Full Length Research Paper
ABSTRACT
Hot flashes and night sweats commonly occur during menopausal transition period due to estrogen deficiency, but these conditions can also occur during postpartum period in which there are marked hormonal fluctuations. This study determined the prevalence and examined factors related to hot flashes and night sweats among the Japanese women in the postpartum period. The design of this study was a longitudinal investigation and the population of the postpartum women recruited was 229. A self-administered questionnaire that adapted Edinburgh Postnatal Depression Scale (EPDS) of measurement was used to collect data at 3 days postpartum, 2 weeks postpartum and one month postpartum. There was a significant association between transient night sweats and anxiety regarding family finances. Women who complained of hot flashes was 22.8% at 3 days postpartum and it decreased thereafter, while women who complained of night sweats were 58.6% at 3 days postpartum, 33.1% at 2 weeks postpartum and 15.2% at one month postpartum. In conclusion, hot flashes and night sweats among Japanese women in the postpartum period was associated with psychological and social factors.
Key words: Hot flashes, night sweats, postpartum women.
INTRODUCTION
The period in which drastic hormonal changes occur is an important period in a woman’s lifetime (Ishihara and Yasui, 2017). Although hot flashes and night sweats due to estrogen deficiency commonly occur during the menopausal transition period in women, these symptoms can also occur in other periods of marked hormonal fluctuation such as pregnancy and postpartum period (Gold et al., 2006). The level of estrogen markedly decreases after placental delivery, although secretion from the placenta is abundant during pregnancy (Moses-Kolko et al., 2009; Ruth et al., 2011). In a study conducted in Japan, it was reported that estradiol levels in postpartum women who had no menstruation until 12 months were 18.1 pg/ml at 3 months postpartum and 13.8 pg/ml at 12 months postpartum (Umeno and Miyazaki, 2008), which are low levels. Researchers also found that the mean durations of ovulation were 45 days after delivery in women with bottle feeding and 189 days after delivery in women with breastfeeding (Campbell and Gray, 1993). The endocrinological status including changes in gonadotrophin and estrogen levels is unstable during the postpartum period (Miyake et al., 1978).
Hot flashes and night sweats can occur in the periods of marked hormonal fluctuation such as pregnancy and postpartum period. It has been reported that 29% of postpartum women complained of nighttime hot flashes and that the proportion of women with hot flashes peaked at 2 weeks postpartum (Thurston et al., 2013). It has been found conducted a longitudinal study that the proportion of women with hot flashes and sweats was approximately 10-15% at one month postpartum (Gjerdingen et al., 1993). Furthermore, researchers found that the proportions of women who complained of hot flashes and excessive sweating were 11.9 and 23.0%, respectively, at 5 weeks postpartum and 5.9 and 7.4%, respectively, at 11 weeks postpartum among women who returned to work at 5 weeks postpartum (McGovern et al., 2007).
It has been reported that depressive symptoms, obesity and low level of education were risk factors for hot flashes in postpartum women (Thurston et al., 2013). Night sweats as well as hot flashes may also be caused by the psychological status. Conversely, the occurrence of hot flashes and night sweats may cause a poor psychological condition. If the status of hot flashes and night sweats and the association of these symptoms with psychological symptoms are clarified, psychological symptoms during the postpartum period may be reduced. Improvement of hot flashes and night sweats may be important for postpartum women if these symptoms are linked to psychological problems. 
There have been few studies on prevalence and factors related to hot flashes and night sweats during the postpartum period, hence this study was conducted. The aim of this study was to determine the prevalence and factors related to hot flashes and night sweats in postpartum women in Japan. In particular, focusing on the period from 3 days postpartum to one month postpartum in which estrogen level dynamically changes, we examined actual status and related factors of hot flashes and night sweats in postpartum women. The significance in this study is to have a proper understanding of physical changes for postpartum women women and to raise children with peace of mind.
