Full Length Research Paper
ABSTRACT
The aim of this study is to present a new approach to sport medicine. Comparative analysis of the Vertebrae Lumbales was done in sedentary group and Muay Thai athletes. It was done by acquiring three dimensional (3-D) data and models through photogrammetric methods from the Multi-detector Computerized Tomography (MDCT) images of the Vertebrae Lumbales sections in male Muay Thai athletes and the sedentary (control) group. 5 male Muay Thai athletes and 5 male sedentary individuals from Ordu Province participated in this study. The Vertebrae Lumbales of 5 male Muay Thai athletes and 5 sedentary (control group) participants were scanned with high-resolution MDCT devices. The resulting 2-D axial images were transferred to CD-ROMs in DICOM format and then to a PC installed with 3D-Doctor 5.0, a three dimensional modeling software. Reconstruction of the data was conducted via the 3-D rendering component of this software. All measurements were automatically calculated via the aforementioned software and Mann Whitney-U test analysis technique. SPSS 15.0 statistical package programme was used for statistical analyses. The statistical results of the vertebrae lumbales showed significant differences (P<0.05) in L1 volume (mm3), in terms of statistical aspect, in both Muay Thai athletes and sedentary participants. Meanwhile, the biometric measurements showed a more significant deformation only in the L1 segment of the Vertebrae Lumbales. Consequently, it was expected that these kinds of researches will contribute to the development of infrastructure work to be conducted on Muay Thai athletes using the MDCT technique and to the appreciation of the need for the involvement of 3-D Reconstruction Procedures in Sports Medicine.
Key words: Sports medicine, athletes, three-dimensional reconstruction.
INTRODUCTION
The diagnosis and treatment of diseases in vertebrae lumbales has gained fairly new dimensions due to the advancements in the field of technology and the reflection of anatomic knowledge into clinic applications. Research on this field usually comprises regulations and implementation of national and international ethic rules whose scope gradually expands. Reducing the cadaver population to minimum levels, and promoting scientific data in training, instruction and academic studies are regarded as concepts that should not be ignored by anatomists. MDCT is an efficient diagnostic modality which produces two dimensional (2-D) multi-planar (horizontal, coronal, sagittal, axial etc.) images of the anatomic structure of bones and deformities (Hall, 1994). MDCT renders hundreds of 2-D multi-planar images in just seconds which may then be transformed into 3-D by means of computer software (Hu et al., 2000).
3-D geometric modeling has a widespread use in medical training along with plastic surgery, orthopedic surgery, traumatology, neurosurgical applications (Krupa et al., 2004).
Studies in the field of Muay Thai are mainly on injuries, injury rates, physiologic reactions, Muay Thai Time-Motion analysis etc. and rarely on biomechanical studies (Gartland et al., 2001; Antonio et al., 2009; Jeronimo et al., 2011).
Literature review indicates no prior study on detailed assessment and the 3-D reconstruction of CT images of Vertebrae Lumbales in Muay Thai athletes. The structure of the Vertebrae Lumbales sections acquired from sedentary group and Muay Thai Athletes by means of Multi-detector Computerized Tomography (MDCT) will be reconstructed in 3-D in order to assess the Vertebrae Lumbales of these two groups.
MATERIAL AND METHODS
This research was performed according to Declaration of Helsinki. In scope of the study, the Vertebrae Lumbales of 5 Muay Thai athletes and 5 sedentary (control group) participants were scanned in high-resolution (Somatom Sensation 64; Siemens Medical Solutions, Forchheim, Germany) MDCT diagnostic device.
