Full Length Research Paper

ABSTRACT
This study focuses on testing the efficacy of herbal remedy used in many homes within the South-Eastern part of Nigeria to treat malaria and also the histopathological effect of the remedy on albino rats. Twenty rats were procured and distributed with five rats to one group. Group 1 received Garcinia kola and Aloe vera extracts, Group 2 received only G. kola extract, Group 3 is negative control and Group 4 is positive control. The treatment lasted for 21 days but parameters were monitored on day zero, second, third, fourth and 21st day. There was a sharp weight reduction of the albino rats at the third day, Group 1 recorded 107.21±15.46 as compared to the initial weight which was 116.18±14.94, but later increased at day 21. The weights across the groups at day three was statistically significant (p<0.05). The rats treated with G. kola extract recorded parasite density of 3997.34±0.00 at day 21 while the group 1 had zero parasite density at day 21. This shows that G. kola extract when used with Aloe vera extract will be more effective in the treatment of malaria as to compare when used alone. Histopathological test revealed no features of acute or chronic damage, but more studies are needed.
Key words: Malaria, Plasmodium falciparum, histopathology, Garcinia kola, Aloe vera extracts
INTRODUCTION
Malaria is one of the major public health problems especially in Africa and many other poorly developed countries. Malaria affect all ages but very lethal to children under the age of five and pregnant women. It is caused through a bite of the female anopheles mosquito, known to bite mostly during the evening time into the night. The mosquito habours in its gut and saliva the sporozoites of the parasite which cause malaria. Plasmodium, a known genus of the parasite that cause malaria is of five species; Plasmodium falciparum, Plasmodium vivax, Plasmodium ovale, Plasmodium malariae and Plasmodium knowlesi. Of these, P. falciparum happen to be the most deadly and common to the tropical region of the world (Hay et al., 2004). It has been noted that malaria causes over one million deaths per year globally but especially in African countries (Rowe et al., 2006). The parasite attack the red blood cells and individuals present with symptoms like high fever, nausea, chills, weakness, headache etc. at this point laboratory diagnosis are advised to confirm the presence of the parasite in blood sample and medications are administered, if this is not done with the correct drug and dosage, death may be the outcome. Over the years, several medications have been used in the treatment of malaria but along the line, resistance set it. Baird et al. (1996) stated that quinine from cinchona tree was used in the treatment of malaria in the early 1632 and this lead to the high cultivation of the tree throughout the world. Later, primaquine and quinacrine followed after the First World War, shortly after, chloroquine came in (Thompson and Werbel, 1972) and this drug was welcomed by many in Nigeria then for the treatment of malaria due to its cheap cost, but later resistance set it. This lead to further studies for proper treatment of malaria; it was as a result of the scientist unending efforts that another effective and latest drug in the fight against malaria emerged from a plant called Artemisia annua, this drug Artemisin was generally accepted (World Malaria Report, 2005) but expensive. In many under developed countries with Nigeria inclusive, many individuals depend on herbal concoctions for the treatment of so many illnesses with malaria inclusive. The term “herbal drug” is used for any plant or plant part that have been converted into phytopharmaceuticals by simple means of processes involving collection or harvesting, drying, storage, extraction of active components, purification of active components, etc. (EMEA, 2013). Nigerian pharmacy shops has a lot of antimalarial drugs but not really affordable by many artisans and so many of them depend on herbs for the treatment of malaria. Some of the plants used for treating malaria are bitter kola, Aloe vera, ginger, garlic, bitter leaf, Neem plant etc. The plants are either used alone or in combination with other plants. The botanical name of Aloe vera is Aloe Barbadensis Miller. It belongs to the Liliaceae family, which has about 360 species. The leaves are composed of three layers: An inner gel, a yellow sap and the outer thick layer of 15-20 cells called as rind. Aloe vera is known to contain anthraquinones and polysaccharides, which may act alone or in synergy (Surjushe et al., 2008). G. kola Heckel (Guttiferae) is a tropical plant whose seed is generally known as Bitter kola (Nwaokori et al., 2010). In Nigeria it is commonly called “Namiji goro” in Hausa, “Aki-inu” in Igbo and “orogbo” in Yoruba (Ndukwe et al., 2005). The plant has been referred to as a “wonder plant” because every part of it has been found to be of medicinal importance (Adegboye et al., 2008). Many of the herb users do not know much about the effectiveness or side effect of the plants they use in treating malaria and since the foreign plants have been investigated and now welcomed by the world in the treatment against malaria disease, why can’t our local plants be investigated as well. This particular study therefore sets out to know the effectiveness and side effect on liver of two plants (bitter kola and Aloe vera) used in the treatment of malaria disease.
