ABSTRACT
This article aims to translate and implement the cross-cultural adaptation of the WAST - Woman Abuse Screening Tool, designed in English and used to track violence by an intimate partner. For adaptation, the conceptual equivalence of terms and semantics between the original version in English and the version translated into Portuguese was evaluated, the result of two translations and back-translation, discussion by a panel of experts, establishment of the preliminary version and finally testing in 88 participants of both sexes, selected in two health units at the level of primary health care. The cross-cultural adaptation resulted in an equivalence of concepts and semantics between the initial translation and the final back-translation. From the testing it was concluded that the version of WAST translated and adapted to the Mozambican context, has good internal consistency, the scales of WAST-Short (α = 0.813) such as those of IPV or WAST-Long (α = 0.834) are highly related. The two scales do not discriminate between men and women (WAST-Short p = 0.204, WAST-Long p = 0.271). Implications are discussed for more effective HIV and violence prevention and treatment counseling.
Key words: Violence, intimate partner, instruments, adaptation, testing, intimate partner violence, HIV prevention, treatment.
Violence refers to the use of physical force or power, in threat or in practice, against oneself (self-inflicted), another person (interpersonal) or against a group or community (extra-family/community), which results or may result in suffering, death, psychological damage, impaired development or deprivation (WHO, 2013).
Intimate partner violence (IPV), a subtype of interpersonal violence, is a global problem that occurs in all social, economic, religious and cultural groups, affecting more women and children, resulting in high rates of physical and psychological trauma. It has been declared a public health problem as well as a violation of human rights (Harvey et al., 2007).
Surveys conducted in several countries like Asia, South America and Africa, identified high prevalence of physical (12.9 to 61.0%), sexual (6.2 to 58.6%) and psychological (19.6 to 75.1%) violence perpetrated by intimate partners against women (García-Moreno et al., 2005). Evidence has shown, for example, that there are different factors that influence IPV against women, such as patriarchal gender role norms, men's socio-economic power over women, poverty, unemployment, illiteracy (Zacarias, 2012). IPV also increases with HIV infection (Li et al., 2014).
In addition to these risk factors, and although IPV affects both sexes, contextualizing with the Mozambican socio-cultural reality, there are others exclusively typical of Sub-Saharan Africa that exacerbate the vulnerability of women, specifically the prevalence of practices that arise from traditional socio-cultural norms and values ??such as rites initiation, premature marriages of girls and traditionally established forms of marriage, which place women in a position of permanent subordination (Osório and Macuácua, 2013; Zacarias, 2012; Jewkes et al., 2002).
Screening refers to the examination of asymptomatic individuals for the presumptive identification of a disease not previously recognized, through tests, clinical or laboratory exams, which allow the classification of individuals into categories of suspected or not of having a certain disease or condition (Eluf-Neto and Wünsch-Filho, 2000). For victims of violence, screening aims to improve case detection, contribute to more appropriate interventions and thereby reduce exposure to violence and related problems. It is recommended for all women in external pediatric consultations, surgery, and those seen in the emergency services (Nelson et al., 2012). Screening is most effective when performed systematically.
However, a systematic review has documented that only 9 to 40% of clinicians screen for IPV (Todahl and Walters, 2011). More recent systematic reviews also identified other barriers to IPV screening including the perception of health professionals about IPV, personal discomfort with the subject, inadequate resources, lack of time, inadequate training or privacy for screening, perceptions that IPV screening is not the clinician's role, fear of offending patients, and lack of knowledge of how to deal with a woman who reveals positive results for IPV (Sprague et al., 2012; Matavel, 2020).
Some well-known IPV screening and diagnosis tools are the Revised Conflict Tactics Scales (CTS2), the Woman Abuse Screening Tool / Woman Abuse Screening Tool-Short Form (WAST / WAST-SF), Hurt, Insult, Threaten, and Scream (HITS), the Partner Violence Screen (PVS) and the Abuse Assessment Screen (AAS). The WAST - Women Abuse Screening Tool has been considered the most complete IPV screening tool for use in primary health care in developing countries, as it tracks all types of violence - psychological, physical and sexual (Iskandar, 2015). Indeed, in a systematic review of 33 studies, WAST was considered, among 4 instruments for screening violence (HITS, WAST / WAST-SF, PVS and AAS), the most reliable and valid for screening violence, with sensitivity of 47% and specificity of 96% (Rabin et al., 2009).
It is generally agreed that IPV is a public health problem, and its screening and diagnosis with specific tools, as well as compliance with standardized protocols, are essential elements in primary health care. However, despite the increasingly high rates of self-reported violence in Mozambican health facilities, the magnitude of IPV is still underestimated, due essentially, to the lack of screening and diagnostic tools in Mozambique's National Health Service. This gap can be filled with the introduction of effective screening instruments. Furthermore, considering the fact that women are only seen as victims and men as aggressors, it is necessary to consider the increasing number of cases of men who are victims of violence, particularly by their partners, which justifies the need of an IPV instrument for an inclusive screening.
