Full Length Research Paper
ABSTRACT
The problem of lack of nurses can be solved by employing student nurses. Obviously, nurse instructors and preceptors have to work extremely hard to train student nurses to meet the standard of nursing. The preceptorship model is yet to be explored as to what it means to have an effective program or the requisite skills to be an effective preceptor. The purpose of this study is to explore how competencies and learning methods can improve nurse preceptors. The objectives of this study are to (1) identify the components of nurse preceptors’ competency and their indicators, (2) determine learning method applicable to program development of qualified preceptors, (3) obtain empirical evidence of the degree of the importance of the competencies and indicators to the constituents associated with program development of qualified preceptors. This study is a descriptive survey design. A purposive literature review identified 7 relevant preceptors’ competencies and 23 indicators. A total of 291 nurses volunteered to complete a questionnaire, indicating support of the desired competencies and preferred learning methods. Findings provide a competency-based model for program development to train nursing student preceptors in Thailand.
Key words: Competency, nurse preceptors, indicators, program development.
INTRODUCTION
There is inadequate number of nurses. This problem will be solved with the employment of student nurses (Srisuphan and Sweangdee, 2012; American Association of Colleges of Nursing, 2014). The preceptorship model bridges the gap between the classroom and clinical area where professional nursing is practiced (Flynn and Stack, 2006). A preceptor is both a clinical teacher and a practicing nurse in a work setting; he/she guides nursing students (or new graduates) in learning how to apply theoretical knowledge. A nurse preceptor is important in the education and socialization process of nursing students (Ousey, 2009). A preceptor’s teaching and clinical competencies impact the professional develop-ment of nursing students (Spouse, 2001; Zilembo and Monterosso, 2008). Although many nurses have excellent clinical skills, their roles in teaching students are less refined. Therefore, it is essential to have nursing preceptors’ programs that strengthen their teaching competencies (Punyathorn, 2009). Nurse preceptors have many roles in their work settingin addition to teaching students. It is quite understood that their didactic skills need to be sharpened as they teach during student nurses’ clinical practice. Nurses need to develop a preceptor’s program to improve the required attributes of preceptors. However, to improve or develop a preceptor’s program, a thorough assessment is necessary to understand all the attributes that are needed for the role. In Thailand, as in other countries, the nursing preceptorship model is in use, but is yet to be explored. It would be useful to understand if there are characteristics of an effective preceptor’s program and a set of competencies needed to be an effective preceptor.
The Thailand Nursing and Midwifery Council provides the standards expected of qualified nurse preceptors in hospitals and a curriculum for training them (Thailand Nursingand Midwifery Council, 2014). The training for preparing these special instructors is available in multiple educational venues throughout Thailand. However, the immediate needs of individual hospitals for qualified preceptors to attend may exceed the capacity of what the training sessions can provide logistically. Furthermore, hospital constituents interested in preceptors’ training may wish to enhance certain aspects of their curriculum and include a variety of learning activities relevant to the contextual needs of their particular circumstances for nurses and nursing students. To do so, there is need for a systematic approach to identify the components associated with the competencies of a qualified nurse preceptor. In addition, evidence is needed from the stakeholders involved in preparing preceptors (i.e., nursing students preceptors, administering preceptor training, and the preceptors themselves) to identify desired curricular enhancements.
Statement of the problem
Preceptor nurses are both clinical teachers and practicing nurses. They guide nursing students and impart them with theoretical knowledge. Preceptors play vital role the education of nursing students. Although many nurses have excellent clinical skills, their roles as teachers are less refined; their competencies are questionable. Hence, it is vital for them to be trained using methods and programs that would strengthen their teaching competencies.
REVIEW OF RELEVANT LITERATURE
Identification of preceptors’ competencies and indicators
The literature was reviewed purposively to identify components of preceptors’ competency. Twelve sources addressed a total of 22 components. The number of components mentioned by individual sources/authors ranged from 1 to 9; that is, one source may identify only one component related to competency whereas another source may address nine components. After examining the similarities and differences between the 12 sources, seven major components were selected as relevant to this study. The criterion to accept the components was based on whether they were mentioned four or more times in the literature. Three additional components were selected because the American Nurses Association includes them as part of the role of preceptors (Ulrich, 2012). These three were combined with the seven identified components.