MATERIALS AND METHODS
Study site and design
This project work was conducted at the animal farm of Godfrey Okoye University, Thinkers corner, Enugu state. The albino mice used in this study were obtained from the institution’s animal farm. The ethical guidelines stated and approved by the University for the use of laboratory animals were strictly followed all through the study. This study lasted for 21 days, during which several tests listed below were carried out at different time intervals.
Acclimatization period
The laboratory animals used were albino rats (20). Five rats per group were used in this study. Group 1 received G. kola and Aloe vera extracts; Group 2-received only G. kola extract, Group 3-is a negative control not infected with the parasite and not given any medication, the negative control groups were fed with the normal feed while Group 4- is positive control of which the rats were administered an orthodox malaria drug (pAlaxin). Acclimatization was done for a week accompanied with it was daily feeding and keeping of the environment clean.
Plant samples collection
The plants (G. kola and Aloe vera) used in this study were collected late February 2019, the samples were well stored to maintain their freshness and were used in March 2019 for the study.
Weight measurement
After the period of acclimatization, the rats were weighed before any herbal administration was started. The weights were also used for calculation of the herbal dose to be administered to each of the rats. The weight of the rats was checked.
Body temperature
The body temperature of each individual rat was checked using a thermometer; the temperatures were carried out prior to the research, second day and the twenty first day.
Blood sample collection
Blood samples were collected from individual rat before any injection of the blood sample known to contain the parasite of interest, during treatment and at 21st day. This research study was done in March 2019; the whole thing was wrapped off within three months. The rats were anesthetized with the use of chloroform soaked in a cotton wool. The soaked cotton wool was put into a mini bucket alongside the albino rat. They were left in the mini bucket containing the cotton wool soaked with chloroform for 20 s to inhale the chloroform, after which the syringe was pierced through the chest region to the heart from which the blood was collected. The blood collected was transferred into an EDTA bottle to avoid clotting. This was done for each rat anytime blood sample is needed.
Malaria microscopy and full blood count
For each rat, two thin blood films were made on a grease free labeled slide and stained using different stains; one of the thin films was for malaria microscopy and the other for full blood count. The thin films were made with five microliters of the blood sample. The thin films were air dried and fixed with methanol. A thick film was also made for parasitemia enumeration with 10 µl of the blood sample. One of the thin films and the thick film were stained with the Giemsa stain for 30 min, washed off with distilled water and allowed to dry. It was viewed under oil immersion. Parasite density was calculated using the following formula for all cases of malaria microscopy (WHO, 2010):

The other thin film was stained with leishman stain for 30 min and viewed under oil immersion as well. Malaria microscopy was carried out on the infected blood sample to be injected into the rats to confirm the presence of Plasmodium falciparum. The procedure stated above was adopted. Three milliliter of the confirmed infected blood was injected using the intraperitoneal method. After injection the site of administration was massaged for 5 s. The same volume of antigen was given across border. This was done for the entire rat except the negative control group. After 72 h of administration, their temperatures were checked under normal room temperature using the digital thermometer. Samples were collected after anesthetizing the rats with the chloroform to confirm the presence of the P. falciparum before beginning the treatment.
Preparation of extracts
The method of Matotoka and Masoko (2018) was followed in the preparation of the herbal concoction with some modifications. Briefly, the plants for the treatment which are G. kola and Aloe vera were collected and identified by a taxonomist from University of Nigeria, Nsukka, Enugu State. These plants were cleaned and washed with clean water. Aloe vera (39.00 g) and 60.00 g of G. kola were sliced and put into a 75 ml sterile bottle and this was labeled Group 1, warm water was added to the container. A different 60 g of G. kola was put into a separate 75 ml sterile bottle and was labeled Group 2, warm water was added as well. The container labeled Group 1 and 2 were left for 24 h before administration. A tablet of orthodox drugs (P-alaxin) was dissolved in 10 ml of distilled water in a sterile bottle labeled positive group.