Thus, this study aims to translate and cross-culturally adapt an intimate partner violence screening tool (WAST) for men and women in the Mozambican context. Further, it discusses the implications of the availability of this culturally adapted tool for clinicians who can now more effectively provide HIV prevention and treatment counseling in Mozambique and other Portuguese speaking countries, e.g., Angola, Brazil, and Portugal.
The WAST – Woman Abuse Screening Tool, is a short and easy to
understand instrument, developed in the United States of America by Brown et al. (1996), consisting of 8 Likert-type questions, which measure (a) the degree of stress in the relationship, (b) difficulty in resolving discussions, and (c) existence of violent episodes at an emotional, psychological, physical or sexual level (Binfa et al., 2018). It is the instrument for IPV screening chosen for cross-cultural adaptation, assessment of conceptual and term equivalence, and evaluation of semantic equivalence in Mozambique.
This evaluative process was based on the assessment of a discussion panel made up of five mental health and psychosocial care professionals, who also work in violence and the psychometric field.
A pre-test of the translated instrument was given to a group of participants who were interviewed individually. It consisted of four health professionals (1 male and 3 female) and six young students with higher education (3 male and 3 female). They were randomly chosen prior to the interview. The results were subsequently submitted to the discussion panel, and they certified the validity of the adapted instrument.
For testing of the adapted instrument, two health units in the city of Maputo were chosen for convenience. A total of 96 participants were randomly chosen. The participants represented the patients in the health units and were screened over three consecutive days.
Study design
The study consisted of a mixed approach with two components. The qualitative component completed the translation into Portuguese and assessed cross-cultural adaptation through the semantic and conceptual equivalence of the WAST instrument. It included a pre-test of the acceptability of the adapted version of WAST. The quantitative component consisted of testing the instrument using a cross-sectional study design. For its operationalization, the following techniques were used according to the type of approach:
Qualitative approach
Translation and cross-cultural adaptation of WAST for the Mozambican context
The cross-cultural adaptation includes a discussion panel made up of (five) mental health and psychosocial care professionals who also work in violence and in the psychometric field. It consisted of two stages, namely the evaluation of semantic equivalence and the evaluation of conceptual and term equivalence using an adaptation model proposed by Herdman et al. (1998). It accepts the possibility of correspondence without assuming equivalence between the constructs of the different cultures (Moraes et al., 2002). Constructs can have different equivalences, which must be confirmed so that a cross-cultural adaptation can be concluded.
Furthermore, following Moraes et al. (2002) during the instrument adaptation process, the concepts and dimensions of the original measures were studied in relation to the target culture of the new version. This assured conceptual equivalence.
Evaluation of semantic equivalence
This assessment was made from the perspective of referential meaning (the ideas or objects of the world that a single or a set of words allude to). If the referential meaning in the original and in the translated version is the same, there is a literal correspondence between them (Reichenheim, 2000). This process consisted of 4 steps:
Step 1 - Translation: Two independent and parallel translations of the instrument were carried out by professional translators from English to Portuguese (Trad 1 and Trad 2), after the objectives of the study had been explained to them. Although native to Mozambique, the translators are fluent in the English language, using it in their daily work both as translators and teachers of the English language.
Step 2 - Synthesis: The translations (Trad 1 and Trad 2) were delivered to a professional, Mozambican translator for a parallel and independent translation. This was done without knowing the characteristics of the previous translators, but with the information of the study objectives. The two translations in Portuguese were then compared with the original English version. The outcome was a single instrument translated into Portuguese (Trad A).
Step 3 - Back-translation: The harmonized translation (Trad A), was delivered to a translator whose native language was English, and he was and fluent in Portuguese. He translated the instrument in Portuguese (Trad A) into English (Ret A).
Step 4 - The instrument (Ret A) was submitted to another translator who was independent of the previous expert and fluent in English and Portuguese. This individual proceeded with the translation into Portuguese (Trad A_1). Subsequently, the semantic equivalence between the original and the back translation Trad A_1 was verified.
Evaluation of conceptual and term equivalence
This step was made based on the model proposed by Herdman et al. (1998). The equivalence between the first harmonized Portuguese translation (Trad A) and the final back translation into Portuguese (Trad A_1) was evaluated taking into account the meaning of the terms or words (conceptual and term equivalence). The correspondence of the general meaning of each question or answer option of WAST in the Portuguese version was compared to the original in English. This assured a correspondence in addition to the literality of terms, which took into account different aspects such as the questions' impact on the cultural context of the target population.