The component most frequently mentioned was teaching-learning (Cooper and Palmer, 2000; Dawudom, 2007; Fawcett, 2002; Freeman, 2004 cited in Barker, 2006; Gray and Smith, 2000; Perrone-Ambrose Associates, 2007; Nursing and Midwifery Council (United Kingdom; NMC-UK), 2008; Pasasawat and Srisathitnarakul, 2011; Ulrich, 2012), followed by being supportive of students’ learning (Canadian Nurses’ Association, 2004; Cooper and Palmer, 2000; Dracup and Bryan-Brown, 2004; Fawcett, 2002; Pasasawat and Srisathitnarakul, 2011; Perrone-Ambrose Associates, 2007; NMC-UK, 2008; Ulrich, 2012).
The third most mentioned component was clinical nursing expertise (Cooper and Palmer, 2000; Dawudom, 2007; Fawcett, 2002; Freeman, 2004 cited in Barker, 2006; Gray and Smith, 2000; NMC, 2008; Pasasawat and Srisathitnarakul, 2011; Perrone-Ambrose Associates, 2007). Two components taking fourth and fifth place were ability to communicate and establish relationship (Dawudom, 2007; Dracup and Bryan-Brown, 2004; Freeman 2004 cited in Barker, 2006; NMC, 2008; Pasasawat and Srisathitnarakul, 2011; Swihart et al., 2007) and role modeling (Cooper and Palmer, 2000; Fawcett, 2002; Gray and Smith, 2000; Ulrich, 2012).
Lastly, two components in the sixth and seventh place were: being accessible for consultation (Cooper and Palmer, 2000; Dawudom, 2007; Fawcett, 2002; Pasasawat and Srisathitnarakul, 2011) and leadership (NMC-UK, 2008; Pasasawat and Srisathitnarakul, 2011; Swihart et al., 2007; Ulrich, 2012). Because of their importance, three additional components were included but combined with the seven components: Risk management with leadership; ethics with role modeling; measurement, feedback, and evaluation with teaching.
Criteria for selecting indicators
An additional 13 sources identified 111 indicators of preceptors’ competency based on the seven afore-mentioned components. The criteria for selecting 23 of the 111 indicators varied for each component as mentioned in the literature.
1. Teaching-learning: giving constructive feedback, evaluation (Boonnoon, 2002; Downudom, 2007; Joyce, 1996; Cooper and Palmer, 2000; Sutachai, 2012), appropriate teaching method (Joyce, 1996; Dowudom, 2007; Cooper and Palmer, 2000; Sutachi, 2012), and individualized teaching (Boonnoon, 2002; Dowudom, 2007; Joyce, 1996; -Cooper and Palmer, 2000).
2. Being supportive of students’ learning: Identifying preferred knowledge source, helping students to adapt, and cooperation between nursing students, institutions, and hospitals (Boonnoon, 2002; Komaratat, 2007).
3. Clinical nursing expertise: Using nursing process and clinical experts (Dowdom, 2007; Public Health Nursing Division, 1996), appropriate diagnoses and intervention (Myrick and Barrett, 1992; Dowudom, 2007).
4. Communication and relationship: Effective communi-cation (Dowdom, 2007; Public Health Nursing Division, 1996; Pasasawat and Srisathitnarakul, 2011; Sullivan and Decker, 1992), effective relationships (Boonyanurak, 1995; Cooper & Palmer, 2000; Sullivan & Decker, 1992; Sutachai, 2012), and clear expression of words (Dowudom, 2007; Public Health Nursing Division, 1996; Sullivan and Decker, 1992).
5. Role model and ethics: Enthusiastic, positive attitude, making impression, and ethical behavior (Boonnoon, 2002; Suriyawan, 1990).
6. Consultant: Analyzing needs of new nurses (Boonnoon, 2002; Dowudom, 2007; Cooper and Palmer, 2000; Sutachai, 2012), using reflection to show empathy, and being able to give counsel (Boonnoon, 2002; Dowudom, 2007; Sutachai, 2012)
7. Leadership: Resolving problems (Ratanaruengwatana et al., 2000; Shamian and Inhaber, 1985; Suriyawan, 1990; Sutachai, 2012), time management skills (Sa-nguansiritum, 1992; Shamian and Inhaber, 1985; Suriyawan, 1990; Sutachai, 2012), being able to give inspiration (Suriyawan, 1990; Rattanaruangwattana et al., 2000; Dowudom, 2007), and fighting for human rights (Dowudom, 2007; Rattanaruangwattana et al., 2000; Sutachai, 2012).
