Full Length Research Paper
ABSTRACT
Trauma to the perineum following vaginal delivery is common and can lead to anal incontinence and pain but can be prevented by perineal support. However, the incidence and how to prevent perineal injury in sub Saharan Africa has not previously been described. The objective of the study was to assess the incidence of perineal trauma at vaginal delivery and to assess a training intervention in perineal support using a criterion-based audit (CBA) design. A CBA was conducted at Kilimanjaro Christian Medical Centre in Tanzania. In total, 552 women who delivered vaginally were included, of whom 80% completed a follow-up interview after three months. Perineal support as trained for this study was not performed before the intervention but was performed in 78.6% of deliveries after the intervention (p<0.000). The number of women with second degree lacerations decreased after the intervention (RR 0.74, CI: 0.61-0.90), and more had an intact perineum (RR 2.85, CI: 1.74-4.69). Anal sphincter lacerations were not significantly changed by the intervention (6.6 to 3.4%, RR 0.52, CI: 0.24-1.14). The frequency of anal incontinence changed insignificantly from 6.1 to 4.9% (RR 0.81, CI: 0.37-1.77) after intervention. Perineal pain three months after delivery was reduced by 72% (RR 0.28, CI: 0.15-0.52). The study demonstrates that CBA may be useful in introducing a simple intervention such as perineal support thereby decreasing the number of women having perineal trauma following vaginal delivery. However, the impact of our intervention on the sustainability of our observations is uncertain and must await long-term studies.
Key words: Clinical audit, developing countries, perineum, trauma, obstetric labor, complications.
Abbreviation: AI, Anal incontinence; OASIS, obstetric anal sphincter injuries; PFMT, pelvic floor muscle training; CBA, criterion-based audit; KCMC, Kilimanjaro Christian Medical Centre.
INTRODUCTION
An estimated 70 to 85% of women sustain some degree of trauma to the perineum during childbirth (Rikard-Bell et al., 2014; Webb et al., 2014). Correct prevention, diagnosis and management are essential to reduce the risk of short-term complications like bleeding, infection and pain.
Anal incontinence (AI) is defined as involuntary loss of flatus, liquid or solid stool (Bols et al., 2010). Vaginal childbirth and perineal trauma of third and fourth degree, also called obstetric anal sphincter injuries (OASIS), are important risk factors for AI (Bols et al., 2010; LaCross et al., 2015). Previous studies in low-income countries have demonstrated that AI may follow vaginal delivery up to 14% (Okonkwo et al., 2002; Obioha et al., 2015; Aguiar et al., 2019). AI often leads to limitations of daily activities, restrictions in social life, poor self-esteem and sexual dysfunction, all of which remain largely silent problems (Walker and Gunasekera, 2011). A simple option in order to reduce AI is pelvic floor muscle training (PFMT), which has been demonstrated to be effective for prevention and treatment (Boyle et al., 2014).
Perineal support is a technique developed to prevent perineal trauma at childbirth when the head is crowning. The thumb and index finger support the perineum, while the other hand slows the delivery of the head. Previous studies have demonstrated that this technique effectively reduce perineal trauma (Laine et al., 2012; Fretheim et al., 2013; Hals et al., 2010; Pirhonen et al., 1998; Aasheim et al., 2017).
The use of perineal support has not been described previously in low-income countries. Currently, we do not know if perineal support can be used to protect the perineum and thereby decrease the frequency of OASIS in these countries.
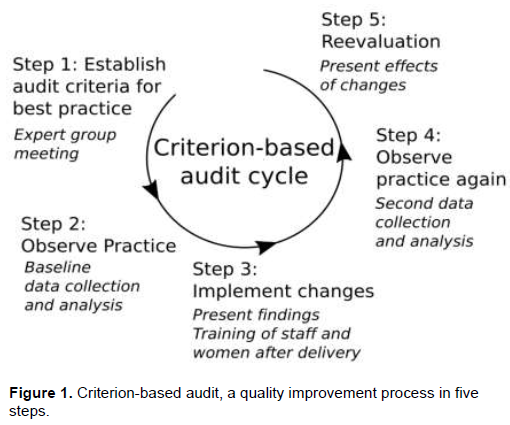
Several options are available to investigate of the impact of introducing new treatments. One way is the use of criterion-based audit (CBA) (Figure 1). CBA is a process that seeks to improve quality of care through systematic review of care against agreed criteria followed by implementation of change. Self-reflection and feedback through CBA have proven effective in both high- and low-income countries (Pirkle et al., 2011; Wagaarachchi et al., 2001; Siddiqi et al., 2005; Kongnyuy and Uthman, 2009).