The panel verified and discussed the dimensions of the original instrument translated into Portuguese, its content, and the conceptual and semantic equivalence for cultural adaptation. The verification was based on the concepts of violence, its types and course, which were used in the guiding documents of the Mozambican Ministry of Health and clinical practice in Psychology. The instrument was compared to those used in western countries including the country of origin of the author of the instrument.
After this process and having confirmed the existence of a literal correspondence between words, terms, or concepts Trad A and Trad A_1, it was possible to propose a preliminary version of WAST translated into Portuguese and for use in Mozambique (WAST - M).
Pre-Test - In order to test the degree of acceptability of the proposed version, a total of 10 participants, consisting of 4 health professionals (1 male and 3 female) and 6 young students in higher education (3 male and 3 female), were chosen at random and invited to self-administer the questionnaire questions as if they were suspected of victims of IPV. Although WAST is an instrument designed to screen IPV in women, for the purposes of this study it was considered to test the same for both sexes in order to assess whether it could also be useful for a gender-inclusive screening process.
All participants were asked to mark the questions or terms they considered culturally incompatible or difficult to understand. After completing the 8 questions of the instrument, they answered a single cognitive question (PCg), at the end of the pre-test, which was added in order to assess the level of questions understanding.
For the cognitive question (PCg), which was a single question, respondents had three options: (1) Good, (2) Fair, (3) Bad. If most respondents considered options 2 and 3 in the cognitive question, the instrument would be returned for reassessment by the discussion panel. The same procedure would be followed if any term was contested by more than 50% of the participants regardless of their profile or gender.
The aggregated WAST-M responses were returned to the discussion panel, which read and considered the interviewees' reports of incompatible or difficult to perceive questions before recommending the preliminary version of the translated and adapted intimate partner violence tool (WAST) for the Mozambican cultural context.
Quantitative approach
Testing of the IPV instrument translated and adapted to the Mozambican cultural context (Portuguese) procedures
Through a simple randomization process, a sample was selected in 2 (two) health units in the cities of Maputo and Xai-Xai (one in the urban area and the other in the peri-urban / rural area). A total of 96 adults were selected to screen the culturally adapted WAST instrument.
Out of the total of invited participants, 88 (91.7%) agreed to participate in the study and the remaining 8 (8.3%) did not wish to participate. They presented justifications such as: conflicts with their jobs and unavailability to answer questions.
Inclusion criteria were: (a) patient in the health unit, (b) age 18 years or older, (c) married, or in an intimate relationship, (d) unaccompanied by the husband / wife or partner, (d) in good physical condition (observed and self-reported), (e) understands, speaks and reads the Portuguese language, (f) available to dedicate 5 to 10 min responding to interview that would be conducted by the researcher.
Exclusion criteria were: (a) patients diagnosed with mental and behavioral disorders, (b) illiterate, (c) exhibits signs of violence (objective or self-reported), and (d) accompanied by a husband / wife or partner.
Statistical analysis
The analysis was performed using the IBM® SPSS® statistical package. A significance level of 0.05 was applied in all tests. Means and standard errors, Pearson correlations (R), and principal component analysis were used to determine the number of interrelated dimensions underlying constructs in the WAST-M questionnaire.
The analysis yielded two scales based on the instrument's eight questions. Scale 1: WAST-M short (sum of questions 1 - 2) and Scale 2: IPV assessment or WAST-M long (sum of questions 3 - 8).
The WAST-M short scale ranged from 2 (very abusive) to 6 (not abusive). The IPV assessment or WAST-long rating scale ranged from 6 (very abusive) to 18 (not abusive).
The internal consistency of these scales was assessed using Cronbach's Alpha (α). A classification α <0.6 was unacceptable; between 0.6 and 0.8 was good, α≥0.8 was excellent (DeVellis, 2012). The scale of the shorter WAST-M was categorized using a cutoff value of 4 for positive (if the scale ≤ 4) and negative (if the scale> 4).
The Intra-Class Coefficient (ICC) was calculated to check the consistency or agreement of the values between the cases, based on a model of analysis of variance (ANOVA) of repeated measures with mixed effects, for consistency using average measures (Qin et al, 2019). ICC values are classified as weak if ICC <0.40, moderate if between 0.40 and 0.75, and excellent if ICC≥0.75. Tukey's additivity test was used to produce a test of the assumption that there is no multiplicative interaction between items or questions.
A canonical discriminant analysis was applied to investigate whether the items and the IPV rating scale could discriminate between sex and between the short WAST-M categories (positive and negative).