Identification of learning methods
The literature was further reviewed purposively to determine learning methods for educational development. Five sources identified 32 learning methods. The number of methods mentioned by individual sources/authors ranged from one to five. After examining the similarities and differences between the five sources, 10 relevant methods were selected for further examination. The criterion for accepting the learning methods was based on whether they were mentioned in the five sources, at least two or more times. The learning method most frequently mentioned was classroom training (Bangmo, 2004; European Federation of National Engineering Association [FEANI], 2013; Kityunyong and N-Taguatung, 1996; Office of Human Resource Management (OHRM), 2010; National Science and Technology Development (NSTDA), 2007), followed by on-the-job training (OHRM), 2010; Kityunyong and N-Taguatung, 1996; NSTDA, 2007; OHRM, 2010).
Four methods ranked third, fourth, fifth, and sixth are: site visits (Bangmo, 2004; NSTDA, 2007; OHRM, 2010), lecture, brainstorming, group discussion (Bangmo, 2004; FEANI, 2013; OHRM, 2010). The followings were mentioned twice: case study (Bangmo, 2004; FEANI, 2013), self-study/e-learning, learning through reflection, and network learning/sharing experiences (Kityunyong and N-Taguatung, 1996; FEANI, 2013). Five additional activities mentioned twice were eliminated because they were deemed impractical styles for gaining role compe-tencies as nurse preceptors (e.g., project assignment, continuing education).
METHOD
Research design
A descriptive survey design was used to obtain information on how competencies, indicators of competencies and learning methods would improve nursing student preceptors. Literature was reviewed purposively to identify the preceptors’ competency, indicators of competencies and learning methods. Stakeholders were asked of the requirements needed to provide the program. Participants responded to a paper-and-pencil questionnaire. The participants were anonymous to the researcher; no names appeared on the questionnaire and the participants’ responses are confidential. The research study was formally approved by the appropriate university Institutional Review Board (IRB) and one hospital ethics committee. Three hospitals and two colleges of nursing accepted the university IRB’s approval.
Sample and setting
The study was conducted in one of the 12 health regions in Thailand. The population included the academic directors of two nursing colleges, who have experience as nurse preceptors, nursing instructors who have experience in clinical teaching and nursing students who have experience being taught by nurse preceptors, the directors of nursing of four hospitals who have experience as nursing student preceptors and the preceptors in the hospitals appointed by nursing colleges. The total population was 1155. All participants less than 10 were selected while for those more than 10, 1:4 was selected. Two academic nursing directors and four directors of nursing were purposively sampled. Also, 255 of the nursing instructors and students were systematically sampled using every fourth name on a list generated by the two colleges. A convenience sample of 30 preceptors was identified by hospital administrators. All of the population was chosen equally and represented. The total sample was 291 participants. The sample size of 291 was based on the Krejcie and Morgan table (Sri Sa-ard, 2008) that allows for a 5% margin of error and 95% confidence. The survey return rate was 100%.
Measures
Based on the review of relevant literature, the researcher developedone questionnaire for all participants with specific directions for sections to complete. There was a set of items with 5-point Likert response options asking for opinions of agreement whether preceptors should possess the seven components of competency. Participants chose one of the following options: 1 = Strongly Disagree; 2 = Disagree; 3 = Neither Agree nor Disagree; 4 = Agree; 5 = Strongly Agree. In another set of items, participants were asked to respond to whether preceptors need development in each of the seven components of competency. They responded using the same 5-point Likert scale. Average level of agreement was calculated for each component.
On a grid listing the seven components of competencies (rows) and learning activities (columns), participants were asked of the required learning method needed to develop each competency. Participants could select more than one activity for each component. The number of selections tallied with each component to determine the overall preferred methods of learning.