The primary objective of this study was to assess the incidence of perineal trauma using CBA in a hospital in a low-income country. Secondary outcome was to assess the incidence of AI, perineal pain and to assess the impact of a training intervention.
MATERIALS AND METHODS
The study was conducted at Kilimanjaro Christian Medical Centre (KCMC), Tanzania. It is a referral hospital in the Kilimanjaro region.
The study was designed as a full CBA cycle (Figure 1). In step one audit criteria for best realistic practice regarding prevention, diagnosis and management of perineal trauma were established considering the resources available. The criteria for perineal trauma were established from evidence-based guidelines (Christiansen et al., 2015) and agreed on in cooperation with an expert group of one Danish and two Tanzanian consultants in obstetrics, and two midwives from KCMC. The audit criteria included classification of the trauma to the perineum into four categories. First-degree tears are limited to the superficial skin or vaginal mucosa. Second-degree tears involve perineal muscles, but with intact anal sphincter. Third-degree tears involve the anal sphincter. Fourth-degree tears involve both the anal sphincter and rectal mucosa. Third- and fourth-degree tears are called OASIS. Perineal support should be performed at all vaginal deliveries. Perineal trauma should be assessed by visual inspection and rectal examination and documented in the case files. Anal sphincter tears should be sutured by doctors.
In step two (Figure 1), baseline data were collected on a daily basis. The inclusion criteria were vaginally delivered women at KCMC with a gestational age of at least 28 weeks and a birth weight of ≥1000 g. Women were included over two periods of eight weeks from March to May (before intervention; baseline) and June to August 2016 (after intervention). All women were included after verbal and written informed consent after being assured strict confidentiality, and assurance that non-participation would not influence the care received.
Demographic data for the women were collected from their medical records, including age, parity, birth weight and other details about the delivery. Telephone numbers for the women and one relative were collected before discharge.
The first author (JM) observed a sample of deliveries for practice of perineal support and management of perineal trauma. For perineal support, it was noted if there was no support at all, if support was insufficient or sufficient as trained for this study.
Furthermore, JM examined all vaginally delivered women for perineal trauma. In case of perineal trauma, the degree of laceration was determined. Women who delivered during the day (7 am–6 pm) were examined directly after their delivery, before suturing. Women delivered during the night were examined the following day. In case JM observed OASIS not diagnosed by staff, they were notified.
Baseline data were analysed to assess the proportion of cases that met the audit criteria. Results were presented to staff, followed by a discussion to explore causes of substandard care and to suggest improvements.
Step 3 (Figure 1) included a 1 h hands-on training in perineal support for all residents, midwives and senior staff. Furthermore, the staff received training in the diagnosis of perineal trauma and treatment of AI by PFMT. Training of staff included theoretical lessons including themes emerging from the analysis of the baseline data collection. A Danish obstetrician and two Danish midwives carried out the training over a period of one week. The technique for perineal support was practiced on a pelvic delivery model. The Danish midwives supervised three deliveries at the delivery ward for further supervision.
All women were instructed in PFMT by a trained nurse before discharge and by a 4 min animated cartoon instruction video in Swahili.
After the intervention, another eight-week data collection period followed step 4 (Figure 1). A follow-up interview by telephone three months after delivery was conducted. A Swahili speaking research assistant performed the interviews. The interviewer was blinded with regard to all delivery details of the women. Symptoms of AI were assessed by the Jorge-Wexner score (Devesa et al., 2013; Jorge et al., 1993), translated into Swahili. The women were asked if they experienced perineal pain, if so to which extent; somewhat, moderately or very much. In addition, women were asked if they knew about PFMT, if they had performed it, and if so, how often.