The parameters of the MDCT device were set as follows: physical detector collimation at 32 x 0.6 mm; final section collimation at 64 x 0.6 mm; section thickness at 0.75 mm; gantry rotation timing at 330 msec; kVp at 120; mA at 300; resolution at 512 x 512 pixels; resolution spacing at 0.92 x 0.92. Dose parameters and scans were conducted based on standard protocols and literature (Prokop, 2003; Kalra et al., 2004). Scans of the control and experimental groups were conducted in supine position. The resulting 2-D axial images were transferred to CD-ROMs in DICOM format and then to a PC installed with 3D-Doctor 5.0 (Copyright© 1998-2013 Able Software Corp.), a three dimen-sional modeling software. During the segmentation process, the operational procedures applied by researchers (Bazille et al., 1994) were adopted. Table 1.

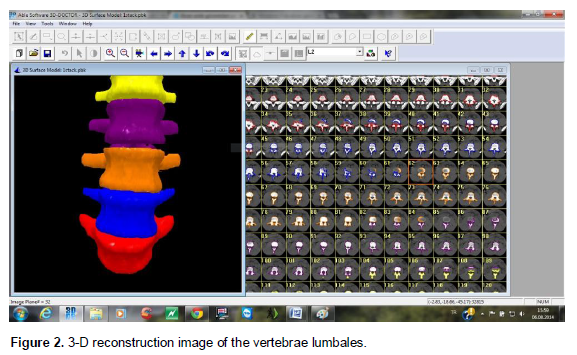
The resulting segmentation was called semi-automatic segmentation. Manual correction time took approximately 3 to 5 min / per section image. At the first phase of semi-automatic segmentation, the bone boundaries were structured automatically. After the automatic boundary segmentation; the spots, which were unable to be properly positioned on the bones, were manually corrected one by one with a PC mouse by means of interactive boundary editing routine (Figure 1). After the manual correction was checked, the corrected boundaries of the bone surface were overlapped with automatic ones. Reconstruction of the data was conducted via the 3-D rendering component of this software (Figure 2). The volume and surface area of vertebral bones composing the Vertebrae Lumbales were automatically measured by the 3-D software.

The statistical analyses were made via Mann Whitney-U test analysis technique in SPSS 15.0 statistical package programme. Statistical significance was recorded as P < 0.05.
Statistical analysis was carried out on the 3-D biometric values of the bones as reconstructed from the Muay Thai and sedentary groups. The results from the Vertebrae Lumbales showed considerable statistical significance (P<0.05) only on the volume of the Lumbales among the L1 vertebral bones in the Muay Thai and sedentary groups.
DISCUSSION
To date, various research on Muay Thai athletes is been conducted (Tony and Nigel, 2012; Tony et al., 2014; Barry, 2011). However, no prior study on detailed assessment and the 3-D reconstruction of CT images of Vertebrae Lumbales in Muay Thai athletes are available.
The results from the Vertebrae Lumbales showed considerable statistical significance (P<0.05) only on the volume (mm3) of the Lumbales among the L1 vertebral bones in the Muay Thai and sedentary groups. Baker and Patel (2005) informed that stress fractures and degenerative illnesses of spinal column caused waist aches. This indicates the importance of L1 value determination at this study. This assertion does not support the claims of Pettersson et al. (1998) that both muscular force and bone parameters would increase in sportsmen and those who exercise regularly. In a study conducted on elite Judo athletes and sedentary groups, Kalayc? (2008) stated that statistically the biometric rates of metacarpal and phalanges bones were larger in Judo athletes compared to sedentary group participants.
Meanwhile, all biometric measurements showed a deformation (P<0.05) only in the L1 segment of the Vertebrae Lumbales in Muay Thai athletes compared to sedentary group participants.
Perspective
It is believed that the biometric measurements and the 3-D images of Vertebrae Lumbales in Muay Thai athletes and other sportsmen would contribute to the appropriate therapeutic approach of orthopedists and neurologists by facilitating the diagnosis and analysis of pathologic formations (vertebral exocytose, vertebral inter-vertebral hernia etc.) of these bones. Furthermore, it is believed that the models rendered by this study would also contribute to the surgical interventions in case of serious injuries in Muay Thai athletes. Meanwhile, realistic vertebral models may be developed in light of the 3-D Vertebrae Lumbales data obtained from the sedentary group participants.