Seven doctoral-prepared experts evaluated each item of the questionnaire for content validity using an index of congruence (Rovilnelli and Hambleton, 1977). Two experts had five years of experience working with preceptors, two had conducted research on competency development, two focused on curriculum development, and one focused on evaluation methods. The range of congruence for each item was from .60 to 1.0, with an average of .71, above the .50 minimum level of acceptance. A pilot study was conducted with nurse preceptors who had a similar nursing background. The Cronbach's alpha coefficient for internal consistency was 0.81.
Data analysis
All data were analyzed using IBM® SPSS® software version 16. Descriptive statistics were frequencies, percentages, means, and standard deviations.
RESULTS
Components of nursing student preceptors’ competency
In the respondents’ opinion, all seven components of nursing student preceptors’ competency are important and should be used (Table 1). Mean scores were high on the level of agreement, ranging from 4.3 to 4.5 on a 5-point scale with negligible variation across the components by standard deviation. Clinical nursing expertise had the highest level of agreement as a component of nursing student preceptors’ competency followed by teaching-learning, communication and relationship.
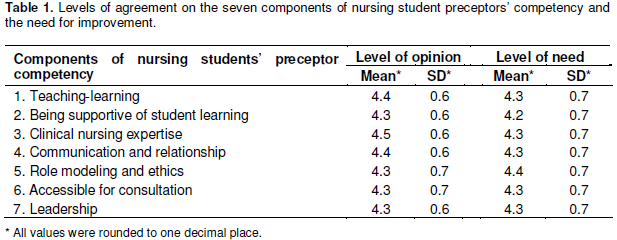
There were slight differences in the level of agreement on whether nursing student preceptors needed improvement in each of the seven components of preceptors’ competency. Mean scores on level of agreement ranged from 4.2 to 4.4 on a 5-point scale with no variation across the components (SD = 0.7). There was a small gap between the importance of clinical nursing expertise and whether there was a need for improvement. The highest need for improvement was for role modeling and ethics. The lowest was for being supportive of students’ learning.
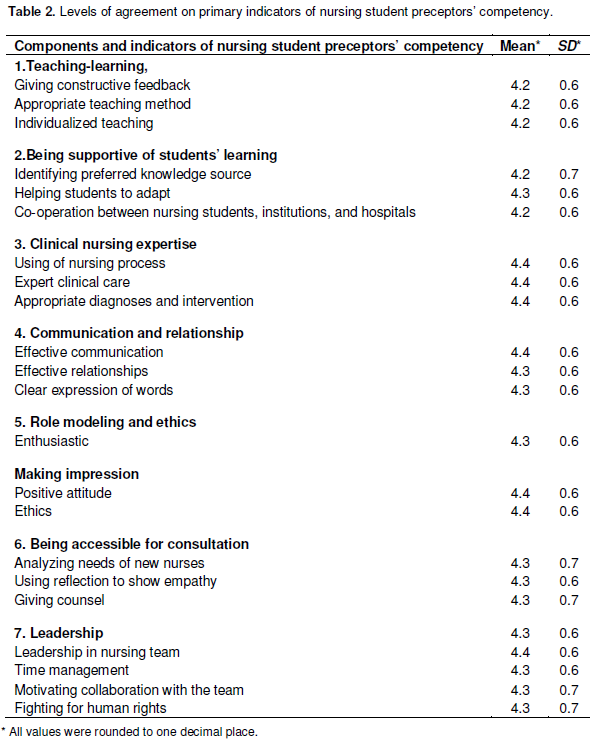
Indicators of nursing student preceptors’ competency
Respondents rated high the three indicators of competency for clinical nursing expertise (Table 2). This was followed by two indicators for role modeling and ethics: one indicator for communication and relationship and one indicator for leadership. Although considered a high level of agreement on 5-point response scale, the consistent lower levels of agreement were the three indicators for teaching-learning. This was followed by two indicators of being supportive of students’ learning.