Observations were compared to baseline data and presented to the staff (step 5, Figure 1).
Statistics
The outcomes were compared before and after the intervention as categorical data by a two-tailed Chi-squared test (or Fisher’s exact test for numbers five), and described as numbers, frequencies, relative risks (RR) and 95% confidence intervals (CI). The statistical software package SPSS 24 (SPSS Inc., Chicago, IL, USA) was used for all data analysis.
Ethical approval
Ethical approval was achieved from the research unit at KCMC, on 5 May 2016, No. 927 (Research No. 795) and from National Institute for Medical Research in Tanzania.
RESULTS
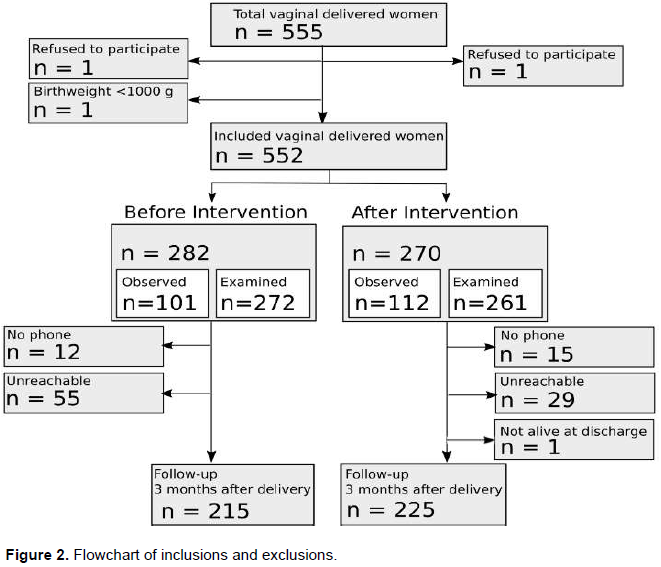
A total of 555 women delivered vaginally during both study periods, 552 met the inclusion criteria and agreed to participate (282 before the intervention and 270 after the intervention). The practice of perineal support was observed in a sample of 101 (35.8%) vaginal deliveries at baseline and 112 (41.5%) after the intervention. Clinical