Evaluation of semantic equivalence
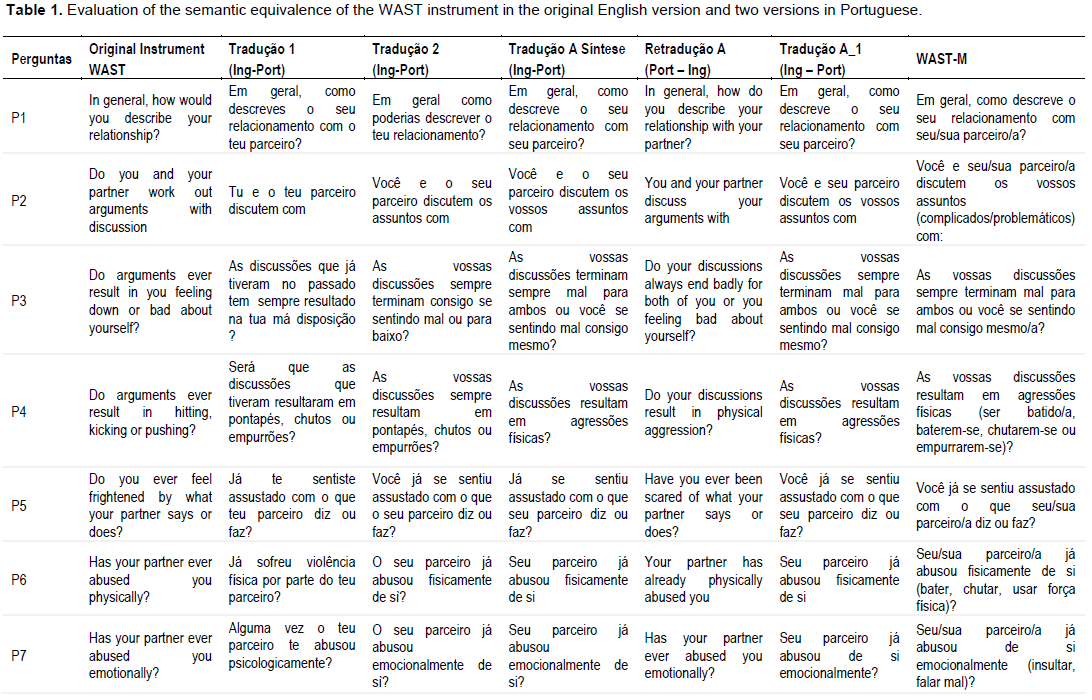
Table 1 summarizes the results of steps 1 to 3, with the items of the original instrument in English, the two translations, the synthesis of the translations, the back translation and the final translation into Portuguese. Still in the same table, the final result is presented - the adapted instrument resulting from the evaluation of semantic, conceptual and term equivalences.
Conceptual and item equivalence assessment
After combining the first two English-Portuguese translations (Trad A), the discussion panel concluded that there were no apparent difficulties in understanding the questions. However, it suggested changing some response items:
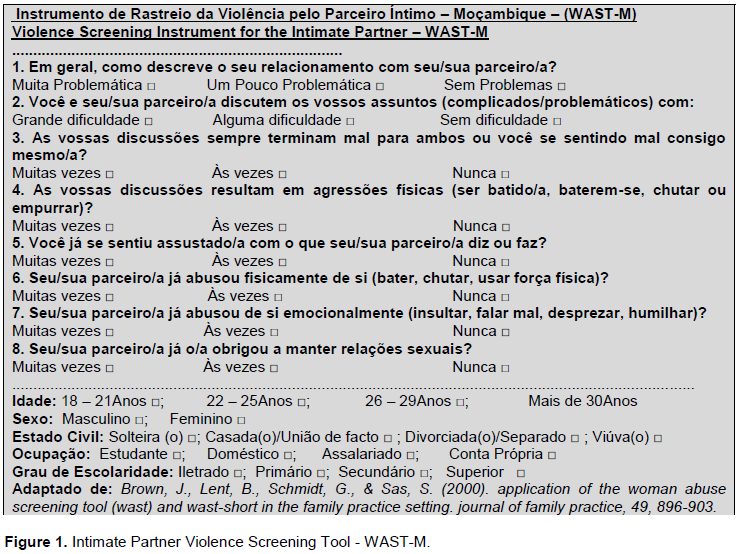
Regarding the first question (P1) about the general description of the relationship (Figure 1), the response "tension" was changed to "problem" because the word "tension" is considered difficult to understand, particularly for less educated people. The word “problem” was considered more appropriate and easy to understand both from the point of view of meaning and of context. Thus, the answer options for the first question (P1) became: “Very problematic”, “Occasionally problematic”, “Without problems”.
Another issue discussed was in relation to the term “abuse” (P6, P7) where one of the experts on the discussion panel suggested the possibility of changing it, as he thought it was of relative interpretation in the Mozambican context:
"Often the husband does not abuse, he can compel or force the woman to have sex" – Panel Member # 3.