MATERIALS AND METHODS
The design of this study was a longitudinal investigation, which was conducted between February 2017 and February in 2018. The sample size was 150 by using permissible errors (5%), reliability (95%) and a ratio of a population (50%). The sample size was determined to be 229, considering the number of uncollected sample. The postpartum women who gave birth through transvaginal or Cesarean section were recruited at birth centers in which birth number is approximately 750 per year in Kagawa prefecture and Tokushima prefecture in Japan. On the day of delivery and at 3 days postpartum, we requested postpartum women to participate in our study and we obtained agreement by signature on a consent form. At that time, we distributed three self-administered questionnaires at 3 days postpartum, 2 weeks postpartum and one month postpartum. The questionnaire was collected at 3 days postpartum through a collection box and at 2 weeks and one month postpartum by mail. Women who were taking medication for psychological diseases, women who experienced death or emergent hospitalization of newborn infants up until the day were requested to participate in the study, women who were having difficulties in answering the questionnaire because of insufficient recovery mentally and physically, and women who could not provide agreement and answer the questionnaire by their own will were excluded.
The contents of the questionnaire were as follows: background characteristics of the participant including age, marital status, presence advisor, menstrual cycle before pregnancy, infertility treatment, parity, method of delivery, satisfaction of delivery, gender of baby, number of baby, birth weight, anxiety regarding family finances, method of lactation and sleeping hours and a Japanese version of the Edinburgh Postnatal Depression Scale (EPDS) (Okano et al., 1996). With respect to the reliability and the validity of the scale, it has been shown that Cronbach’s coefficient alpha indexes were 0.67 at one month postpartum and 0.74 at 3 months postpartum, and the sensitivity was 0.75 and specificity was 0.93 (Okano et al., 1996). By using the Japanese version of the EPDS, the associations of impact of neighborhood environment and perinatal anemia with postpartum depression were reported in Japan (Miura et al., 2019; Maeda et al., 2020). EPDS is a 10-item self-administered questionnaire that was originally developed to screen for postpartum depression (Cox et al., 1987). For hot flashes and night sweats, the presence of these symptoms and the sites and frequency of the symptoms were examined.
Statistical analysis
Chi-square test was used to compare factors related to night sweats, while on way analysis of variance was used to analyzed the age. The chi-square test with Yates correction was used for menstrual regularity before pregnancy, infertility treatment, parity, method of delivery, anxiety regarding family finances, lactation method, EPDS score and sleeping hours. All statistical analyses were conducted with SPSS statistics ver.24 (IBM Corp.).
Ethical consideration
This study was approved by the Research Ethics Committee of Tokushima University Hospital (approval number 2702). An explanation sheet about the study was first distributed and followed by a consent form to the subjects. Participants who provided written informed consent were recruited and they were informed of their right to free participation and personal privacy protection.
RESULTS
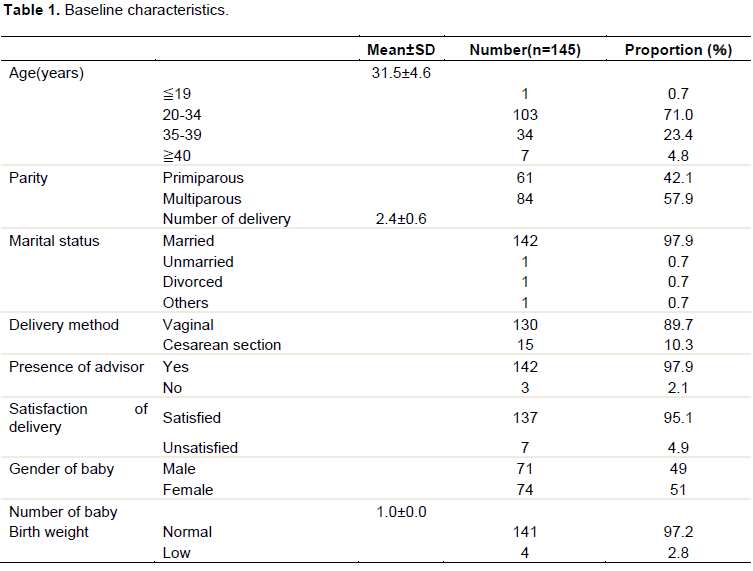
Two hundred and twenty-nine questionnaires were distributed to the participants in the two selected hospitals. The number of the participants who responded to the questionnaires at 3 days postpartum, 2 weeks postpartum and one month postpartum was 145 (63.3%). In Table 1, the mean age ± standard deviation of the participants at 3 days postpartum was 31.5 ± 4.6 years. The proportion of primiparous women was 42.1% and the proportion of multiparous women was 57.9%. The proportion of women with vaginal delivery was 89.7% and the proportion of women who received Cesarean section was 10.3%. The babies were all singletons and the proportion of babies with low birth weight was 2.8%.