assessment of the women with perineal trauma was performed in 272 (96.5%) before and 261 women (96.7%) after the intervention, while 21 (3.8%) of the included women refused examination. In total, 440 women completed the follow-up phone interview three months after delivery (80%) (Figure 2).
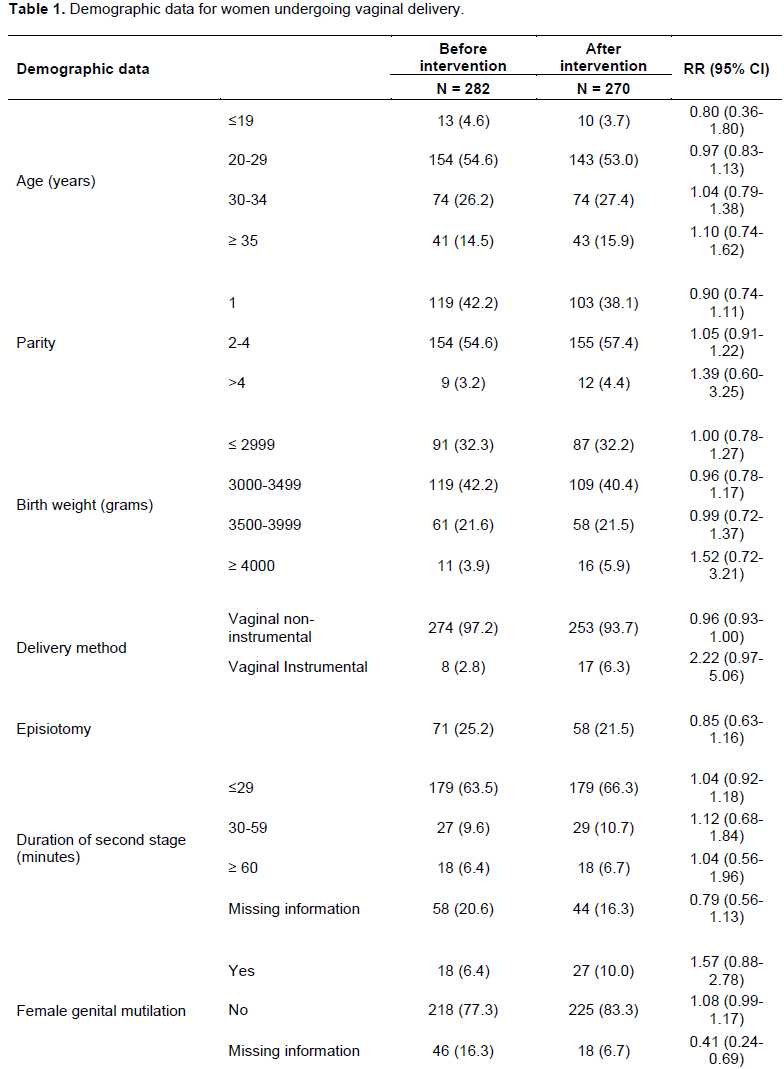
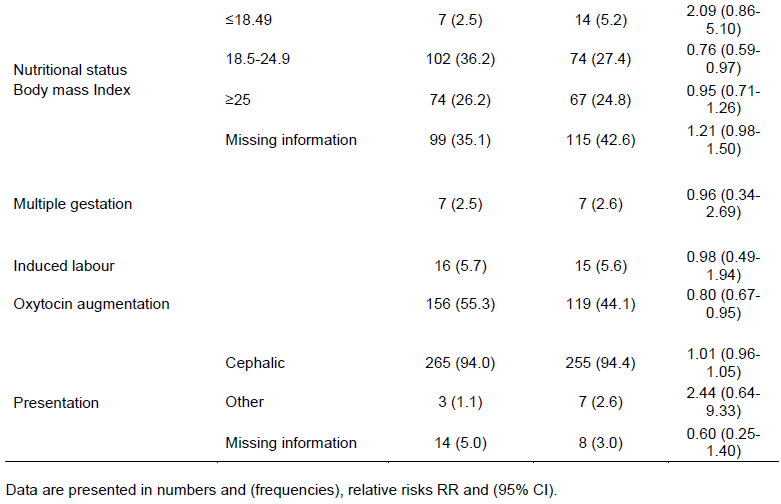
Demographic parameters appear from Table 1. Only oxytocin stimulation, nutritional status and female genital mutilation differed between the two groups.
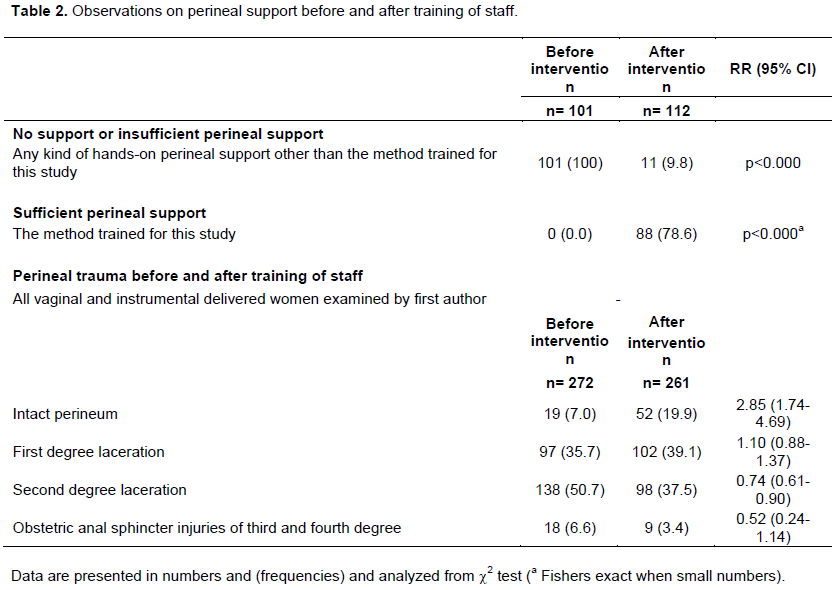
Before the training-intervention of staff perineal support as trained for this study was not performed at the hospital. However, a hands-on technique was used in 73% of the deliveries by applying the tips of the index and third fingers to pinch the perineum with a gauze swab and thus registered as insufficient perineal support (Table 2). After the intervention, perineal support as trained for this study was observed correctly at 78.6% of the deliveries (Table 2).
