including quetiapine, olanzapine and risperidone for moderate level of evidence (Eguale et al., 2012).
Table 2 showed that the highest percentage of off-label use of anticonvulsants was for lamotrigine in patients with bipolar depressed phase.
AEDs in bipolar has been widely used since the discovery of the mood stabilizing properties of it. AEDs can be used as mood stabilizers in the treatment of bipolar disorders, like lithium. But unlike lithium, none of them has proved effective for both manic and depression (Onyenwenyi, 2008).
Adjunctive use of antidepressant drugs is common, but this practice may place patients with bipolar disorders at increased risk of developing hypomania, mania, or acceleration of the cycle. In a double-blind placebo-controlled study of lamotrigine monotherapy, the results of the study show that lamotrigine has significant antidepressant effectiveness in bipolar I depression and that clinical improvement is evident as early as the third week of treatment. Lamotrigine use was well tolerated in patients with bipolar I depression, with a similar side effect profile to placebo (Calabrese et al., 1999).
In another six-months open-label trial of lamotrigine with 67 patients, 39 of them entered the study with depressed phase, 9 (23%) of them had a moderate improvement and 18 (46%) had marked improvement, as measured by the HAM-D (Botts and Raskind, 1999). But lamotrigine still has a moderate level of evidence (category B) that it may increase the potential to cause unwanted side effects, so special caution is needed when prescribing this drug for an off-label indication.
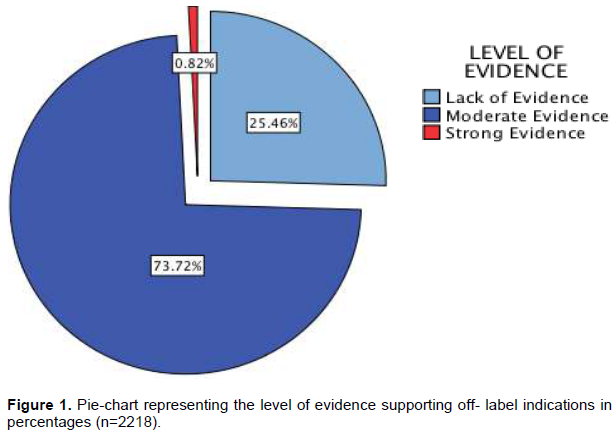
Figure 1 showed the proportion of the level of evidence for the off-label indication and we can see that the moderate evidence support has the highest percentage (73.72%) followed with ( 25.46%) of lack of scientific evidence support and only (0.8%) of off- label prescriptions that had strong evidence support which highlight a serious problem in prescribing off-label antidepressants because the incidence of adverse event might be higher than on label drug use and strong level of evidence of off-label drug use; so the clinician and pharmacist should be responsible and prescribe these kinds of drugs with caution and apply shared decision making process with patients.
In our study, insomnia was the indication that have been mostly prescribed for as an off-label. A study conducted in Makkah city to measure the prevalence of insomnia showed that among 463 participants, 29.4% suffered from insomnia (Bashawri, 2013).
The cost of the drug is an important factor that may affect the patient's compliance. Therefore, in this study, we analyzed the prices of the most commonly off-label used drugs in the treatment of insomnia.
Finally, our results showed that the there is a significant variation in the prices of amitriptyline, quetiapine, escitalopram and mirtazapine available in Saudi Arabia. Among these four drugs, quetiapine 100 mg showed the highest price variation (518.12%) while mirtazapine has the lowest price variation (238.37%).
CONCLUSION
This study has revealed that when physicians prescribed antidepressants, antipsychotics and antiepileptics for off-label indication, most of these prescribed indications were not supported by scientific evidence.
Highest prevalence of off-label prescribing was among second generation antipsychotics, where there is a need for appropriate monitoring for side effects and treatment response due to potential severe side effects (Varghese and Carroll, 2015).
When analysing the costs difference for the most common drugs used as an off-label for the treatment of insomnia, we found that the highest cost difference was in quetiapine (300 mg, then 200 mg and finally 100 mg) and the lowest cost difference was in amitriptyline 25 mg.
In this study, we had some limitations; we could not include adverse effects of off label drug use with our data due to the poor data documentation and this problem may lead to bigger confusion with clinicians and pharmacists who are in charge for drug dispensing of off label drug indications. Moreover, this study was conducted in one hospital setting in Makkah and cannot be generalised to the whole Kingdom.