However, after the discussion, the group decided to keep the term “abuse” as a way of raising awareness among professionals and society to recognize that the act of forcing or compelling the other, constitutes a form of abuse:
"In one way or another, compelling, forcing the woman, or the man, to have sexual relations or unauthorized intercourse is a type of abuse. We agreed on this definition." - Panel Member # 1.
Finally, the discussion panel suggested and agreed that in the questions related to physical, emotional and sexual abuse (P6, P7, P8); the following examples should be listed:
a) Physical abuse - hitting, pushing, kicking,
b) Sexual abuse - forcing you to have sex, forcing you to accept sexual positions or practices,
c) Emotional abuse - insulting, speaking ill, despising, humiliating.
Pre-test: The 10 participants (4 health professionals - 1 male and 3 female) and (6 young students of higher education - 3 male and 3 female), who were chosen at random and contacted individually, responded to the instrument in an average time of between 4 and 7 minutes. This was the maximum time frame in which the respondent had to reflect a little more on the question and on their relationship. Of this group, fifty percent agreed that forced sexual relations were abuse. All of the respondents reported that they had a "good" understanding of the questions.
With these results, the discussion panel considered the translation and cross-cultural adaptation of WAST (Trad A_1) for the Mozambican context to be satisfactory and agreed to accept the final version of the instrument called Violence Screening Instrument for the intimate partner – WAST-M (Figure 1).
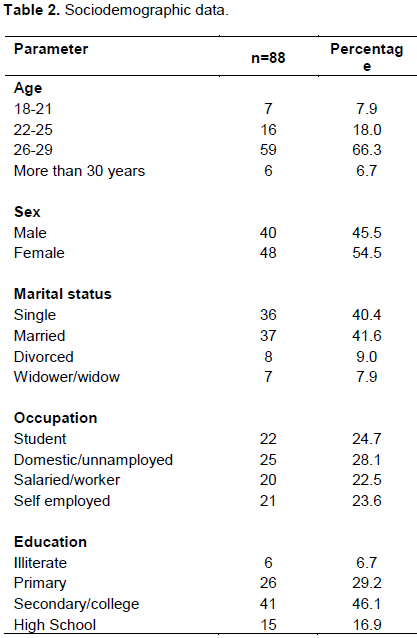
A total of 88 patients were evaluated, of which 48 (54.5%) were female and 40 (45.5%) were male, most were in the 26 to 29 age group (67%). Almost half (46.1%) had some level of education and 28.1% were unemployed (Table 2).
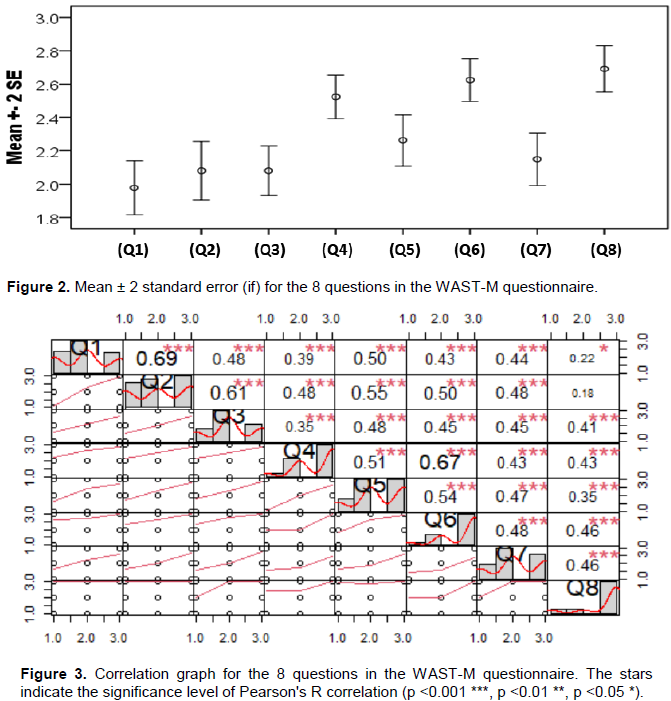
The average scores for Q1, Q2 and Q3 were relatively low, indicating that a large number of patients suffered from abusive violence by their intimate partner (Figure 2).
Correlations were low to moderate most pairs of questions (Figure 3), with the highest correlation observed for pairs Q1 and Q2 (R = 0.69, p <0.001) and Q4 and Q6 (R = 0.67, p <0.001).