In total, 162 (30.5%) women were sutured immediately after delivery and before the assessment by JM was possible.
The proportion of women with no perineal trauma increased from 7.0 to 19.9% (RR 2.85, CI: 1.74-4.69) after the intervention, while second-degree lacerations decreased by 26% from 50.7 to 37.5% (RR 0.74, CI: 0.61-0.90). The incidence of OASIS was reduced from 6.6 to 3.4%, however not significantly (RR 0.52, CI: 0.24-1.14) (Table 2). Rectal examination in order to establish the degree of perineal trauma increased significantly comparing the two study periods (4.0 to 58.9%, p<0.001). The perineal trauma was documented in the case files in 47.7% before and in 73.7% after the intervention (RR 1.55, CI: 1.34-1.77). More women with OASIS were diagnosed and sutured by doctors instead of nurses, 20.0% before and 88.9% after intervention (p<0.001).
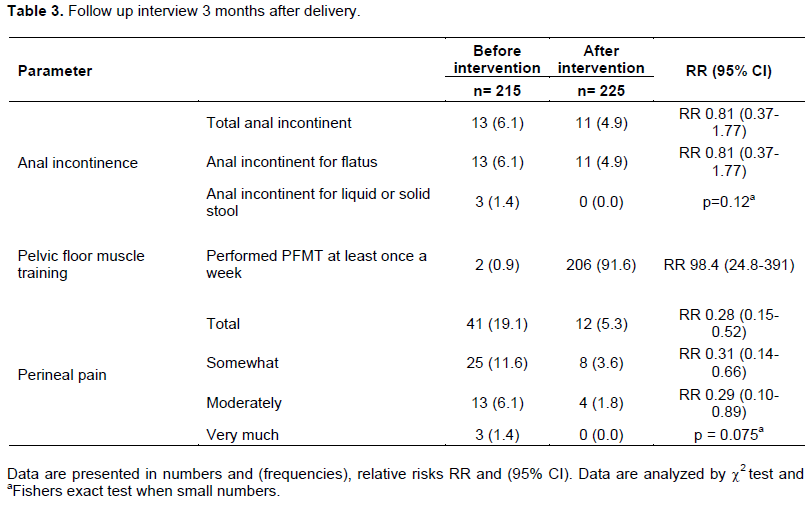
Before the intervention, 6.1% of the women reported AI where 1.4% also experienced incontinence for stools. After the intervention, 4.9% reported flatus incontinence and no women had incontinence for stools (RR 0.81, CI: 0.37-1.77). The number of women practicing PFMT regularly at least once a week increased from 2 (0.9%) to 206 (91.6%) after the intervention (RR 98.4, CI: 24.8-391). The number of women with perineal pain was reduced by 72% from 19.1% to 5.3% (RR 0.28, CI: 0.15-0.52) (Table 3).
DISCUSSION
The incidence of perineal trauma was high before the intervention, and prevention, diagnosis and management were insufficient. Our study demonstrates that the use of a CBA process increased the awareness of perineal support and may act to decrease the number of women with perineal trauma.
Furthermore, the intervention was followed by a better classification of the trauma, however without significantly decreasing the frequency of AI. The frequency of AI in our study prior to intervention was comparable with previous studies in Africa demonstrating a frequency of 7% or even higher (Okonkwo et al., 2002; Obioha et al., 2015; Aguiar et al., 2019; Walker and Gunasekera, 2011), but declined to a frequency comparable to that observed in the Nordic countries after the intervention, however not statistically significant (Laine et al., 2012; Fretheim et al., 2013; Hals et al., 2010; Pirhonen et al., 1998; Aasheim et al., 2017). Although decreasing AI is important, a more careful suturing and consequently lower pain perception as observed may follow a better definition of the degree of perineal trauma.