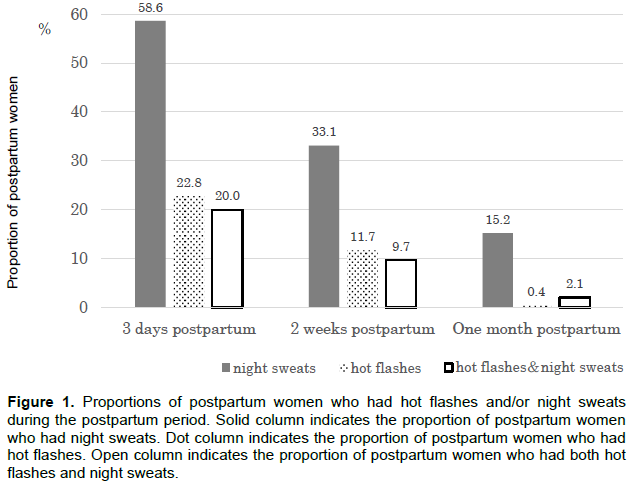
In Figure 1, the proportions of women who complained of hot flashes were 22.8% at 3 days postpartum, 11.7% at 2 weeks postpartum and 0.4% at one month postpartum. The proportions of women who complained of night sweats were 58.6% at 3 days postpartum, 33.1% at 2 weeks postpartum and 15.2% at one month postpartum. The proportions of women who complained of both hot flashes and night sweats were 20.0% at 3 days postpartum, 9.7% at 2 weeks postpartum and 2.1% at one month postpartum.
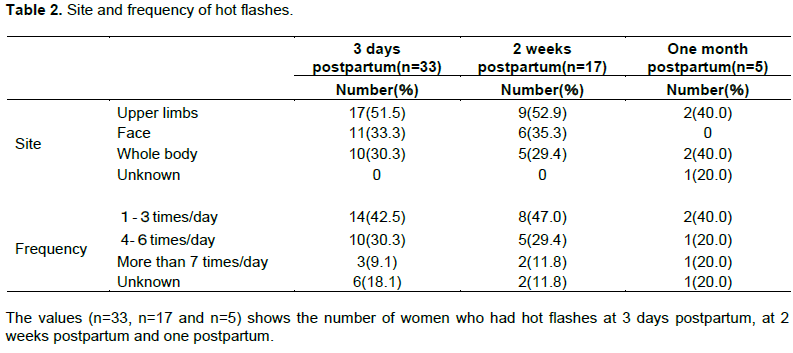
Among the women with hot flashes at 3 days postpartum, 2 weeks postpartum and one month postpartum, 40-50% of the women felt hot flashes in their upper limbs and 29-40% felt hot flashes over the entire body. Also, 33-35% of women felt hot flashes in their face at 3 days postpartum and 2 weeks postpartum, and there were no women who felt hot flashes in their face at one month postpartum (Table 2). In Table 2, the proportion of women who felt hot flashes in their upper limbs was higher than the proportions of women who felt hot flashes at the other sites at both 3 days postpartum and 2 weeks postpartum. At 3 days postpartum, the proportions of women in whom the frequencies of hot flashes were 1-3 times/day and 4-6 times/day were 42.5 and 30.3%, respectively. At 2 weeks postpartum, the proportions of women in whom the frequencies of hot flashes were 1-3 times/day and 4-6 times/day were 47.0 and 29.4%, respectively (Table 2).