Determination of the number of scales in the WAST-M questionnaire
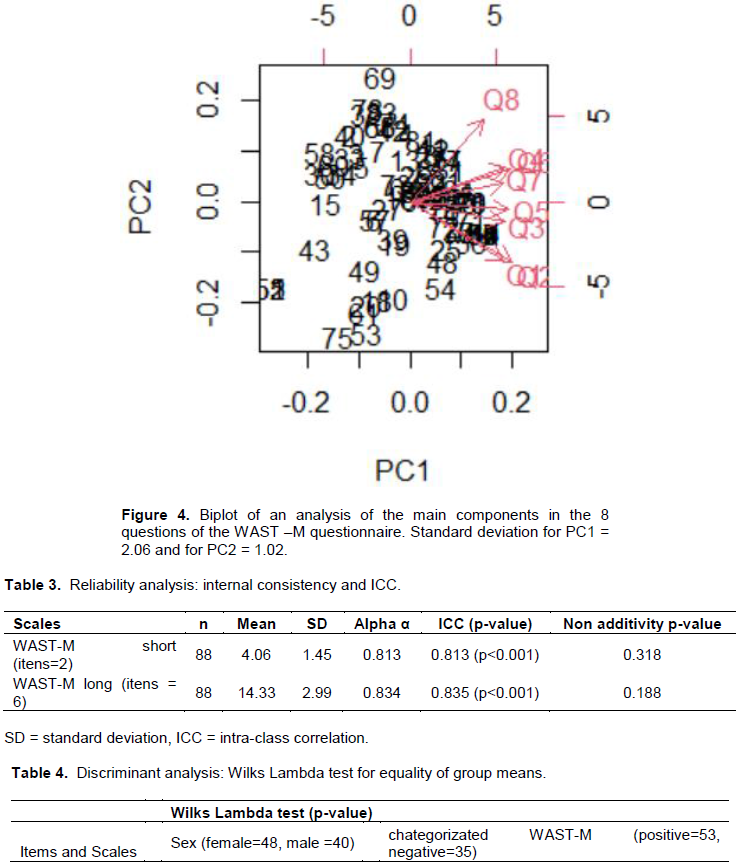
The correlations also indicate the existence of two underlying constructs, as shown by the results of the principal component analysis (PC) below (Figure 4), where the first two principal components explained almost 70% of the total variation in the 8 questions and had deviations greater than 1.
PC1 was highly correlated with Q1 and Q2, while PC2 was highly correlated with Q4, Q6 and Q8. This clearly indicated that, although the instrument is generally implemented using the 8 questions, there are two scales that can be assessed separately: short WAST-M (Q1 and Q2) and long-term VPI or WAST-M (Q3 - Q8).
Reliability of scales
Cronbach's Alpha (α) for both scales was greater than 0.8, which indicates good internal consistency, that is, that the items of the short WAST-M short scales (α = 0.813) and the IPV assessment or WAST-M long scales (α = 0.834) are highly related to each other. In addition, the intraclass correlation was excellent for both scales (ICC> 0.8), an indication of good inter-patient consistency or repeatability of the questionnaire (Table 3).
Tukey's additivity test for both scales failed to reject the null hypothesis. Therefore, the items on both scales had no multiplicative interaction and can be added together or accumulated.
The average score for the WAST-M short form was 4.06 with a standard deviation of 1.45. Using this mean value as a cutoff point for a dichotomized version of this construct, 53 patients (50.9% men and 49.1% women) had a positive intimate partner violence score (positive IPV), and 35 patients (62.9% women and 37.1% male) had a negative score for intimate partner violence (negative IPV).
Gender discrimination
The results of the discriminant analysis, shown in Table 4, demonstrate that both scales could not discriminate between men and women (WAST-M short p = 0.204, IPV assessment or WAST-M long p = 0.271), nor the individual items that make up these scales (p> 0.05).
Routine screening for violence in general and intimate partner violence (IPV) in particular is highly recommended and the existence of specific instruments is important for this purpose, taking into account the contexts of each country.
In fact, it is essential to choose among those that already exist; an instrument that can be adapted to the social and cultural context of each country, but it must be adapted, tested and validated for that purpose (Fogarty and Brown, 2002). However, research suggests that there is no perfect instrument for tracking violence by an intimate partner (Iskandar et al., 2015).
In terms of socio-demographic characteristics, our results indicate that 54.5% of females and 45.5% of males reported that they were able to discuss their IPV experiences with a healthcare professional. This is important because as Brown et al. (2000) noted, victims of IPV must feel perceived and heard in a respectful and supportive way when they speak to a healthcare professional about violence and abuse.