Dosage of extracts administered
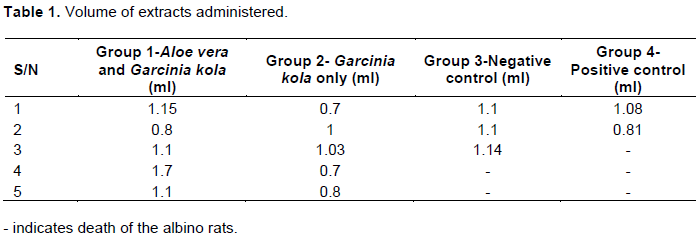
The extracts administered were based on the rats’ body weight calculation. The extracts were administered once daily. The rats were marked on their bodies to help differentiate them. During the period of acclimatization, some rats died and are indicated in the Table 1 with a hyphen.
Histopathological test
From each group one albino rat was dissected for the histopathological analysis of the liver. The albino rat was anesthetized and it was placed on a dissection tray. A dissection blade was used to dissect the rat vertically and the liver was located in the right upper quadrant of the abdomen, beneath the diaphragm. The liver was caught out and put into a sterile bottle containing formalin for preservation.
Statistical analysis
The average of the temperature, weight, packed cell volume and full packed count were calculated. All of the measured data were presented in the mean±standard error of mean. ANOVA was used to compare the means of the single factors different levels. Less significant difference (LSD) was used to compare the mean pairwise of the multiple factor different levels. All of the above statistical analyses were completed using the statistical software version 23.
RESULTS AND DISCUSSION
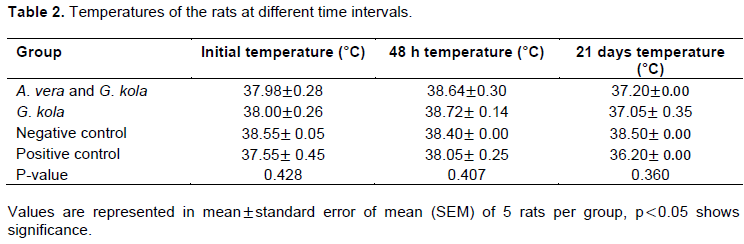
There is a sharp rise in the temperature of the experimental animals at 48 h from the initial temperatures as shown in Table 2 below. Although, the temperature of the negative control is seen to be high all through, but that of 48 h is lower than the initial temperature which brings us to say that it could be the normal temperature of the animal. The standard error of mean of Groups 1, 3 and 4 all through the tables except for the parasite density cannot be computed because some of the rats died leaving not enough data for the analysis. There was no significant change in the temperature of the laboratory rats (p>0.05).
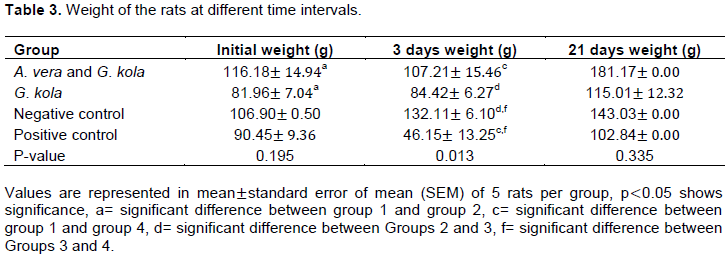
The combined medication of Aloe vera and G. kola extracts given to the laboratory animals reduced the weight of the animals by 8.97 g which canbe seen in Table 3, but later increased. That of the positive control was drastically reduced by 44.3 g why that of the negative control presented with no reduction in weight, instead there is a steady increase in their weights. These changes witnessed in their weights could be from the medications, the Group 2 with just G. kola extract witnessed no reduction in their weights. The weight gain seen with the group treated with only G. kola extract in this study is similar to that of the study carried out by Airaodion et al. (2020), who treated Plasmodium berghei infected rats with ethanolic extract of G. kola seed. There is statistical difference between their weights at third day.