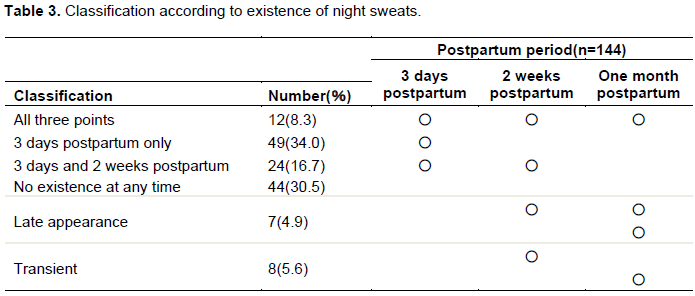
In Table 3, the postpartum women were divided into 6 patterns according to the presence and process of night sweats to examine factors related to night sweats. The proportion of the postpartum women with night sweats in all three periods was 8.3%. The proportion of the postpartum women without night sweats at any of the periods was 30.5%. The proportion of the women in whom night sweats had disappeared at one month postpartum was 16.7% and the proportion of the women whom night sweats had disappeared at 2 weeks postpartum was 34.0%. A woman whom night sweats appeared at 3 days postpartum and disappeared at 2 weeks postpartum and reappeared again at one month postpartum was excluded.
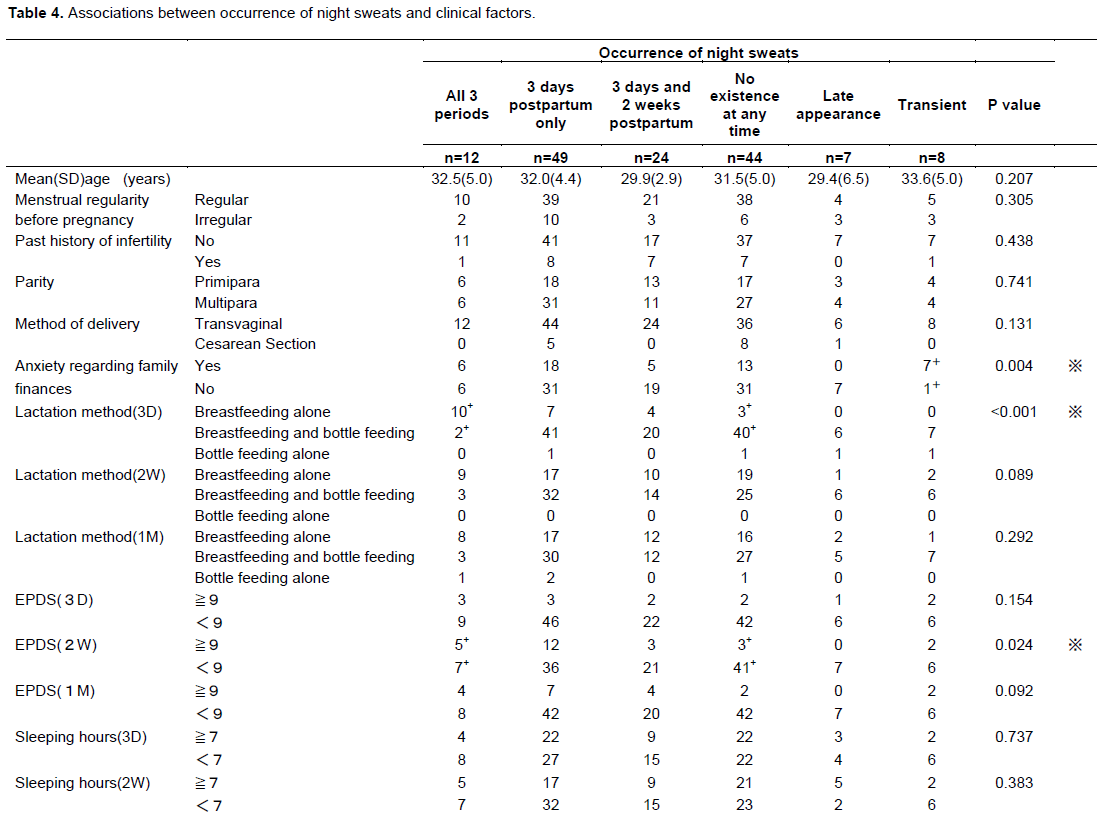
In the 6 patterns according to the presence of night sweats, factors related to night sweats including age, menstrual cycle before pregnancy, infertility treatment, parity, method of delivery, anxiety regarding family finances, method of lactation, EPDS score and sleeping hours were compared. There was a significant association between transient night sweats at 2 weeks or one month postpartum and anxiety regarding family finances (p=0.004). The presence of night sweats in all three periods was associated with breastfeeding alone as a lactation method at 3 days postpartum (p<0.001). The presence of night sweats in all three periods was associated with a high EPDS score (more than 9 points) at 2 weeks postpartum (p=0.024). On the other hand, the absence of night sweats in all three periods was associated with sleeping time of more than 7 h at one month postpartum (p=0.026) (Table 4).

DISCUSSION
In this study, it was found that the prevalence of night sweats (58.6% at 3 days, 33.1% at 2 weeks and 15.2% at one month) was higher than the prevalence of hot flashes (22.8% at 3 days, 11.7% at 2 weeks and 0.4% at one month) in the postpartum period. The results also showed that hot flashes occurred most frequently in the upper limbs. It has been reported that the proportion of women with hot flashes (42%) was higher than the proportion of women with night sweats (33%) during the climacteric period (Matsuzaki et al., 2014). It has also been reported that postpartum women during the first week after delivery wake up at night because of night sweats (Ricci, 2009). It has been suggested that the occurrence of night sweats during the postpartum period is due to reduction in the amount of body fluid retained during pregnancy and restoration to the body fluid level before pregnancy (Ricci, 2009). Thus, night sweats might be the most easily noticeable adaptation during the early postpartum period.