The correlations carried out allowed the authors to conclude that although WAST is usually applied in the long version, with 8 questions, in the adapted version (WAST-M) there are two scales that can be evaluated separately, the WAST-M short (Question 1 and Question 2), and the IPV Assessment or WAST-M long (Questions 3 to 8). These data confirm the characterization of the WAST as a single instrument divided into two parts, where the WAST-short consisting of the first two questions, was used to trace the presence of abuse, while the remaining six questions were used for a complete assessment of IPV in relation to the three areas of IPV - physical, sexual and psychological (Salahi et al., 2018).
The results of Cronbach's Alpha (α) for the two scales were above 0.8, which indicates that the adapted instrument has good internal consistency, with a great correspondence between the items of the two scales: WAST-M short (α = 0.813) as well as WAST-M long (α = 0.834), as well as an excellent intra-class correlation (ICC>0.8). This is an indicator of good inter-patient consistency or repeatability of the questionnaire, corroborating the findings of Basile et al. (2007) for which several studies reported that WAST has a high reliability, good specificity and sensitivity, and that it can additionally be applied in its short and long versions.
The analysis of the results also showed that the two scales do not present discrimination between genders (WAST-M short p = 0.204, WAST-M long p = 0.271), nor do the individual items that compose the scales (p> 0.05).
This is a new feature in this cross-cultural adaptation to Portuguese, as WAST is an instrument designed for screening IPV in women, which, however, will be of great value for screening in both sexes.
Furthermore, the results of this study suggest the need for additional studies, particularly aimed at validating the adapted instrument in relation to other instruments or procedures that can be considered “gold standard”, in order to allow its use in the context of the national health service of Mozambique.
Although the results revealed WAST-M as a simple, easy to apply and comprehensive IPV screening tool, it can be used by any health professional and any care service. This is especially important in providing HIV prevention and treatment counseling. HIV/AIDS focused health services offer a significant point of entry for locating, informing, and serving women affected by violence. Giving individuals doing HIV counseling and persons treating persons domestic violence the WAST and instruction on the interrelations of both epidemics will sensitize them to the importance of connecting with related services such as psychosocial therapy, prevention of mother-to-child transmission (pMTCT), and anti-retroviral treatment (ART) (WHO, 2017; Li et al., 2014). For primary health care, the challenge remains in the development of consistent and effective violence prevention and victim care policies, including intersectoral coordination (Binfa et al., 2018).
Violence in general and intimate partner violence in particular (IPV), are sensitive and complex issues. Thus, asking about these behaviors in a context in which violence is underreported, and often legitimized by cultural norms, was an obstacle encountered and limitation of this study. However, once the objectives of the study were explained and potential participants learned that abused participants would receive professional assistance, we were able to overcome this issue and obtain good participation.
Nevertheless, the fact that this clinical study was carried out in only one geographical area of the country with a heterogeneous population with regional customs and cultural norms may limit generalization of the results. Therefore, further validation of our instrument must be attempted in other regions of Mozambique and in other African countries.
Formal authorizations for the translation and adaptation to the Mozambican context in Portuguese was granted, by the author of the original instrument WAST - Woman Abuse Screening Tool.
All subjects who agreed to participate in the study signed a consent form, after the objectives and procedures of the study were explained to them.
This study was approved by the Bioethics Committee of the Faculty of Medicine of the Eduardo Mondlane University in the city of Maputo - Mozambique.
This study allowed for the translation and cross-cultural adaptation of the WAST screening instrument for IPV. Conceptual and semantic equivalence between the original instrument in English and the version adapted for Portuguese in a Mozambican context was achieved without major changes.
From the testing of the adapted instrument, it was concluded that the version of WAST translated and adapted to the Mozambican context, has good internal consistency, the scales of the two components of the WAST-Short instrument and the assessment of IPV or WAST-Long are related. Further, the two scales are valid for both men and women. Thus, the WAST-M is an appropriate instrument for the screening of violence by the intimate partner in the Mozambican context. Further, it enhances HIV prevention and treatment counseling and supports improved primary care in general.
The authors have not declared any conflicts of interests.
REFERENCES
|
Basile KC, Hertz MF, Black SE (2007). Intimate partner violence and sexual violence victimization assessment instruments for use in healthcare settings. Version 1.
|
|
|
|
Binfa EL, Cancino V, Ugarte I, Mella Guzmán M, Cavada Chacón G (2018). Adaptación del instrumento WAST para la detección de violencia doméstica en Centros de Salud.
Crossref
|
|
|
|
|
Brown JB, Lent B, Brett PJ, Sas G, Pederson LL (1996). Development of the Woman Abuse Screening Tool for use in family practice. Family Medicine-Kansas City 28:422-428.
|
|
|
|
|
Brown JB, Lent B, Schmidt G, Sas G (2000). Application of the Woman Abuse Screening Tool (WAST) and WAST-short in the family practice setting. Journal of Family Practice 49(10):896-903.