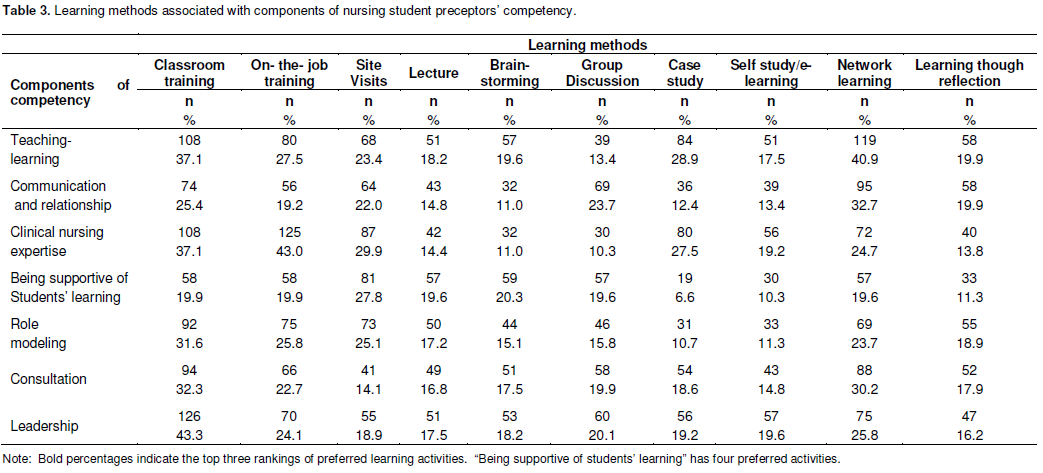
Learning methods related to nursing student preceptors’ competency
Participants were asked of the required learning methods needed to develop each competency. Participants identified the learning method they preferred for each of the seven components of nursing student preceptors’ competency (Table 3). Classroom training was identified in all of the seven components of nursing student preceptors’ competency as one of the top three learning methods. On-the-job training was in the top three learning methods out of the five components; network learning/ sharing experience was similarly ranked in four components. Site visiting was ranked in the top three learning methods of preferred learning for three components. Case study and group discussion were listed in the top three learning methods for a single component.
DISCUSSION
This research study explored how nursing students’ competencies and learning methods could provide guidance to those seeking how to educate nursing student preceptors by developing training programs. The study’s findings strongly support the seven components of nursing student preceptors’ competencies. The role of nursing student preceptors encompasses imparting knowledge and experiences by using appropriate teaching and learning methods. This requires leadership with nursing students, often in a consultative role. Nursing student preceptors should have clinical nursing expertise in their clinical practice to role model nursing skills to nursing students.
To develop a training program, educators recognize that the variety of possible learning methods makes it cumbersome to apply all possible methods for each competency. The findings show that the constituents surveyed in this study have preferences (Table 3). This may be a model for future program development. For example, learning method for preceptor trainees to achieve a competency in teaching and learning could include visiting a nursing college/school/ faculty to speak to instructors for shared experiences on how to teach and give constructive feedback. This would be by using network learning, site visits, and case studies. Classroom training would focus on the topic of education theories, learning styles of nursing students, and how to develop a lesson plan.
When deemed ready by a mentor, the preceptor trainee would move to on-the-job training with supervision in real situations and hospital setting. Indicators of knowledge acquisition by preceptor trainees could be assessed by using 15 to 20 multiple choice test items. The time allocated for learning methods may be judged subjectively based on the importance of selected contents and the logistical practicalities associated with the methods. Each developer of a program can judge the appropriateness of time and conduct formative and summative program evaluation which can bemodified for future programs.
In a similar manner, program developers can examine the desired learning activities for the remaining competencies by referencing Table 3. A trained observer would assess the trainees’ skills and attitudes by using a checklist during practice or simulation of giving constructive feedback and appropriate individualized teaching and role modeling. Other indicators of achievement could be the use of nursing process; the level of clinical nursing expertise in clinical care; the observed ability to solve problem and intervene effectively; the ability to identify a preferred knowledge source for information seeking (part of role modeling); assisting nursing students to adapt to a new situation; showing cooperation between institution, hospital, and nursing students. Other skills are the ability to analyze the needs of nursing students, using reflection to show empathy, ability to give wise counsel, effective time management. Giving impression to the students, displaying enthusiasm, showing a positive approach, showing leadership in the nursing team, motivating collaboration with the healthcare team, advocating for patients and human rights, and using ethical judgments are attitude indicators for assessment of role modeling and ethical behavior. A mentor can assess preceptor trainees’ knowledge by multiple choice test items, observation and checklists, and nursing students’ feedback. The use of dichotomous (yes-no) or 5 – 7 point Likert options of agreement can further assess levels of competency achievement.