The CBA process is flexible and makes adaption possible to context and available resources. Relevant staff was involved throughout the process that resulted in a valuable mapping of suboptimal care, which provided a strong basis for tailoring an effective intervention. The selected audit criteria were simple and clear making the data collection feasible. The prospective study design allowed clarification of unclear documentation and thereby improved data quality. Together this made the intervention feasible for the low-income setting. This is in agreement with experiences with CBA in other conditions (Pirkle et al., 2011; Wagaarachchi et al., 2001; Siddiqi et al., 2005 and Kongnyuy and Uthman, 2009). For the improvements seen in this study to be sustainable, continued training and improvement of care and guidelines are important, which was out of the scope of this study.
This is, to our knowledge, the first intervention study to investigate the incidence and possibilities of prevention of birth-related trauma and subsequent complications in sub-Saharan Africa.
Telephone interviews were used as a feasible and inexpensive follow-up method as many women had access to telephones, and consequently a high follow-up rate on 80% was reached. This suggests that follow-up could be simplified in settings with limited resources and long distances between patients and hospitals.
A limitation is the study design not being a randomized controlled trial. However, such a trial is both ethically questionable and difficult to implement in a low income setting with valid data.
However, we cannot exclude that our results may be due to other circumstances than the intervention such as being present at the study site, improved registration, etc. However, other quality assurance interventions that could influence the results did not take place during the study period, neither were other major incidences like shortage of staff or supplies noticed. We are aware that sustainability is a problem, and that adherence to the instructions may decrease with time. This is a well-known problem, which has been described by others (Pirkle et al., 2011; Wagaarachchi et al., 2001; Siddiqi et al., 2005; Kongnyuy and Uthman, 2009).
The strong adherence among the women to the PFMT shows that the instruction video, when introduced by a trained nurse, was effective. Women were eager to receive advice from health professionals, which explains the high motivation to perform PFMT after delivery. However, the adherence is probably overestimated as a health-educated interviewer could be perceived as an authority figure, which could lead to exaggeration of how often PFMT was performed.
All clinical assessments and collection of data were performed by the same researcher, and all follow-up interviews were done by the same Tanzanian research assistant, making the before and after assessment comparable. However, the validity of the observations and categorization of trauma concerning the 30.5%, who were sutured before the assessment could be questioned. Another concern is the absence of blinding of JM who performed the clinical assessments. This could tend to underestimate the degree of perineal trauma wishing to see positive effects of the intervention. This was kept in mind, and observations were found to be done as meticulous and as objective as possible.
In conclusion, we observed that the incidence of perineal trauma was high and prevention, diagnosis and management were poor at the study site. Through the CBA process, perineal support was more frequently used, and perineal trauma and perineal pain after three months were reduced but not AI. Based on these findings we think that CBA can be used to improve quality of care in low-income settings. Regarding the impact on sustainability, further long-term studies are needed.
CONFLICT OF INTERESTS
The authors have not declared any conflict of interests.
ACKNOWLEDGMENTS
The authors thank all staff members at KCMC and Miss Elly Kimaro for doing the follow-up interviews. The study was funded by The Augustinus Foundation (grant number: 16-0082).