In the future, there is a need for close communication between pharmacists and physicians to increase the effectiveness and to encourage evidence-based off-label drug use to optimize prescribing decisions.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
REFERENCES
|
Anderson SL, Griend JP (2014). Quetiapine for insomnia: A review of the literature. American Journal of Health-System Pharmacy 71(5):394-402. |
|
|
Bashawri H (2013). Sleepless in Makkah City, Saudi Arabia: Prevalence and Risk Factors of Insomnia and the Variations in Sleep Quality among Visitors of Primary Health Care Centers. MPH. Emory University. |
|
|
Botts SR, Raskind J (1999). Gabapentin and lamotrigine in bipolar disorder. American Journal of Health-System Pharmacy 56(19):1939-1944. |
|
|
Calabrese JR, Bowden CL, Sachs GS, Ascher JA, Monaghan E, Rudd GD (1999). A Double-Blind Placebo-Controlled Study of Lamotrigine Monotherapy in Outpatients With Bipolar I Depression. The Journal of Clinical Psychiatry 60(2):79-88. |
|
|
Eguale T, Buckeridge DL, Verma A, Winslade NE, Benedetti A, Hanley JA, Tamblyn R (2016). Association of Off-label Drug Use and Adverse Drug Events in an Adult Population. JAMA Internal Medicine 176(1):55. |
|
|
Eguale T, Buckeridge DL, Winslade NE, Benedetti A, Hanley JA, Tamblyn R (2012). Drug, Patient, and Physician Characteristics Associated With Off-label Prescribing in Primary Care. Archives of Internal Medicine 172(10): |
|
|
Franco V, Canevini MP, Capovilla G, Sarro GD, Galimberti CA, Gatti G, Perucca E (2014). Off-Label Prescribing of Antiepileptic Drugs in Pharmacoresistant Epilepsy: A Cross-Sectional Drug Utilization Study of Tertiary Care Centers in Italy. CNS Drugs 28(10):939-949. |
|
|
Fukada C, Kohler JC, Boon H, Austin Z, Krahn M (2012). Prescribing Gabapentin off Label: Perspectives from Psychiatry, Pain and Neurology Specialists. Canadian Pharmacists Journal / Revue Des Pharmaciens Du Canada 145(6). |
|
|
Kamath L (2017). Cost variation analysis study of oral anti-depressant drugs available in India. International Journal of Basic and Clinical Pharmacology 6(4):973. |
|
|
Maher AR, Maglione M, Bagley S, Suttorp M, Hu J, Ewing B, Shekelle PG (2011). Efficacy and Comparative Effectiveness of Atypical Antipsychotic Medications for Off-Label Uses in Adults. Jama 306(12):1359. |
|
|
Mercier A, Auger-Aubin I, Lebeau J, Schuers M, Boulet P, Hermil J, Peremans L (2013). Evidence of prescription of antidepressants for non-psychiatric conditions in primary care: An analysis of guidelines and systematic reviews. BMC Family Practice 14(1). |
|
|
Onyenwenyi AJ (2008). Off-label prescribing of anticonvulsant drugs. (Order No. 3381471, University of Florida). ProQuest Dissertations and Theses, p. 184. |
|
|
Park Susie H, Pharm D, BCPP, FCSHP (2013). Off-label use of atypical antipsychotics: Lack of evidence for their use in primary insomnia. Formulary 48(11):361-362,365-368,370-376. |
|
|
Rahajeng B, Ikawati Z, Andayani TM, Dwiprahasto I (2018). A Retrospective Study: The Off-Label Use Of Anticonvulsants At A Private Hospital In Indonesia. International Journal of Pharmacy and Pharmaceutical Sciences 10(5):119. |
|
|
Sartori SB, Singewald N (2019). Novel pharmacological targets in drug development for the treatment of anxiety and anxiety-related disorders. Pharmacology and Therapeutics 107402. |
|
|
Shrestha R, Prajapati S (2019). Assessment of prescription pattern and prescription error in outpatient Department at Tertiary Care District Hospital, Central Nepal. Journal of Pharmaceutical Policy and Practice 12(1):16. |
|
|
Varghese D, Carroll N (2015). Resource Utilization and costs associated with off-label use of atypical Antipsychotics in a Community-Dwelling Adult Population: Findings from the Medical Expenditure Survey. Value in Health 18(3): |
|
|
Walton SM, Schumock GT, Lee K, Alexander GC, Meltzer D, Stafford RS (2008). Prioritizing Future Research on Off-Label Prescribing: Results of a Quantitative Evaluation. Pharmacotherapy. The Journal of Human Pharmacology and Drug Therapy 28(12):1443-1452. |
|
|
Wittich CM, Burkle CM, Lanier WL. (2012). Ten common questions (and theiranswers) about off-label drug use. Mayo Clinic Proceedings. 356:982-90. |
|
|
Wong J, Motulsky A, Abrahamowicz M, Eguale T, Buckeridge DL, Tamblyn R (2017). Off-label indications for antidepressants in primary care: Descriptive study of prescriptions from an indication based electronic prescribing system. BMJ 356, j603. |
|
|
Wong J, Motulsky A, Eguale T, Buckeridge DL, Abrahamowicz M, Tamblyn R (2016). Treatment Indications for Antidepressants Prescribed in Primary Care in Quebec, Canada, 2006-2015. Jama 315(20):2230. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