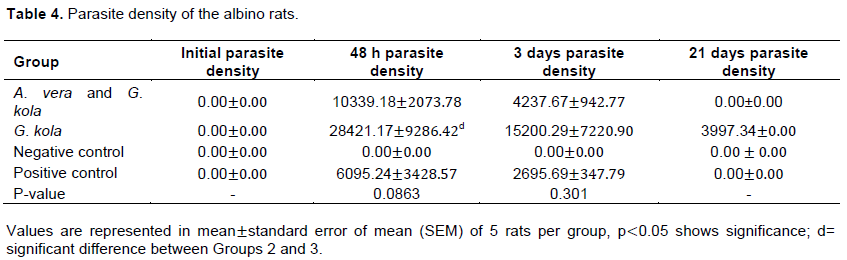
Parasite density shows the extent of the infection, efficiency of any medication against malaria parasite is proven once the medication is able to clear the parasite, hence the importance of determining parasite density. This was determined using WHO standard. All through the rats recorded zero parasite density initially but at day 2, there was a sharp rise in the parasite density which reduced at day three and none was recorded at the 21st day except for the group treated with only G. kola extract. Table 4 displayed the parasite density of the rats represented in mean±standard error of mean. The negative control had no parasite all through. The work of Damian et al. (2017) noted a drastic reduction in the percentage parasitemia of the mice used their study targeted against P. berghei when treated with G. kola.
Full blood count of the albino rats
Koshy et al. (2001) reported that anaemia is one of the clinical manifestations of malaria in mice, hence the need to carry out full blood count. These blood cells help in the fight against antigens. Reduced number of them always connotes the intensity of infection and will be high in immunocompromised or immunosuppressed individuals.
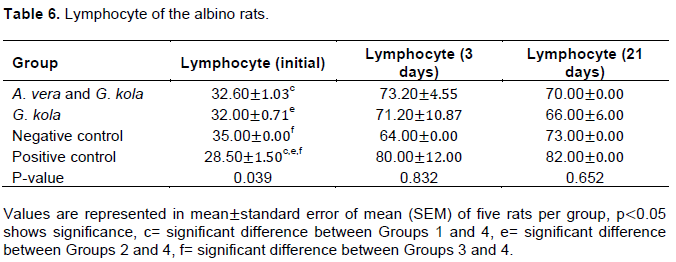
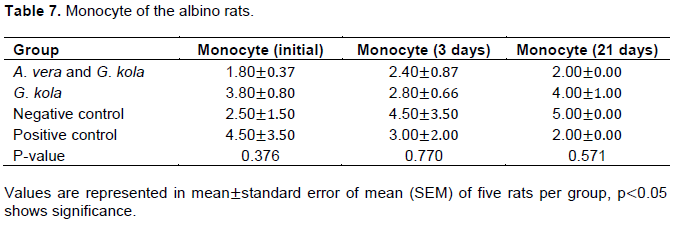
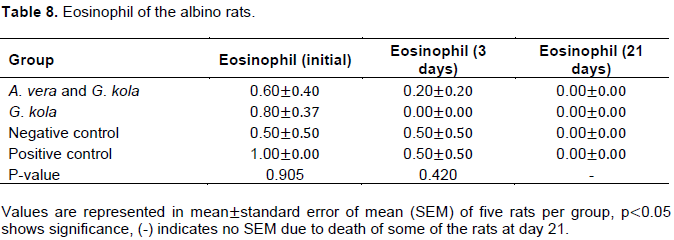
Tables 5 to 8 provide the results of the full blood counts carried out to determine the rate at which the immune system was responding to the infection.