REFERENCES
|
Aasheim V, Nilsen AB, Reinar LM, Lukasse M (2017). Perineal techniques during the second stage of labour for reducing perineal trauma. Cochrane Database of Systematic Reviews, (6). |
|
|
Aguiar M, Farley A, Hope L, Amin A, Shah P, Manaseki-Holland S (2019). Birth-Related Perineal Trauma in Low- and Middle-Income Countries: A Systematic Review and Meta-analysis. Maternal and Child Health Journal.23(8):1048-1070. |
|
|
Bols EMJ, Hendriks EJM, Berghmans BCM, Baeten CGMI, Nijhuis JG, de Bie RA (2010). A systematic review of etiological factors for postpartum fecal incontinence. Acta Obstetricia et Gynecologica Scandinavica 89:302-314. |
|
|
Boyle R, Hay-Smith EJC, Cody JD, Mørkved S (2014). Pelvic floor muscle training for prevention and treatment of urinary and fecal incontinence in antenatal and postnatal women: a short version Cochrane review. Neurourology and urodynamics 33(3):269-276. |
|
|
Christiansen AG, Colding P, Elers J, Gommesen D, Jangö H, Kindberg S, Leenskjold S, Lund NS, Persson LG, Rasmussen OB, Skorstensgaard M, Westergaard HB (2015). Forebyggelse af Sphincterruptur, Sandbjerg Guideline. |
|
|
Devesa JM, Vicente R, Abraira V (2013). Visual analogue scales for grading faecal incontinence and quality of life: their relationship with the Jorge-Wexner score and Rockwood scale. Techniques in Coloproctology 17(1):67-71. |
|
|
Fretheim A, Odgaard-Jensen J, Røttingen J-A, Reinar LM, Vangen S, Tanbo T (2013). The impact of an intervention programme employing a hands-on technique to reduce the incidence of anal sphincter tears: interrupted time-series reanalysis. BMJ Open 3:e003355. |
|
|
Hals E, Øian P, Pirhonen T, Gissler M, Hjelle S, Nilsen EB (2010). A multicenter interventional program to reduce the incidence of anal sphincter tears. Obstetrics and Gynecology 116:901-908. |
|
|
Jorge MJN, Wexner SD (1993). Etiology and management of fecal incontinence. Diseases of the Colon and Rectum 36:77-97. |
|
|
Kongnyuy EJ, Uthman OA (2009). Use of criterion-based clinical audit to improve the quality of obstetric care: A systematic review. Acta Obstetricia et Gynecologica Scandinavica 88:873-881. |
|
|
LaCross A, Groff M, Smaldone A (2015). Obstetric anal sphincter injury and anal incontinence following vaginal birth: a systematic review and meta-analysis. The Journal of Midwifery and Women's Health 60(1):37-47. |
|
|
Laine K, Skjeldestad FE, Sandvik L, Staff AC (2012). Incidence of obstetric anal sphincter injuries after training to protect the perineum: cohort study. BMJ Open 2:e001649. |
|
|
Okonkwo JE, Obionu CN, Okonkwo CV, Obiechina NJ (2002). Anal incontinence among Igbo (Nigerian) women. The International Journal of Clinical Practice 56(3):178-180. |
|
|
Obioha KC, Ugwu EO, Obi SN, Dim CC, Oguanuo TC (2015). Prevalence and predictors of urinary/anal incontinence after vaginal delivery: prospective study of Nigerian women. The International Urogynecology Journal 26(9):1347-1354. |
|
|
Pirhonen JP, Grenman SE, Haadem K, Gudmundsson S, Lindqvist P, Siihola S (1998). Frequency of anal sphincter rupture at delivery in Sweden and Finland-result of difference in manual help to the baby's head. Acta Obstetricia et Gynecologica Scandinavica 77:974-977. |
|
|
Pirkle CM, Dumont A, Zunzunegui MV (2011). Criterion-based clinical audit to assess quality of obstetrical care in low- and middle-income countries: a systematic review. The International Journal for Quality in Health Care 23(4):456-463. |
|
|
Rikard-Bell J, Iyer J, Rane A (2014). Perineal outcome and the risk of pelvic floor dysfunction: a cohort study of primiparous women. Australian and New Zealand Journal of Obstetrics and Gynaecology 54:371-376. |
|
|
Siddiqi K, Newell J, Robinson M (2005). Getting evidence into practice: what works in developing countries?. International Journal for Quality in Health Care 17(5):447-454. |
|
|
Webb S, Sherburn M, Ismail KMK (2014). Managing perineal trauma after childbirth. BMJ 25:349(nov25 27):g6829-g6829. |
|
|
Walker GJA, Gunasekera P (2011). Pelvic organ prolapse and incontinence in developing countries: review of prevalence and risk factors. International Urogynecology 22(2):127-135. |
|
|
Wagaarachchi PT, Graham WJ, Penney GC, McCaw-Binns A, Yeboah Antwi K, Hall MH (2001). Holding up a mirror: changing obstetric practice through criterion-based clinical audit in developing countries. The International Journal of Gynecology and Obstetrics 74:119-130. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