Crossref
|
|
|
|
|
Fogarty CT, Brown JB (2002). Screening for abuse in Spanish-speaking women. The Journal of the American Board of Family Practice 15(2):101-111.
|
|
|
|
|
DeVellis RF, Thorpe CT (2021). Scale development: Theory and applications. Sage publications.
|
|
|
|
|
Eluf-Neto J, Wünsch-Filho V (2000). Is screening good for your health?. Journal of the Brazilian Medical Association 46(4):310-311.
Crossref
|
|
|
|
|
García-Moreno C, Jansen HA, Ellsberg M, Heise L, Watts C (2005). WHO multi-country study on women's health and domestic violence against women. World Health Organization.
Crossref
|
|
|
|
|
Harvey A, Garcia-Moreno C, Butchart A (2007). Primary prevention of intimate partner violence and sexual violence: Background paper for WHO expert meeting May 2-3, 2007. Geneva: World Health Organization, Department of Violence and Injuy Prevention and Disability.
|
|
|
|
|
Herdman M, Fox-Rushby J, Badia X (1998). A model of equivalence in the cultural adaptation of HRQoL instruments: the universalist approach. Quality of Life Research 7(4):323-335.
Crossref
|
|
|
|
|
Iskandar L, Braun KL, Katz AR (2015). Testing the woman abuse screening tool to identify intimate partner violence in Indonesia. Journal of Interpersonal Violence 30(7):1208-1225.
Crossref
|
|
|
|
|
Jewkes R, Levin J, Penn-Kekana L (2002). Risk factors for domestic violence: findings from a South African cross-sectional study. Social Science and Medicine 55(9):1603-1617.
Crossref
|
|
|
|
|
Moraes CL, Hasselmann MH, Reichenheim ME (2002). Cross-cultural adaptation to Portuguese of the instrument "Revised Conflict Tactics Scales (CTS2)" used to identify violence between couples. Public Health Notebooks 218:163-176.
Crossref
|
|
|
|
|
Nelson HD, Bougatsos C, Blazina I (2012). Screening women for intimate partner violence: a systematic review to update the US Preventive Services Task Force recommendation. Annals of Internal Medicine 156(11):796-808.
Crossref
|
|
|
|
|
Osório C, Macuácua E (2013). The initiation rites in the current context. Maria José Arthur.
|
|
|
|
|
Qin S, Nelson L, McLeod L, Eremenco S, Coons SJ (2019). Assessing test-retest reliability of patient-reported outcome measures using intraclass correlation coefficients: recommendations for selecting and documenting the analytical formula. Quality of Life Research 28(4):1029-1033.
Crossref
|
|
|
|
|
Rabin RF, Jennings JM, Campbell JC, Bair-Merritt MH (2009). Intimate partner violence screening tools: a systematic review. American Journal of Preventive Medicine 36(5):439-445.
Crossref
|
|
|
|
|
Reichenheim ME, Moraes CL, Hasselmann MH (2000). Semantic equivalence of the Portuguese version of the Abuse Assessment Screen instrument to track violence against pregnant women. Journal of Public Health 34(6):610-616.
Crossref
|
|
|
|
|
Salahi B, Mohammad-Alizadeh-Charandabi S, Ranjbar F, Sattarzadeh-Jahdi N, Abdollahi S, Nikan F, Alizadeh-Asl R (2018). Psychometric characteristics of an intimate partner violence screening tool in women with mental disorders. International Journal of Women's Health and Reproduction Sciences 6:204-210.
Crossref
|
|
|
|
|
Sprague S, Madden K, Simunovic N, Godin K, Pham NK, Bhandari M, Goslings JC (2012). Barriers to screening for intimate partner violence. Women and Health 52(6):587-605.
Crossref
|
|
|
|
|
Todahl J, Walters E (2011). Universal screening for intimate partner violence: A systematic review. Journal of Marital and Family Therapy 37(3):355-369.
Crossref
|
|
|
|
|
World Health Organization (WHO) (2013). Responding to intimate partner violence and sexual violence against women: WHO clinical and policy guidelines. Geneva: World Health Organization.
|
|
|
|
|
World Health Organization (WHO) (2017). Violence against women and HIV/AIDS: Critical intersections. Geneva: World Health Organization.
|
|
|
|
|
Li YC, Li Y, Marshall CM, Rees HC, Nunez A, Ezeanolue EE, Ehiri JE (2014). Intimate partner violence and HIV infection among women: a systematic review and meta?analysis. Journal of the international AIDS Society 17(1):18845.
Crossref
|
|
|
|
|
Zacarias AE (2012). Women as victims and perpetrators of intimate partner violence (IPV) in Maputo city, Mozambique: Occurence, nature and effects. Inst för folkhälsovetenskap/Dept of Public Health Sciences.
|
|