A qualified nursing student preceptor can have a positive impact on nursing students during clinical practices (Carlson et al., 2009). The study’s findings strongly support the seven elements of nursing student preceptors’ competencies. The role of nursing student preceptors encompasses imparting knowledge and experiences by using appropriate teaching and learning methods. This requires leadership skills and a supportive relationship with students. Nursing student preceptors are to have clinical nursing expertise in their clinical nursing practice to teach clinical skills to students. This enables nursing students to learn how to apply those experiences from practice to real situations (Canadian Nurses Association, 2004; NMC-UK, 2008; Pasasawat and Srisathitnarakul, 2011). Creative competency is an effective method for maintaining and monitoring skill and attributes of people in an organization (Thompson, 2015).
Most nursing student preceptors undertake orientation for years and require more updated knowledge, as well as improved requisite. In the survey of the nursing student preceptors in Practicum Placements of Udornthani, 80.8% of participants showed the need to improve their competency (Punyathorn, 2009).
Developing the program for improving the competencies of nursing student preceptors entails obtaining data from opinion survey on the needs and development of preceptors’ competency from stakeholder groups based on the context of the nursing student preceptors. Each competency needs diverse methods for improvement. That means in one competency there are many methods to make the preceptors have knowledge skill and attributes in their job because they may have different learning styles and learning objectives.
CONCLUSION
The strength of studying competencies and learning activities to develop training programs to improve preceptors comes from an examination using actual constituents that would be most affected by the program. The program may be clinical and educational settings where there is an identified need.
Limitation of the study
It was difficult to search for data on specification of nursing student preceptors’ competency. New nurse preceptors’ competency was studied in this research
RECOMMENDATION FOR FUTURE RESEARCH
Further work should be on the effectiveness of nursing student preceptors’ competency indicators and program evaluation by comparing the effectiveness of each learning method or activity. The validity of the methods will change over time with technology advancements, and changes in life style.
CONFLICT OF INTERESTS
The authors have not declared any conflicts of interest.
REFERENCES
|
American Association of Colleges of Nursing (2014). Nursing shortage fact sheet. Washington, DC. |
||||
| Bangmo S (2004). Training and meetings (2nd ed.). Bangkok: June Publishing. | ||||
|
Barker ER (2006). Mentoring-A complex relationship. J. Am. Acad. Nurse Practitioners 18:56-61. Crossref |
||||
| Boonnoon A (2002). Preceptorship training program for staff nurses: A case study of Banmi hospital. J. Nurs. Sci. Chulalongkorn University 15(1):45-54. | ||||
| Boonyanurak P (1995). Strategies to create success in the practice of nursing . Journal of Faculty of Nursing Burapha University 2(2):14-24. | ||||
|
Carlson E, Wann HC, Pilhammar E (2009). Teaching during clinical practice: Strategies and techniques used by preceptors in nursing education. Nurse Educ. Today 29:522–526. Crossref |
||||
|
Canadian Nurses' Association. (2004). Promoting continuing competence for registered nurses. |
||||
| Cooper AM, Palmer A (2000). Mentoring, preceptorship and clinical supervision: A guide to professional roles in clinical practice. Wiley-Blackwell. | ||||
| Dawudom N (2007). The components of competency of mentors in nursing. J. Nursing Sci. Chulalongkorn University 21(1):50-63. | ||||
| Dracup K, Bryan-Brown C (2004). From novice to expert to mentor: Shaping the future. Am. J. Crit. Care 13:448-450. | ||||
|
European Federation of National Engineering Association. (2013). Management Training: How to Train Employees. |
||||
|
Fawcett D (2002). Monitoring what it is and how to make it work. Association of Post Operative Registered Nurses J. 75:950-954. Crossref |
||||