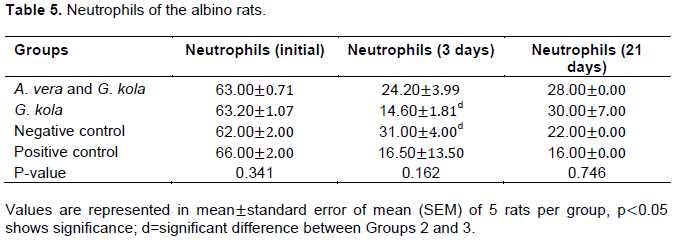
The work of Adaramoye et al. (2014) recorded that kolaviron, a biflavonoid from G. kola seeds has high antimalarial activities against P. berghei another parasite that causes malaria, when they tested the efficacy of the kolaviron on mice. That same study also witnessed an improvement in the packed cell volume of the groups treated with kolaviron and chloroquine which was statistically significant (p<0.05).
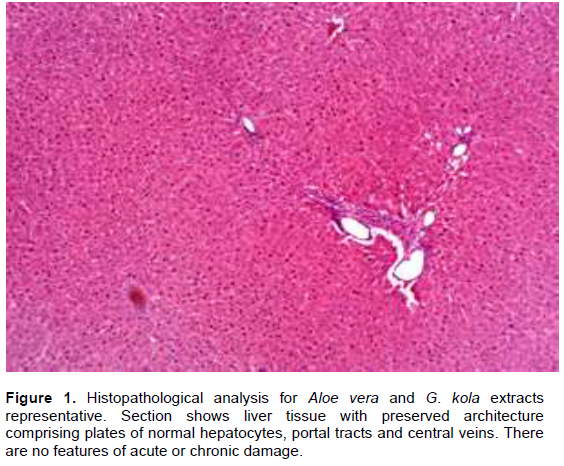
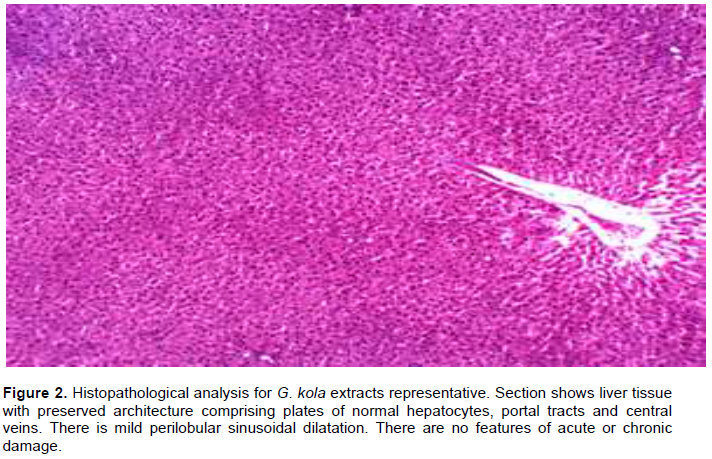
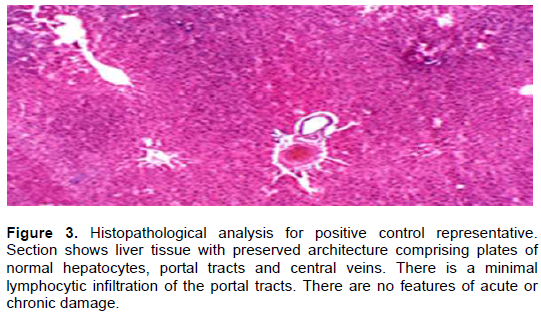
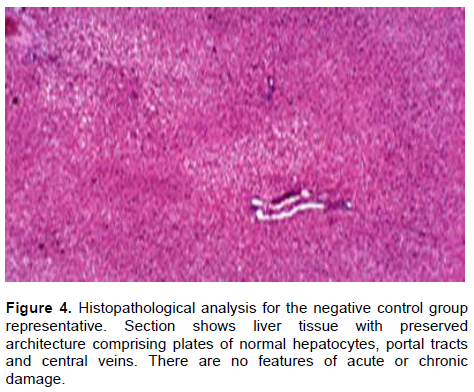
Histopathological analysis
The Figures 1 to 4 show the various effect of the extract on the liver of a representative rat from each group
CONCLUSION
This study has provided information on the use of the said plants as another alternative to the treatment of malaria infection, although longer days of treatment are required. The results gotten from the study are not so wonderful when compared to orthodox medicine but very promising and can be used to treat malaria. This medication is used by many people within villages in Nigeria without the reach of orthodox medicine. Therefore further identification and purification of the active components of these plants are needed. The side effect of the medication should be determined as well.