The proportion of women with hot flashes showed a peak (22.8%) at 3 days postpartum and decreased thereafter. It has been reported that the proportion of women who complained of hot flashes showed a peak (20%) at 2 weeks postpartum and then decreased to 14% at 12 weeks postpartum, 11% at 26 weeks postpartum and 10% at 52 weeks postpartum in USA (Thurston et al., 2013). The proportions of women with hot flashes at the peak were similar in Japanese women and women in USA. A peak of the proportion of women with hot flashes was different between women in Japanese women and women in USA. However, the pattern that a peak at the first period of survey decreases thereafter was similar.
The proportion of women who had night sweats was 58.6% at 3 days postpartum and decreased to 15.2% at one month postpartum. It has been reported that the proportion of women who had an increase in sweating was approximately 15% at one month postpartum (Gjerdingen et al., 1993). The prevalence of night sweats in this study was similar to that in the previous study by Gjerdingen at 1 month postpartum.
There have been no reports on factors related to the occurrence of night sweats. The finding showed that breastfeeding at 3 days postpartum was associated with night sweats. In one of the hospitals where the study was conducted, there were separate rooms for mothers and infants, and nursing is performed in the nursing room. Frequent lactation is needed for postpartum women during the period of insufficient milk secretion. Since infants are not sufficiently accustomed to drink milk and mothers are not sufficiently accustomed to breastfeeding in the early postpartum period, postpartum women have large physical and psychological burdens. Breastfeeding method at 3 days postpartum, was a large burden in the early postpartum period, and may cause night sweats. On the other hand, during the hypo-estrogenic state due to lactation, it has been reported that an increase in maternal skin surface temperature due to hot flashes could provide radiant heat for infant warming, particularly when infants are sucking (Naftolin et al., 1994; Pollycove et al., 2011). Thus, hot flashes may reduce metabolic stress for newborn infants and contribute to a survival advantage. However, it has been reported that there was no significant difference between the prevalence of hot flashes in women who gave birth within the past year and women who had not give birth within the past 2 years and their results did not support this study hypothesis that the reason for the occurrence of menopausal-like hot flashes in the postpartum period is to warm infants (Sievert and Masley, 2015). Also, the finding showed that the occurrence of night sweats was associated with sleeping hours at one month postpartum.