It was also expected that the method used in this study and the data acquired by means of this method would broaden the point of view and provide an innovative educational approach for the students of anatomy as well as to anatomic studies in the future. Furthermore, this study is believed to make a considerable contribution to the field of sports medicine.
CONFLICT OF INTERESTS
The author has not declared any conflict of interests.
REFERENCES
|
3D-Doctor 5.0. (2014).Copyright© 1998-2013 Able Software Corp. |
|
|
|
|
|
Antonio C, Stefano V, Ivo C, Raffaele M, Filippo T, Franco M and Alberto C (2009). Physiological rsponses and energy cost during a simulation of a Muay Thai boxing match, Applied Physiology, Nutrition Metabolism. 34(2):143-150. |
|
|
|
|
|
Baker RJ, Patel D (2005). Lower back pain in the athlete: common conditions and treatment. Pirim care. 32 (1):201-29. |
|
|
|
|
|
Barry A. Piorkowski, Adrian Lees & Gabor J. Barton (2011). Single maximal versus combination punch kinematics, Sports Biomechanics. 10(1):1–11. |
|
|
|
|
|
Bazille A, Guttman MA, McVeigh ER, Zerhouni EA (1994). Impact of semiautomated versus manual image segmentation errors on myocardial strain calculation by magnetic resonance tagging, Invest Radiology. 29:427–33. |
|
|
|
|
|
Gartland S, Malik MHA and Lovell ME (2001). Injury and injury rates in Muay Thai kick boxing, Br. J. Sports Med. 35:308–313. |
|
|
|
|
|
Hall RK (1994). The role of CT, MRI and 3D imaging in the diagnosis of temporomandibular joint and other or ofacial disorders in children. Australian Orthodontic J. 13:86–94. |
|
|
|
|
|
Hu H, He HD, Foley WD, Fox SH (2000). Four multidetector-row helical CT: image quality and volume coverage speed, Radiology. 215:55–62. |
|
|
|
|
|
Jeronimo JRS, Fabricio BDV, Luan MP, Monica YT and Emerson F (2011). Time-Motion analysis in Muay-Thai and Kick-Boxing amateur, J. Hum. Sport Exercıse. 6(3):490-496. |
|
|
|
|
|
Kalaycı İ (2008). 3D Reconstruction of phalangeal and metacarpal bones of male judo players and sedentary men by MDCT images. J. Sports Sci. Med. 7:544-548. |
|
|
|
|
|
Kalra MK, Maher MM, Toth TL, Hamberg LM, Blake MA, Shepard J, Saini S (2004). Strategies for CT radiation dose optimization, Radiology. 230 (3): 619-28. |
|
|
|
|
|
Krupa P, Krsek P, Cernochova P, Molitor M (2004). 3D real modelling and CT biomodels application in facial surgery. In: Neuroradiology European Society of Neuroradiology, ISBN 0028-3940. Berlin. 141. |
|
|
|
|
|
Pettersson U, Alfredson H, Nordström P, Henriksson K, Lorentzon R (1998). Bone mass in female cross-country skiers, reletionship between muscle strenth and different bmd sites. Sport Medicine Unit, Orthopaedics, Universtiy of Umea. 67: 199–206. |
|
|
|
|
|
Prokop M (2003). General principles of MDCT, Eur. J. Radiology. 45:4-10. |
|
|
|
|
|
Tony M, Nigel B (2012). The impact of crowd noise on officiating in MuayThai: achieving external validity in an experimental setting, Front. Psychol. 3:1-7. |
|
|
|
|
|
Tony M, Alan N, Yahya AN (2012). The Influence of Crowd Noise upon Judging Decisions in Muay Thai, Advances Physical Educ. 2(4):148-152. |
|
Copyright © 2024 Author(s) retain the copyright of this article.
This article is published under the terms of the Creative Commons Attribution License 4.0