| Flynn JP, Stack M (2006). The role of the preceptor: A guide for nurse educators, clinicians and managers.New York: Springer. | ||||
|
Gray MA, Smith LN (2000). The qualities of an effective mentor from the student nurse's perspective: findings from a longitudinal qualitative study. J. Adv. Nurs. 32:1542-1549. Crossref |
||||
| Joyce B (1996). The coaching of teaching. Educational Leadership, 40(1):4-106. | ||||
| Kityunyong S, N-Taguatung O (1996). Technical training effectively (2nd ed.). (The new season). Bangkok: Se-education. | ||||
|
Komaratat S (2007). Effect of using mentorship model on nursing competency of new graduated nurses. J. Continuing Educ. Nurs. 40(10):475-480. Crossref3-02 |
||||
| Myrick F, Barrett C (1992). Preceptor selection criteria in Canadian basic baccalaureate school of nursing – A survey. Can. J. Nurs. Res. 24(3):53-68. | ||||
|
National Science and Technology Development (2007).Guide to develop the competency of staff. |
||||
|
Nursing and Midwifery Council (United Kingdom) (2008). Standards to support learning and assessment in practice. |
||||
|
Office of Human Resource Management (2010). UN competency development: A practical guide. United Nations Office of Management. |
||||
|
Ousey K (2009).Socialization of student nurses-the role of mentor. Learn. Health Soc. Care 8(3):175-184. Crossref |
||||
| Pasasawat O, Srisathitnarakul B (2011) A study of preceptor competency, tertiary hospital. J. Royal Thai Army Nurses 12(Special):21-27. | ||||
| Perrone-Ambrose Associates. (2007). A mentor's companion: Mentoring coaching consulting. | ||||
| Public Health Nursing Division, (1996). The roles and responsibilities of the nurse in the hospital. Ministry of Public Health. Bangkok: Thammasart University. | ||||
| Punyathorn K (2009). Problem and requirements of nursing preceptors in practicum placements ofUdornthaniCollege of Nursing. Northeast Med. Assoc. J. 27(3):57-65. | ||||
| Ratanaruengwatana S, Kanoksuntornrat N, Sirapongam Y (1998). New graduated nurse anxiety, general characteristics and clinical competencies of preceptors based on the graduates need. Ramathibodi Nurs. J. 4(2):120-132. | ||||
| Rovilnelli RJ, Hambleton RK (1997). On the use of content specialists in the assessment of criterion-referenced test item validity. Dutch J. Educ. Res. 2:49-60. | ||||
| Sa-nguansiritum U (1992).The development of the nursing profession. Chaingmai: Changpurg. | ||||
|
Shamian J, Inhaber R (1985). The concept and practice of preceptorship in contemporary nursing: A review of pertinent literature. Int. J. Nurs. Stud. 22(2):79-88. Crossref |
||||
|
Spouse J (2001). Bridging theory and practice in the supervisory relationship: A sociocultural perspective. J. Adv. Nurs. 33(4):512–522. Crossref |
||||
| Swihart D (2007). Nurse Preceptor Program Builder: Tools for a Successful Preceptor Program. HCPro. | ||||
| Srisuphan W, Sawaengdee K (2012). Recommended policy to resolve the shortage of nurses. Professions in Thailand. Thai J. Nurs. Council 27(1):5-12. | ||||
| Sri Sa-ard B (2008). Curriculum development and research. Bangkok: Suweriyasan Publishing. | ||||
| Srisathitnarakul B (2011).Leadership and management strategy nursing organization in the 21st century. Bangkok: Faculty of Nursing, Chulalongkorn University. | ||||
| Sullivan EJ, Decker PJ (1992). Effective management in nursing (3rd ed.). New York: Addison-Wesley. | ||||
|
Suriyawan B (1990). Effects of using preceptorship in the orientation program towards knowledge, attitudes, and skills for nursing practice of new graduate nurses. |
||||
|
Sutachai B (2012). Development of a competency framework of nurse preceptors.MaharajNakorn Chiang Mai Hospital. |
||||
|
Thailand Nursingand Midwifery Council (2014). Manual of certification Academy of Nursing and Midwifery,Nursing and Midwifery Council. |
||||
|
Thompson R (2015). Development a competency framework. |
||||
| Ulrich BT (2012). Mastering precepting: A nurse's handbook for success. Indianapolis: Sigma Theta Tau International. | ||||
|
Zilembo M, Monterosso L (2008). Towards a conceptual framework for preceptorship in the clinical education of undergraduate nursing students. Contemp. Nurse 30(1):89-94. Crossref |
||||
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