In Japanese Sleep Guidelines for Health Promotion in 2014, sleeping time of more than 7 h is indicated as a Japanese standard sleeping time (Ministry of Health, 2014). In postpartum women who do not have sufficient sleeping hours at one month postpartum, the mother’s daily life rhythm may be disturbed by the mother’s poor physical and psychological conditions caused by factors such as frequent nocturnal lactation and the infant crying at night. Since stress caused by insufficient sleep may induce the occurrence of night sweats, sufficient sleep is important for postpartum women.
Furthermore, the finding showed that the occurrence of night sweats at 2 week postpartum was associated with a high EPDS score. In the process of adaptation of postpartum women to a new daily life in which both mothers and infants live together in the home, women may have a large psychological burden at 2 weeks postpartum. Takehara et al. reported that the prevalence of maternal depression among primiparous women in Japan peaked at 2 weeks postpartum (Takehara et al., 2018). The intensity of psychological concerns in women at 2 weeks postpartum may affect the occurrence of night sweats. It has been suggested the presence of depressive symptoms is a factor related to hot flashes (Thurston et al., 2013). It is necessary for midwives to conduct medical interviews regarding mental health in postpartum women and provide care for the women by checking symptoms at 2 weeks postpartum. Lack of finance to care for a family can affect daily life any time during the postpartum period. Thus, transient night sweats might occur when postpartum women have anxiety about family finances.
The implication of the findings of this study is that women with severe hot flashes and night sweats may have psychological and social problems. Hot flashes and night sweats are symptoms that midwives can easily ask about and postpartum women can easily complain of. During the postpartum period, midwives should confirm the presence and degree of hot flashes and night sweats in postpartum women and should provide advice for dealing with issues that are causing these symptoms. It is important to approach psychological and social problems in relation to the symptoms by providing information about how to cope with discomforting symptoms such as hot flashes and night sweats.
This study has several limitations. First, the number of subjects was small and the results obtained are inconclusive for generalizability. This study was a longitudinal study during the postpartum period. We speculate that it was difficult for postpartum women to answer for the questionnaires and mail to us in each period. Postpartum women might be busy for child-caring and forget response of questionnaires. Therefore, the response rate might be low. We cannot clarify the direct associations of circulating hormone levels with hot flashes and night sweats. A prospective study on the factors associated with hot flashes and night sweats before pregnancy may be needed.
RECOMMENDATIONS
Based on the results in the present study, postpartum women can feel relieved and raise children positively since they have a proper understanding of physical changes occurred in their own bodies during the postpartum period. Midwives should confirm the presence and degree of symptoms and factors related to the symptoms in postpartum women and should provide advice for dealing with issues that are causing these symptoms. Further study of the effects of psychological symptoms with hot flashes and night sweats may be needed.
CONCLUSION
Women who complained of night sweats were 58.6% at 3 days postpartum and it gradually decreased thereafter, while women who complained of hot flashes was 22.8% at 3 days postpartum and it decreased thereafter in Japanese women during the postpartum period. The occurrence of night sweats was associated with anxiety regarding family finances, and breastfeeding at 3 days postpartum, a high EPDS score at 2 weeks postpartum and sleeping hours at one month postpartum.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors are grateful to doctors, midwives and medical assistants in Sanuki municipal hospital and Tsurugi-Handa hospital for supporting this research and also thank the women who participated in this study.