CONFLICT OF INTERESTS
The authors hereby declare that they do not have any conflict of interest.
REFERENCES
|
Adaramoye O, Akinpelu T, Kosoko A, Okorie P, Kehinde A, Falade C, Ademowo O (2014). Antimalarial potential of kolaviron, a biflavonoid from Garcinia kola seeds against Plasmodium berghei infection in Swiss albino mice. Asian Pacific Journal of Tropical Medicine 7(2):97-104. |
|
|
Adegboye MF, Akinpelu DA, Okoh AI (2008). The bioactive and phytochemical properties of Garcinia kola (Heckel) seed extract on some pathogens. African Journal of Biotechnology 7(21):3934-3938. |
|
|
Airaodion AI, Ekenjoku JA, Ngwogu KO, Ngwogu AC (2020). Ethanolic extract of Garcinia kola (Heckel) seed possesses antiplasmodialproperties against Plasmodium berghei. Asian Journal of Medical Principles and Clinical Practice 3(1):33-39. |
|
|
Baird JK, Caneta-Miguel E, Masba S, Bustos DG, Abrenica JA, Layawen AV, Calulut JM, Leksana B, Wignall FS (1996). Survey of resistance to chloroquine of falciparum and vivax malaria in Palawan, The Philippines. Transactions of the Royal society of Tropical Medical Hygiene 90:413-414. |
|
|
Damian DC, Nweze EI, Onyeke CC (2017). The In vivo anti-plasmodium activity of Garcinia kola Heckel. Journal of BasicPharmacology and Toxicology 1(2):27-31. |
|
|
European Medicine Agency (EMEA) (2013). Quality of Herbal Medicinal Products. Guidelines. European Agency for the Evaluation of Medicinal Products (EMEA), London. |
|
|
Hay SI, Guerra CA, Tatem AJ, Noor AM, Snow RW (2004). The global distribution and population at risk of malaria: past, present and future. Lancet Infectious Diseases 4:327-336. |
|
|
Koshy AS, Anila L, Vijayalakshmi NR (2001). Flavonoids from Garcinia cambogia lower lipid levels in hypercholesterolemic rats. Food and Chemical Toxicology 72(3):289-294. |
|
|
Matotoka MM, Masoko P (2018). Phytochemical screening and pharmacological evaluation of herbal concoctions sold at Ga Maja Limpopo Province. South African Journal of Botany 117:1-10 |
|
|
Ndukwe KC, Okeke IN, Lamikanra A, Adesina SK, Aboderin OJ (2005). Antibacterial activities of aqueous extracts of selected chewing sticks. Journal of Contemporary Dental Practice 6(3):86-94. |
|
|
Nwaokorie, F., Coker, A., Akitoye, C. Folasade, O., Gaetti-Jardim, E., Oyedele, G., Ayanbadejo, P., Abdurrazag, T. and Umezudike, A. (2010). Antimicrobial activity of Garcinia kola on oral Fusobacterium nucleatum and biofilm. African Journal of Microbiological Research, 4(7):509- 514. |
|
|
Rowe AK, Rowe SY, Snow RW, Korenromp EL, Armstrong JR, Stein C, Nahlen BL, Bryce J, Black R, Steketee RW (2006). The burden of malaria mortality among African children in the year 2000. International Journal of Epidemiology 35(3):691-704. |
|
|
Surjushe A, Vasani R, Saple DG (2008). Aloe vera: A short review. Indian Journal of Dermatology 53(4):163-166. |
|
|
Thompson PE, Werbel LM (1972). Antimalarial agents: chemistry and pharmacology. In: de Stevens G, editor. Medicinal chemistry, Academic Press, Inc. New York |
|
|
World Health Organization (2010). Basic malaria microscopy: part I. Learner's guide, second edition, WHO Press, World Health Organization, Geneva, Switzerland P 75. |
|
|
World Malaria Report (2005). Information available to WHO and UNICEF at the end of 2004. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