REFERENCES
|
Campbell OM, Gray RH (1993). Characteristics and determinants of postpartum ovarian function in women in the United States. American Journal of Obstetrics and Gynecology 169(1):55-60. |
|
|
Cox JL, Holden JM, Sagovsky R (1987). Detection of postnatal depression: development of the 10-item Edinburgh Postnatal Depression Scale. The British Journal of Psychiatry 150(6):782-786. |
|
|
Moses-Kolko EL, Berga SL, Kalro B, Sit DK, Wisner KL (2009). Transdermal estradiol for postpartum depression: A promising treatment option. Clinical Obstetrics and Gynecology 52(3):516-529. |
|
|
Gjerdingen DK, Froberg DG, Chaloner KM, McGovern PM (1993). Changes in women's physical health during the first postpartum year. Archives of Family Medicine 2(3):277-283. |
|
|
Gold EB, Colvin A, Avis N, Bromberger J, Greendale GA, Powell L, Sternfeld B, Matthews K (2006). Longitudinal analysis of the association between vasomotor symptoms and race/ethnicity across the menopausal transition: study of women's health across the nation. American Journal of Public Health 96(7):1226-1235 |
|
|
Ishihara R, Yasui T (2017). Health status of women in the recovery process of the hormonal changes. Journal of Kagawa prefectural University of Health Sciences 8:5-10. |
|
|
Maeda Y, Ogawa K, Morisaki N, Horikawa R, Sago H (2020). Association between perinatal anemia and postpartum depression: A prospective cohort study of Japanese women. International Journal of Gynecology and Obstetrics 148(1):48-52. |
|
|
Matsuzaki K, Uemura H, Yasui T (2014). Associations of menopausal symptoms with job-related stress factors in nurses in Japan. Maturitas 79(1):77-85. |
|
|
McGovern P, Dowd B, Gjerdingen D, Dagher R, Ukestad L, McCaffrey D, Lundberg U (2007). Mothers' health and work-related factors at 11 weeks postpartum. Annals of Family Medicine 5(6):519-527. |
|
|
Ministry of Health, Labor and Welfare, (2014). Sleep Guidelines for Health Promotion 2014. |
|
|
Miura R, Tani Y, Fujiwara T, Kawauchi I, Hanazato M, Kim Y (2019). Multilevel analysis of the impact of neighborhood environment on postpartum depressive symptoms. Affective Disorders. Available at: |
|
|
Miyake AK, Tanizawa OS, Aono TO, Kurachi KE (1978). Pituitary LH response to LHRH during puerperium. Obstetrics and Gynecology 51(1):37-40. |
|
|
Naftolin F, Whitten P, Keefe D (1994). An evolutionary perspective on the climacteric and menopause. Menopause 1(4):223-225. |
|
|
Okano T, Murata M, Masuji A, Tamaki R, Nomura J, Miyaoka H (1996). Validation and reliability of Japanese version of EPDS. Archives of Psychiatric Diagnostics and Clinical Evaluation 7:525-533. |
|
|
Ricci SS (2017). Essentials of Maternity, Newborn, and Women's Health Nursing 4th ed . Philadelphia: Wolters Kluwer P 507. |
|
|
Ruth AL, Robert ML (2011). Breastfeeding a guide for the medical profession 8 nd ed. United States of America: Elsevier P 689. |
|
|
Sievert LL, Masley A (2015). Are menopausal hot flashes an evolutionary byproduct of postpartum warming? Menopause 22(4):377-383 |
|
|
Takehara T, Tachibana Y, Yoshida K, Mori R, Kakee N, Kubo T (2018). Prevalence trends of pre- and postnatal depression in Japanese women: A population-based longitudinal study. Journal of Affective Disorders 225:389-394. |
|
|
Thurston RC, Luther JF, Wisniewski SR, Eng H, Wisner KL (2013). Prospective evaluation of hot flashes during pregnancy and postpartum. Fertil Steril 100:1667-1672. |
|
|
Umeno Y, Miyazaki F (2008). An examination of the transition of hormones in the blood of women during lactation. Japanese Journal of Maternal Health 49:327-335. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


